


1Department of Dermatology and Allergy, Herlev and Gentofte Hospital, University of Copenhagen, Hellerup, 2Department of Immunology and Microbiology, Faculty of Health and Medical Sciences, University of Copenhagen, Copenhagen, Denmark
This study investigated serum 25-hydroxyvitamin D (25(OH)D) concentrations and circulating regulatory T cells in patients with atopic dermatitis receiving narrow-band ultraviolet B (nbUVB) phototherapy. Thirty adult patients with atopic dermatitis were included. Blood samples were collected at baseline and at weeks 2 and 4 of nbUVB phototherapy. Skin biopsies were taken at baseline and at week 4. Serum 25(OH)D concentrations increased significantly following nbUVB phototherapy (estimate of change from baseline to week 2: 32.00 nmol/l, confidence interval (CI) 20.48–43.52, p < 0.0001, n = 25; and from baseline to week 4: 50.30 nmol/l, CI 37.28–63.33, p < 0.0001, n = 18). This increase was independent of the filaggrin gene loss-of-function mutation status. Flow cytometry showed no significant change in regulatory T cells or cytokine profiles of T cells in blood. Real-time quantitative PCR showed no change in skin cytokine levels. In conclusion, nbUVB phototherapy was associated with increased serum 25(OH)D concentrations, but not changes in circulating regulatory T cells in patients with atopic dermatitis.
Key words: nbUVB phototherapy; atopic dermatitis; 25-hydroxy-vitamin D; regulatory T cells, filaggrin.
Accepted Sep 23, 2018; Epub ahead of print Sep 24, 2018
Acta Derm Venereol 2018; XX: XX–XX.
Corr: Stine Simonsen, Department of Dermatology and Allergy, Herlev and Gentofte Hospital, University of Copenhagen, Kildegårdsvej 28, DK-2900 Hellerup, Denmark. E-mail: stine.simonsen.01@regionh.dk
Vitamin D synthesis is induced by ultraviolet B irradiation of the skin and may have a beneficial effect on the immune system in patients with atopic dermatitis. We measured changes in vitamin D levels and immunological markers in patients with atopic dermatitis receiving ultraviolet B photo-therapy. Following ultraviolet B phototherapy, vitamin D levels were increased, as expected, but no changes were found in the immune system. Furthermore, ultraviolet B phototherapy induced equal increases in the vitamin D levels in patients with atopic dermatitis with and without a mutation that causes a defective skin barrier.
Narrow-band ultraviolet B (nbUVB) phototherapy is an established treatment for atopic dermatitis (AD) (1). AD is a complex trait characterized by a dysfunctional skin barrier and a pathological immune polarization. Although different endotypes may exist, AD is characterized by a strong activation of TH2 immune responses in lesional and non-lesional skin, with some contribution from the TH22, TH17/IL-23, and TH1 cytokine pathways (2). Regulatory T cells are pivotal for maintenance of self-tolerance and probably also for the regulation of unwanted immune activation, such as in atopy (3). However, the role of regulatory T cells in the pathogenesis of AD is not fully understood. Several studies have suggested that patients with AD have increased levels of circulating regulatory T cells compared with healthy controls, although the data are conflicting (4–8). Vitamin D is central for immune function (9). Notably, vitamin D levels may be associated with the risk and severity of AD, and a few small studies have shown that vitamin D supplementation may reduce the clinical severity of AD (10). A recent study has investigated circulating regulatory T cells and serum 25-hydroxyvitamin D (25(OH)D) concentration in a group of patients with different inflammatory skin diseases who were undergoing nbUVB phototherapy (11). The authors showed that the numbers of regulatory T cells increased mainly in the first 14 days of nbUVB phototherapy, and that there was a correlation between this increase and an increase in serum 25(OH)D concentration.
Loss-of-function mutations in the filaggrin gene, FLG, result in a complete or partial lack of monomeric filaggrin in the epidermis, and are a strong risk factor for AD (12). Filaggrin is metabolized to amino acids and their derivatives, which constitute a major part of the natural moisturizing factors in the upper layers of the stratum corneum. One important metabolite is trans-urocanic acid (trans-UCA), a key UVB photon-absorbing chromophore of the epidermis (13). In vitro and animal studies have suggested that decreased levels of trans-UCA result in increased keratinocyte UVB photosensitivity (14–18). A meta-analysis of cross-sectional studies has shown that subjects with FLG loss-of-function mutations have a 10% higher concentration of serum 25(OH)D concentration than wild-type (WT) subjects (19). Based on these observations, one may hypothesize that FLG loss-of-function mutations cause increased epidermal penetration of UVB photons and thereby increased 25(OH)D synthesis. This study investigated changes in serum 25(OH)D concentration and circulating regulatory T cells in the early stage of nbUVB phototherapy in a group of patients with AD. The study also examined changes in the cytokine profiles of circulating T cells and cytokine levels in the skin. Furthermore, the study examined differences between patients with AD who had or did not have FLG loss-of-function mutations, in nbUVB-induced changes in serum 25(OH)D concentration and in circulating regulatory T cells.
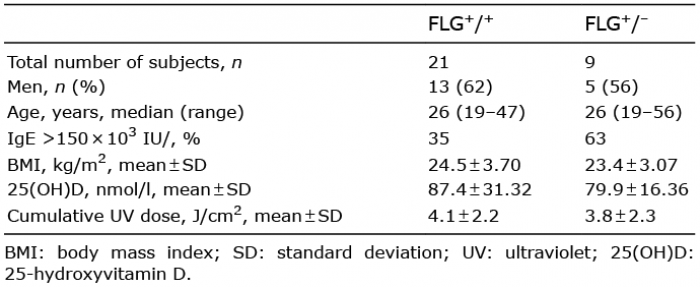
The study was approved by the local ethics committee of the Capital Region of Denmark (no. H-4-2014-037) and the Danish Data Protection Agency. Written informed consent was obtained from all patients before inclusion, and the study was performed according to the Declaration of Helsinki. Enrolled patients had been diagnosed with AD, were of Northern European descent, and were 18 years old or more. All patients were planned to start nbUVB phototherapy as part of their treatment for AD. Recruitment was accomplished from dermatological outpatient clinics and dermatological practitioner clinics in the Capital Region of Denmark between February and April 2015 and between September and April in the period 2015 to 2017. The season of the study was chosen to minimize UVB-induced 25(OH)D synthesis by exposure to sunlight. The nbUVB phototherapy was given as whole-body exposure, starting at 0.05 J/cm2 to 0.41 J/cm2 depending on skin type and gradually increasing by 0.05–0.2 J/cm2 per treatment. NbUVB phototherapy was scheduled 3 times a week. If patients had attended fewer than 3 nbUVB treatments between study visits, they were excluded from the rest of the study. For information on machines and light sources, see Table SI. The patients were instructed not to take vitamin D supplements during the study period and were allowed to use topical therapy (steroids and calcineurin inhibitors) on minor skin areas if necessary. All patients started treatment immediately after control by a dermatologist due to eczema activity or flare up. The age, body mass index (BMI), and sex of the patients were recorded (Table I). Cumulative doses were also recorded (Table I).
Table I. Demographics and baseline data
The study comprised 3 visits: within hours before the first session of nbUVB phototherapy (baseline), after 2 weeks of nbUVB phototherapy (week 2), and after 4 weeks of nbUVB phototherapy (week 4). Blood samples were obtained at all study visits. At baseline, total IgE and the presence of the 3 most common FLG mutations in Europe were determined. At all study visits, blood was analysed for serum 25(OH)D concentration and was directly analysed for regulatory T cells and intracellular cytokine expression by flow cytometry, as described below. In patients who agreed to the taking of biopsies, skin biopsies (4 mm in diameter) were taken under local anaesthesia from lesional skin at baseline, and at approximately the same location at week 4 of nbUVB photo-therapy. All biopsies were used for real-time quantitative polymerase chain reaction (RT qPCR) analysis.
