


1Department of Dermatology, University Hospital and University of Franche Comté, EA3181, 3 Bd Fleming, FR-25030 Besançon, 2Department of Neurology, and 3Department of Ear, Nose and Throat, University Hospital, Besançon, France. E-mail: francois.aubin@univ-fcomte.fr
Accepted Oct 3, 2018; Epub ahead of print Oct 3, 2018
Paraneoplastic opsoclonus-myoclonus syndrome (POMS) is most commonly associated with neuroblastoma in children, but it also occurs with a variety of neoplasms in adults, particularly small-cell lung cancer and breast cancer (1). We report here a case of POMS that led to the finding of a non-metastatic mucosal melanoma.
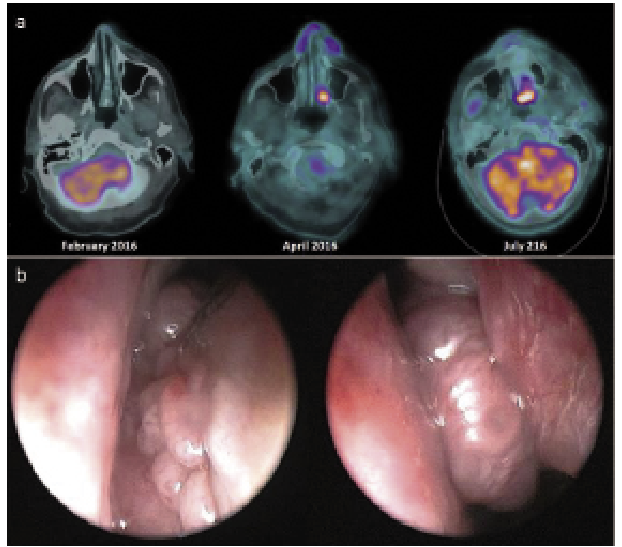
A 69-year-old man was admitted to the emergency unit for subacute and intense dizziness, associated with nausea and vomiting. Physical examination revealed vertigo with truncal and limb ataxia, in relation to a cerebellar syndrome, orthostatic myoclonic jerks and characterized arrhythmic, multidirectional, continuous involuntary eye movements (even during sleeping) consistent with opsoclonus. Further examinations, including laboratory investigations (autoimmune tests), cerebrospinal fluid analysis, serological tests for HIV, hepatitis B, C and Lyme’s disease, neuronal antibodies in blood and cerebrospinal fluid, radiological investigations (chest X-ray, abdominal and pelvis computed tomography (CT) scan, positron emission tomography (PET) scan, brain magnetic resonance imaging (MRI)) and functional tests (videonystagmography, audiometry) were normal. Based on these data, the diagnosis of post-infectious opsoclonus-myoclonus syndrome was initially made and the patient was treated with monthly intravenous immunoglobulins (IVIG). No improvement was observed after 4 months, therefore the investigations were repeated. Although the nasal endoscopy was normal, the PET scan now showed a positive uptake in the left nasal cavity. Brain MRI was normal. Systemic corticosteroids were added to IVIG. Two months later, the patient presented with worsening of the neurological syndrome, including an increase in opsoclonus and cerebellar ataxia, and the appearance of a confusional state and dysarthria, responsible for a major loss of autonomy. A new PET scan was performed and confirmed an increase in the uptake previously observed in the left nasal cavity (Fig. 1a). Brain scan was normal. Nasal endoscopy finally demonstrated a friable bleeding lesion under the left inferior turbinate and inside the middle turbinate (Fig. 1b). Pathological examination confirmed a locally advanced malignant melanoma. Surgical resection was performed, but was incomplete. The patient progressed to coma within 2 weeks and died 8 months after the onset of neurological symptoms due to complications associated with the POMS (aspiration pneumonia).
Fig. 1. (a) Increase in uptake in repeated fluorodeoxyglucose postitron emission tomography/ computed tomography (FDG PET/CT) during follow-up. (b) Nasal endoscopy: mucosal melanoma in the left nasal cavity.
Neurological paraneoplastic syndromes, including melanoma-associated retinopathy (1), dermatomyositis (2) and POMS are uncommon in patients with melanoma. POMS is most commonly associated with neuroblastoma in children, but it also occurs with a variety of neoplasms in adults, particularly small-cell lung cancer and breast cancer (3). To our knowledge, only 3 melanoma-associated POMS have been reported (4–6).
Opsoclonus is defined by the presence of spontaneous, arrhythmic and large amplitude conjugate saccades occurring in all directions of gaze, without saccadic interval. Opsoclonus is usually associated with myoclonus of the limbs and trunk, and sometimes, with encephalopathy. POMS is observed in 3 clinical settings (3): (i) paediatric patients with neuroblastoma; (ii) adult female patients with Ri-Ab, whose underlying tumour is usually breast cancer; and (iii) adult patients whose tumour is almost always small-cell lung carcinoma. There are individual case reports associated with other tumours.
The pathophysiology of the POMS is not well-known. The clinical differences observed between POMS and idiopathic opsoclonus-myoclonus suggest different mechanisms according to the trigger agent. POMS is believed to be the result of an autoimmune response provoked by molecular mimicry between the tumour and a distinct group of central nervous system neurones (7, 8). However, the absence of antineuronal antibodies is not unusual, as demonstrated in a substantial number of patients (8), in particular in previously reported melanoma-associated POMS (4–6).
It is notable that, among the 4 reported melanoma-associated POMS, 3 were associated with mucosal melanoma (5, 6, our case). We do not have any clear explanation for this specific association. Our case is original, since unlike the other cases of POMS linked to a melanoma previously diagnosed, the POMS clearly preceded clinical diagnosis of the melanoma and occurred in the context of a locally advanced, but non-metastatic, cancer.
The authors thank Elisabeth Homassel for her technical assistance.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize