


Department of Dermatology, Venereology and Allergology, University Medical Center, Ruprecht-Karls-University, Im Neuenheimer Feld 440, DE-69120 Heidelberg, Germany. E-mail: julia.hartmann@med.uni-heidelberg.de
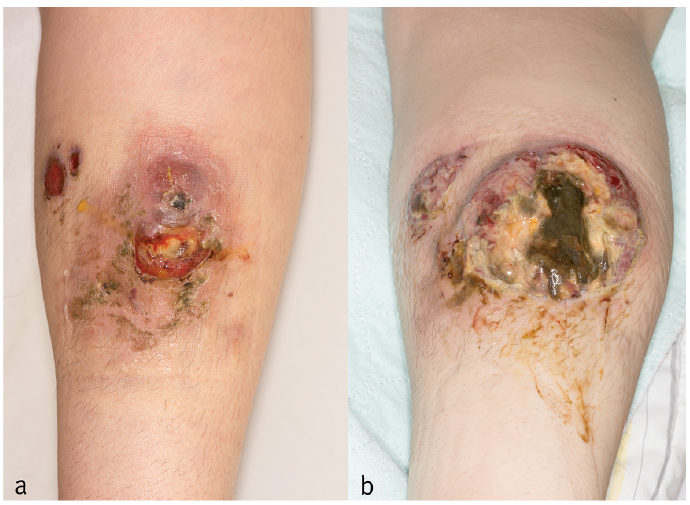
A 26-year-old woman presented with an 8-month history of a fast-growing, painful ulceration on her right lower leg (Fig. 1). The patient’s medical history included systemic lupus erythematosus (SLE), antiphospholipid syndrome, arterial hypertension, hypothyreosis and ovarian cysts. One year previously the patient had had a stroke and Libman-Sacks endocarditis. Her current medication included 100 mg azathioprine, 5 mg prednisone and 150 mg hydroxychloroquine per day, in addition to rivaroxaban.
Initially, the lesion had presented as a painful bluish discoloration with no epidermal involvement and had first been recognized by the patient as a bruise. The patient was referred to the department of surgery. Sonography and a magnetic resonance imaging (MRI) of her right lower leg were performed and the findings were compatible with an organized haematoma. Therefore the lesion was incised and drainage was inserted. Following this procedure a second smaller lesion developed where the drainage had been located. As neither lesion healed the patient was referred to our dermatology outpatient department.
What is your diagnosis? See next page for answer.
Fig. 1. (a) Lower right leg with 2 partially ulcerated lesions measuring approximately 3 cm and 6 cm in diameter. (b) Six weeks later the lesions measured approximately 4 cm and 10 cm in diameter, with a purulent exudate, slightly undermined borders and livid discoloration of the perilesional skin.
Acta Derm Venereol 2018; XX: XX–XX.
Diagnosis: Primary cutaneous CD30+ anaplastic large-cell lymphoma (CD30+ pcALCL)
A punch biopsy was performed and histopathology showed a dermal oedema, extravasation of red blood cells and an infiltrate consisting of histiocytes, lymphocytes and granulocytes. Furthermore, clusters of large, atypical, hyperchromatic blast-like cells were evident (Fig. 2a,b). The atypical cells showed a strong membranous positivity for CD30 (Fig. 2c) and were negative for anaplastic lymphoma kinase, S-100 protein and AE1/3. Molecular analysis did not show a monoclonal T-cell γ-gene rearrangement. A secondary cutaneous involvement by an extracutaneous lymphoma was ruled out by complete haematological staging (including complete blood count, serum protein electrophoresis and peripheral blood immunophenotyping by flow cytometry) and imaging studies (computed tomography of the trunk and abdomen, MRI of the skull, lymph node sonography). No bone marrow biopsy was performed due to its limited value in such cases (1).
Fig. 2. (a, b) Punch biopsy showing an infiltrate consisting of histiocytes, lymphocytes and granulocytes as well as clusters of large, atypical, hyperchromatic blast-like cells (haemtoxylin-eosin, original magnification ×200 and ×630 (oil immersion)). (c) Strong membranous positivity for CD30 (original magnification ×200).
In the present case approximately 9 months passed between the initial symptoms and final diagnosis due to the changing clinical presentation. Initially the lesion was diagnosed as a haematoma, as the patient took anticoagulants. In the further course an ulceration developed and a second lesion appeared at the site of surgical intervention, suggestive of a pathergy phenomenon. As the lesions were painful pyoderma gangrenosum (PG) was considered as a differential diagnosis. PG in patients with lupus erythematodes is a well-described phenomenon (2). As the patient was immunosuppressed and the lesion showed a purulent exudate an infectious aetiology also seemed plausible. Nevertheless, microbial swabs and special stains (Giemsa, PAS, Ziehl-Neelson) were inconspicuous. Despite the patient’s young age, a malignancy with seeding caused by drainage was considered as a differential. Given a lower cell-to-cell adhesion in cancer cells, iatrogenic interventions, such as drains or fine needle aspiration, might cause cutaneous metastasis, mostly at postoperative drain sites in patients with abdominal or pulmonal malignancies (3, 4). In primary cutaneous CD30+ anaplastic large-cell lymphoma this phenomenon has not been described previously.
Patients with SLE are at increased risk of developing lymphomas in general (5), and T-cell lymphomas in particular (6). Histopathology in the present case revealed a dense inflammatory infiltrate masking the lymphoma cells; a phenomenon that is seen in pyogenic variants of ALCL (7), whereas in non-pyogenic ALCL lymphoma cells are accompanied by only a small number of reactive cells (8).
CD30+pcALCL generally has a favourable prognosis with a 5-year survival rate of >90% and spontaneous resolution in approximately 25% of patients (9, 10), therefore a watch-and-wait approach might be reasonable. Nevertheless, in patients with extensive limb disease (multiple lesions on the leg) the 5-year survival rate is much lower, at only 50% (11). In addition, a more rapid progression is seen, as well as significantly lower clinically complete response rates and less durable response (11, 12). The immunosuppressive medication was an additional risk factor in our patient. Several case series have described the poor prognosis of primary cutaneous T-cell lymphomas (including CD30+pcALCL) in patients receiving immunosuppressive treatment with varying combinations of azathioprine, cyclosporine and steroids after organ transplantation (13, 14).
The rapid progression and atypical/changing clinical presentation in this case might be explained by the patient’s underlying autoimmune disorder and the immunosuppressive medication.
In summary, the present case underlines the need to consider CD30+pcALCL as a differential diagnosis in atypical leg ulcers, as well as the importance of clinicopathological correlation, especially in immunosuppressed patients.


 Click to show fullsize
Click to show fullsize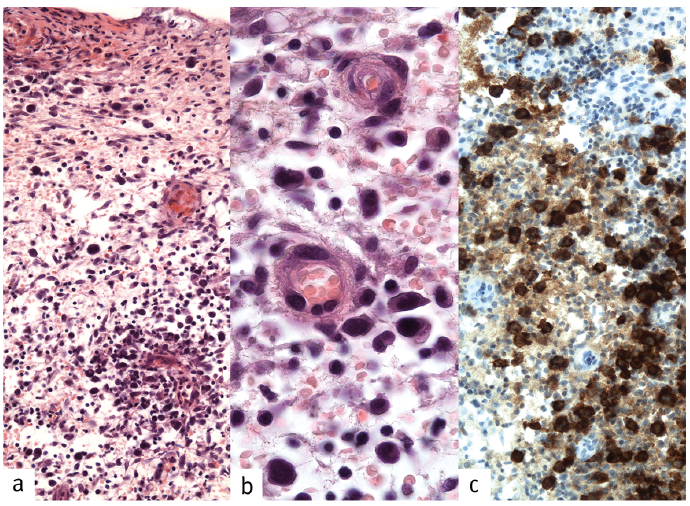 Click to show fullsize
Click to show fullsize