Serum 25(OH)D concentration was determined as the sum of the concentrations of 25-hydroxyvitamin D2 and 25-hydroxyvitamin D3 determined with a competing antibody immunoassay system (Advia Centaur; Siemens, New York, NY, USA). Plasma IgE concentration was determined with a sandwich immunoassay system (Advia Centaur; Siemens). FLG loss-of-function mutations (R501X, 2282del4, and R2447X) were determined by PCR technique (20). All analyses were performed at the Department of Clinical Biochemistry, Herlev and Gentofte Hospital, Hellerup, Denmark.
Peripheral blood mononuclear cells (PBMCs) were isolated by density gradient centrifugation (Lymphoprep; Fresenius Kabi, Oslo, Norway). Cells were counted and used for two separate intracellular staining procedures: FoxP3 and intracellular cytokines.
Cells (2×107/ml) were plated and immediately stained with the following antibodies from BD Biosciences (San Jose, CA, USA): anti-CD3-FITC (561806), anti-CD4-AF700 (557922), anti-CD25-PE-Cy7 (557741), anti-CD45RA-BV711 (563733), and anti-CD45RO-BV786 (56429). Brilliant Stain Buffer (563794; BD Biosciences) was added to the antibody cocktail. Then the cells were fixed and permeabilized with the Transcription Factor Buffer Set (562574; BD Biosciences) according to the manufacturer’s protocol. Finally, they were stained with anti-FoxP3-AF647 (560045).
Cells (107/ml) were plated and incubated at 37°C in an atmosphere of 5% CO2 for 5 h in RPMI-1640 (Sigma-Aldrich, Steinheim, Germany) with penicillin-streptomycin (Sigma-Aldrich), L-glutamine (Sigma-Aldrich), and foetal bovine serum (Sigma-Aldrich) in the presence of 50 ng/ml phorbol 12-myrisate 13-acetate (Sigma-Aldrich), 250 ng/ml ionomycin (Sigma-Aldrich), and 2 μg/ml monensin (Sigma-Aldrich). Thereafter, the cells were immediately stained with the following antibodies from BD Biosciences: anti-CD3-BV650 (563852), anti-CD4-AF700 (557922), and anti-CD8-APC-H7 (560179). Next, they were fixed and permeabilized according to the manufacturer’s protocol (Permeabilization Buffer 00-8333-56, Fixation/Permeabilization Diluent 00-5223-56, and Fixation/Permeabilization Concentrate 00-5123-43; eBioscience, San Diego, CA, USA). Finally, the cells were stained with the following antibodies: anti-IL5-PE (554395; BD Biosciences), anti-IL10-BV421 (564053; BD Biosciences), anti-IL17-BV510 (563295; BD Biosciences), anti-IL22-PerCP eFluor (710 46-7229-42; eBioscience), and anti-interferon (IFN)-γ-BV488 (557718; BD Biosciences). Brilliant Stain Buffer was added to the antibody cocktail.
Skin biopsies were frozen immediately in liquid nitrogen and stored at −80°C until RNA purification. RNA extraction, cDNA synthesis, and RT qPCR analysis were performed by AROS Applied Biotechnology A/S, Aarhus, Denmark. Skin biopsies from baseline and week 4 of nbUVB phototherapy were used for RNA extraction. Total cellular RNA was extracted and purified from tissue samples using the automated process on a QIAsymphony SP robot using the QIAsymphony RNA kit (QIAGEN, Hilden, Germany). cDNA synthesis was undertaken using the High-Capacity cDNA Reverse Transcription Kit (Applied Biosystems; ThermoFisher Scientific, Waltham, MA, USA) using 100 ng RNA. A specific target amplification was performed using a pool of the PCR assays IL-4: Hs00174122_m1; IL-5: Hs01548712_g1; IL-10: Hs00961622_m1; IL-13: Hs00174379_m1; IL-17: Hs00174383_m1; IL-22: Hs01574154_m1; IL-33: Hs04931857_m1; IFN-γ: Hs00989291_m1; PGK1: Hs00943178_g1; and SDHA: Hs00188166_m1 (TaqMan; ThermoFisher Scientific), which were also used in the subsequent qPCR. The pre-amplified cDNA and the assays were loaded on a 48×48 dynamic array and run under standard conditions on the Fluidigm BioMark system according to the manufacturer’s protocol. Data were analysed using Fluidigm BioMark software version 4.1.3 with linear (derivative) baseline correction and the user (detectors) method for Ct threshold settings. Mean Ct values were calculated from the raw data along with assay standard curve linearity and amplification efficiency.
NbUVB phototherapy-induced changes and interaction between nbUVB phototherapy and mutation were tested with a mixed-effect model and analysis of variance (ANOVA). Paired t-test was used to compare baseline values between FLG heterozygous and WT patients. RT qPCR data were assessed with paired Wilcoxon matched-pairs signed rank test. Statistical significance was assumed at p-values less than 0.05. All analyses were performed with RStudio, version 0.99.902 (RStudio Inc., Boston, MA, USA).
A total of 36 patients were screened, and 30 were included in the study. Baseline data for the included patients are given in Table I. Three patients dropped out after baseline sampling. Two patients were excluded at week 2, and 6 were excluded at week 4 due to having less than 3 nbUVB treatments between study visits (Fig. S1). Of the patients who entered the study, 9 were heterozygous for FLG mutation. None of the patients were homozygous or compound-heterozygous for FLG mutation. Total IgE was elevated (>150×103 IU/l) in 56% of FLG heterozygous patients and in 32% of WT patients.
At baseline, the overall mean ± SD 25(OH)D serum concentration was 85.13 ± 27.62 nmol/l (n = 30). There was no significant difference between FLG heterozygous patients and WT patients (p = 0.51, nWT=21, nheterozygous=9) (Table I). 25(OH)D concentration above 50 nmol/l was defined as sufficient. Only 3 patients had a 25(OH)D concentration below 50 nmol/l at baseline. NbUVB phototherapy led to a significant increase in 25(OH)D concentration at both study visits compared with baseline (pWeek 2 < 0.0001, n = 25; pWeek 4 < 0.0001; n = 18). The mean ± SD increase in 25(OH)D concentration between baseline and week 2 was 31.20 ± 26.48 nmol/l and the mean increase between week 2 and week 4 was 20.00 ± 27.97 nmol/l (Fig. 1). No significant effect of FLG mutations on increase in 25(OH)D concentration was found (Table II). Regulatory T cells were measured as the percentage of CD25+FoxP3+ cells in CD4+ cells (Fig. 1). The baseline proportion of regulatory T cells was not significantly different between FLG heterozygous patients and WT patients (meanWT ± SD = 5.28% of CD4+ ± 2.38, meanheterozygous ± SD=5.87% of CD4+ ± 3.53; p = 0.63, nWT=18, nheterozygous=8). Overall, there was no change in the proportion of regulatory T cells at week 2 (p = 0.11, n = 24) or at week 4 (p = 0.97, n = 18) and we found no significant effect of FLG mutation on the proportion of circulating regulatory T cells following nbUVB phototherapy using mixed-effect model analysis (pWeek 2= 0.10, n = 24; pWeek4= 0.88, n = 18).
Fig. 1. Serum 25(OH)D concentration is increased by ultraviolet B (UVB) phototherapy, but circulating regulatory T cell proportion is not. 25-hydroxyvitamin D concentration was measured in blood by a competing antibody immunoassay system, while regulatory T cells were evaluated by flow cytometry of fresh blood samples. FLG+/+: FLG wild-type subjects; FLG+/–: FLG heterozygous subjects; 25(OH)D: 25-hydroxyvitamin D; % CD25+FoxP3+: % CD25+FoxP3+ cells in CD4+ cells. Open squares represent mean values. (A) and (B): serum 25(OH)D concentration; (C) and (D): % CD25+FoxP3+ of CD4+ T cells.
Table II. Summary of mixed-effect model analysis
Intracellular cytokine profiles of circulating CD4+ cells from PBMCs were evaluated with flow cytometry at baseline, at week 2, and at week 4 following nbUVB phototherapy. No overall change was found in the proportions of CD4+IL-5+ cells, CD4+IL-10+ cells, CD4+IFN-γ+ cells, CD4+IL-17+ cells, or CD4+IL-22+ cells during nbUVB phototherapy (Table II and Fig. 2), but CD4+IL-22+ cells were borderline significantly increased (p = 0.05). Furthermore, there was no significant effect of FLG mutation status on the phenotype of CD4+ T cells as determined by intracellular cytokine expression. The proportions of CD45RA+ cells and CD45RO+ cells in circulating CD4+ cells from PBMCs were not significantly changed during nbUVB phototherapy (Table II), and no significant effect of FLG mutation status on the number of CD45RA+ cells and CD45RO+ cells was found. Skin biopsies from baseline and at week 4 of nbUVB phototherapy were analysed with RT qPCR for selected cytokine mRNA. This showed no change in IL-10, IL-13, IL-22, IL-33, or IFN-γ mRNA following nbUVB phototherapy (Table SII) (n = 6 or n = 5). This part of the study included too few patients to make comparisons between patients with and without FLG loss-of-function mutations. IL-4, IL-5, and IL-17 mRNA were detected in only a few biopsies.
Fig. 2. Intracellular cytokine levels are not changed during ultraviolet B (UVB) phototherapy. Peripheral blood mononuclear cells were isolated from fresh blood samples, stained intracellularly, and analysed with flow cytometry. FLG+/+: FLG wild-type subjects; FLG+/–: FLG heterozygous subjects. Cytokines are given as the percentage of cytokine-positive CD4+ cells in total CD4+ cells. Open squares represent mean values. (A) and (B): CD4+IFN-γ+; (C) and (D): CD4+IL-5+; (E) and (F): CD4+IL-17+; (G) and (H): CD4+IL-22+; (I) and (J): CD4+IL-10+.
Adult patients with AD showed an increase in serum 25(OH)D concentration during nbUVB phototherapy. FLG loss-of-function mutations had no significant effect on this increase. No increase in circulating regulatory T cell levels was detected during nbUVB phototherapy in patients with AD.
The finding of a significant increase in serum 25(OH)D concentration during nbUVB phototherapy is in line with previous studies that have investigated AD patients alone or a group of patients with various skin disorders (11, 21–26). The lack of effect of FLG loss-of-function mutations on this increase contrasts with epidemiological and experimental studies that have indicated that decreased filaggrin levels in the skin cause higher nbUVB penetration (14–19). In keeping with a possible greater nbUVB penetration caused by filaggrin deficiency, a recent study investigating patients with irritant contact dermatitis of the hands found that the increase in serum 25(OH)D concentration after nbUVB irradiation was inversely correlated with the baseline levels of trans-UCA in epidermal interstitial fluid (27). However, neither baseline levels of trans-UCA nor FLG mutation status had an effect on UVB-induced changes in cytokines in epidermal interstitial fluid (27). In agreement with our study, minimal erythema dose has been shown to be similar in FLG heterozygous and WT subjects (28). In addition, levels of filaggrin degradation products are influenced by disease severity as well as FLG status (29), and both filaggrin mRNA and protein levels can be suppressed by various inflammatory cytokines (30). The lack of effect of FLG loss-of-function mutations may therefore also be explained by insignificant differences in trans-UCA levels in the epidermis between patients with AD who have and do not have FLG loss-of-function mutations, minimizing the difference in penetration of UVB photons.
Milliken et al. (11) showed that the mean proportion of circulating regulatory T cells increased significantly at week 2 of nbUVB phototherapy in a group of patients with different inflammatory skin diseases. Similarly to Milliken et al. the current study examined the early UVB-induced changes in the blood and the effect of the first 4 weeks of UVB treatment. The results suggest that this does not apply to a group of patients with AD only. In contrast to our data, a recent study from Egypt (31) showed that numbers of circulating regulatory T cells were increased significantly after 6 weeks of nbUVB phototherapy in AD patients, but the authors did not assess FLG genotype. Comparisons with our study should be made with caution, because the study from Egypt was based on patients with more severe disease, different ethnicity, and different time points of follow-up.
In keeping with our findings, it has been shown recently that there is no difference in circulating regulatory T cells between patients with AD who have and do not have FLG loss-of-function mutations (32).
Several studies have shown differences in intracellular cytokines or serum cytokine levels in patients with AD and in healthy control subjects (6, 33–36). The present study did not compare cytokine values with those in healthy controls. Our group has previously shown a higher number of Th17 cells in AD patients with FLG loss-of-function mutations than in AD patients without these mutations (37). In this study, both compound-heterozygous patients and homozygous AD patients were included. To our knowledge, no previous study has investigated changes in cytokine profiles in circulating T cells in patients with AD who are undergoing nbUVB phototherapy. Our data do not suggest that nbUVB phototherapy has any influence on cytokine profiles in blood in the first 4 weeks of treatment; nor did we find any significant changes in IL-10, IL-13, IL-22, IL-33, or IFN-γ mRNA expression in biopsies from lesional AD skin at week 4 following nbUVB phototherapy compared with pretreatment. In previous studies, IL-10, IL-13, IL-22, and IFN-y expression in skin from patients with AD has been shown to be significantly elevated (36, 38, 39). Twelve weeks of nbUVB phototherapy has been shown to be associated with decreased levels of IL-10, IL-13, IL-22, IL-17A, and IFN-γ mRNA in the skin of patients with AD. However, at this time point the skin is well treated and the data therefore cannot be compared with the data from our study.
This study is the first to investigate 25(OH)D serum concentrations and the proportion of circulating regulatory T cells during nbUVB phototherapy exclusively in patients with AD. The aim was to examine the initial changes in 25(OH)D serum concentration and immune markers in the blood and skin, and not clinical outcomes. One strength of the present study is that it did not examine a selected group based on clinical severity or baseline serum 25(OH)D concentration. The findings are therefore likely to represent real-life data.
The study has several limitations. Only one patient with severe disease was included. In addition, we were only able to include a limited number of patients with FLG loss-of-function mutations and no FLG homozygous patients were included. A difference in 25(OH)D serum concentration between patients with and patients with-out FLG loss-of-function mutations might have been more easily detectable if baseline mean serum 25(OH)D had been insufficient. Furthermore, it is possible that immune function does not benefit from increases in vitamin D levels if the baseline concentration is sufficient. The baseline serum 25(OH)D concentration in our study population is higher than that found in the Danish background population in a study 6 years ago (40).This may be explained by increased public awareness about the risk of vitamin D insufficiency, and thus increased use of supplements.
Human data suggest that the vast majority of circulating regulatory T cells express skin homing receptors (41). Future studies are needed to investigate the effect of nbUVB on the proportion of circulating regulatory T cells that express skin homing receptors in patients with AD.
In conclusion, this study confirms that there is an increase in serum 25(OH)D concentration after nbUVB phototherapy in patients with AD. This study did not find any evidence of increased vitamin D synthesis in AD patients with FLG loss-of-function mutations. The data did not show any overall effect of phototherapy on the proportion of circulating regulatory T cells in patients with AD, either in those with or in those without FLG mutations.
This work was supported by grants from the Capital Region of Denmark Foundation for Health Research and from the Aage Bang Foundation. Stine Simonsen was supported by a grant from the University of Copenhagen. The authors thank all the patients who volunteered for the study, and all the doctors and nurses at the Department of Skin and Allergy, Gentofte Hospital, who helped to recruit patients. The authors also thank Anne Danielsen, Mads Nielsen, Gitte Strauss, David Mølenberg, Elisabeth Ammitzbøll Holm, Eva Due, and Lene Overgaard and their staff who helped to recruit patients from dermatological practitioner clinics and kindly let us use their facilities.
Disclosures: LS has received consultancy and/or speaker honoraria from Abbvie, Pfizer, Janssen-Cilag, Novartis, and Leo Pharma and is a member of the advisory boards of Abbvie, Sanofi, Pfizer, Leo Pharma, Janssen-Cilag, Eli Lilly, Orion, Celgene, Admirall and Novartis. The other authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize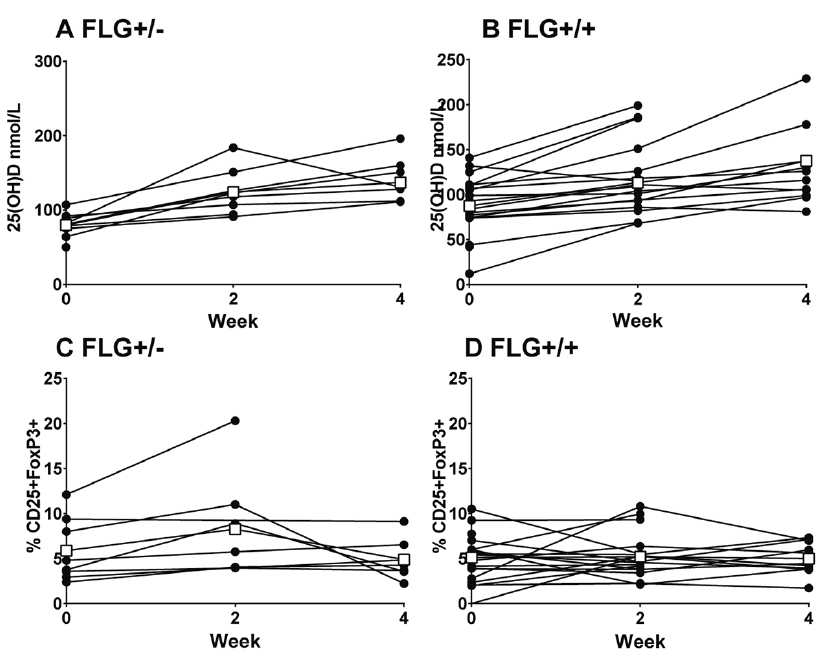 Click to show fullsize
Click to show fullsize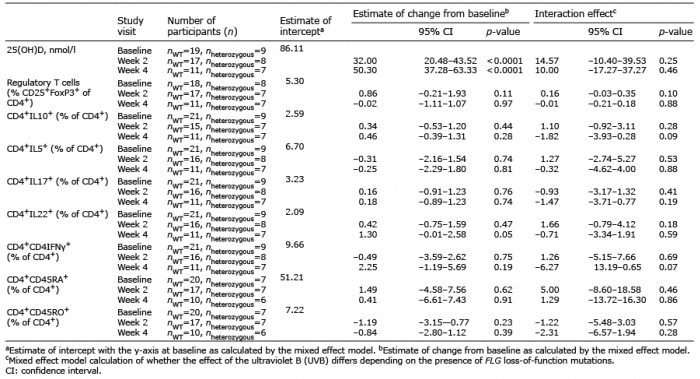 Click to show fullsize
Click to show fullsize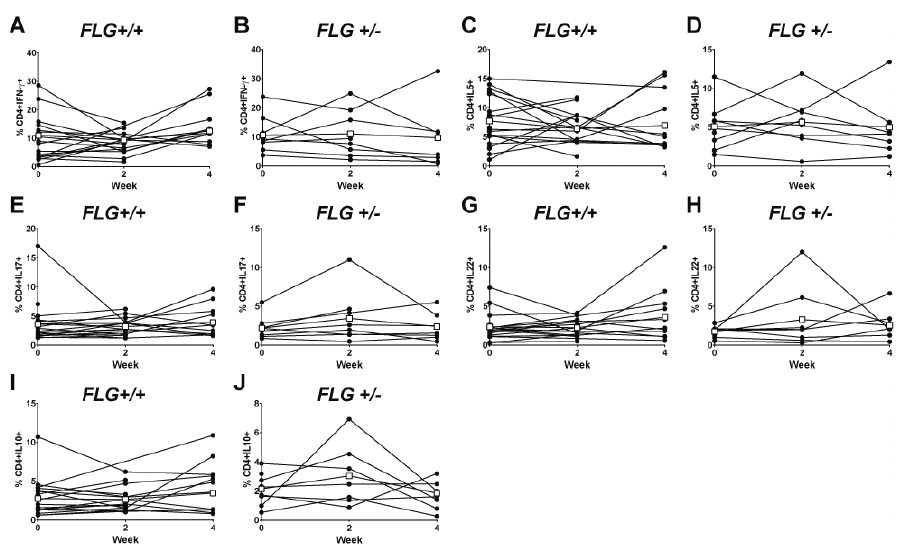 Click to show fullsize
Click to show fullsize