


1Department of Dermatology, 2Division of Skin Surface Sensing, 4Department of Medicine and Biosystemic Science and 5Department of Medicine and Bioregulatory Science, Graduate School of Medical Sciences, Kyushu University, 3-1-1 Maidashi, Higashi-ku, Fukuoka 812-8582, 3Department of General Internal Medicine, Kyushu University Hospital, 6Kyushu General Internal Medicine Center, Haradoi Hospital, and 7Department of Internal Medicine, Fukuoka City Hospital, Fukuoka, Japan. E-mail: macky@med.dermatol.med.kyushu-u.ac.jp
Accepted Oct 11, 2018; Epub ahead of print Oct 11, 2018
Many patients with chronic liver disease develop pruritus with or without skin lesions. The prevalence of pruritus in patients with primary biliary cholangitis (PBC) has been reported to be especially high, at around 70% (1, 2). How-ever, the prevalence of pruritus in patients with chronic hepatitis C varies, depending on the study, with reported values ranging from 5.1% to 58.4% (3–6). Moreover, the prevalence of pruritus in patients with other chronic liver diseases, such as chronic hepatitis B, autoimmune hepatitis (AIH), non-alcoholic fatty liver disease (NAFLD), alcoholic liver disease (ALD), liver cirrhosis, and hepatocellular carcinoma (HCC), has hardly been reported.
Pruritus causes both physical and mental stress and affects the quality of life of the afflicted patients. To better understand the current status of pruritus, we assessed its prevalence and intensity in patients with chronic liver diseases by performing a questionnaire survey on 216 patients.
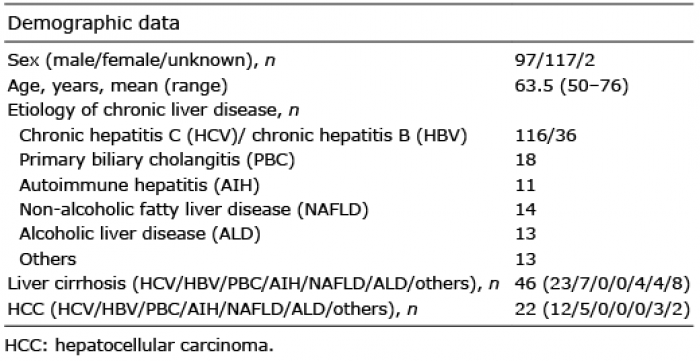
A total of 216 patients who visited departments of internal medicine at our 3 general hospitals for the diagnosis and treatment of chronic liver disease from September 2015 to March 2016 were recruited in this study. The patients’ characteristics and diagnoses are summarized in Table I. A total of 49 patients were treated for pruritus by antipruritic agents, of whom 59.2% received them only externally, 10.2% received them only orally, and 26.5% received them both externally and orally. Data were not available for two cases.
Table I. Profile of 216 patients with chronic liver disease
We asked the patients to complete a questionnaire (Appendix S1) when they visited our departments in the daytime. In the questionnaire, the patients were asked about the occurrence of pruritus and its intensity in the daytime and at night within a 24-h period using a visual analog scale (VAS) and verbal rating scale (VRS). The VAS involves a 10-cm-long horizontal line, the beginning of which represents “no itch” (0 mm) and the end of which represents “worst imaginable itch” (100 mm), on which patients indicate the intensity of pruritus by crossing the line at the point corresponding to the severity of their pruritus. The VRS consists of a list of phrases that describe increasing levels of pruritus intensity: no pruritus, mild pruritus, moderate pruritus, severe pruritus, and very severe pruritus. This study was approved by the local ethics committees of Kyushu University.
Mean values and standard errors were calculated. Where appropriate, the following tests were used: Student’s t-test, χ2 test, and one-way analysis of variance (ANOVA) with Bonferroni’s post hoc test or Dunnett’s post hoc test. In this study, p-values < 0.05 were considered statistically significant. All data were analyzed using Microsoft Excel 2012 (Microsoft Corporation) or GraphPad Prism 5 (GraphPad Software).
The prevalence of pruritus according to the underlying liver disease is summarized in Fig. 1. In the present study, 41.2% of the patients suffered from pruritus (Fig. 1). Those with PBC (72.2%), AIH (54.5%), and liver cirrhosis (54.3%) showed a relatively high prevalence of pruritus, whereas those with chronic hepatitis B (24.3%) and NAFLD (14.3%) showed a lower prevalence. The prevalence rates of pruritus in those with chronic hepatitis C, ALD, and HCC were 44.4%, 38.5% and 36.4%, respectively. In patients with hepatitis C, pruritus was more frequently detected in those with liver cirrhosis (65.2%) than in those without it (39.6%) (χ2 test: p < 0.01). In contrast, there was no significant difference in the prevalence of pruritus between the hepatitis B patients with liver cirrhosis (42.9%) and those without it (21.4%) (Fig. 1b, c).
Fig. 1. (a) Prevalence of pruritus in 216 patients with different chronic liver diseases. The black bar shows the overall prevalence of pruritus in the patients. (b, c) Prevalence of pruritus in patients with hepatitis C (HCV) (b) and hepatitis B (HBV) (c) with or without liver cirrhosis. The black and white columns show the numbers of patients with and without pruritus, respectively. The percentages indicate the proportions of patients with pruritus among all patients. PBC: primary biliary cholangitis; AIH: autoimmune hepatitis; ALD: alcoholic liver disease; NAFLD: non-alcoholic fatty liver disease.
The mean VAS scores of pruritus during the daytime and at night were 21.78 ± 2.11 and 27.42 ± 2.43, respectively, in all patients with chronic liver diseases who had pruritus. Pruritus was significantly more severe at night than during the day (p < 0.01, Fig. S1a). There were no significant disease-specific differences in VAS in both the daytime and at night (Fig. S2a, b). Notably, VAS score at night was significantly higher in patients with liver cirrhosis than in those without it (Student’s t-test: p < 0.01), although such a significant difference of VAS was not observed in the daytime (Fig. S1b, c). There were no significant differences of VAS between the patients with and without HCC (data not shown). With respect to VRS, 60.7% and 55.1% of patients gave their degree of pruritus as “mild” in the daytime or at night, respectively. There was no significant difference in VRS between the daytime and at night (Fig. S3).
Pruritus has not been sufficiently studied in patients with chronic liver disease. In our study, among 216 patients with chronic liver disease, 41.2% suffered from pruritus. The prevalence of pruritus differed among the different etiologies of chronic liver disease. Its rates were 72.2% in those with PBC, 44.0% in chronic hepatitis C virus infection, 38.5% in ALD, and 24.3% in chronic hepatitis B virus infection, which are similar to the rates in previous reports (1–6). Oeda et al. (6) reported that the prevalence of pruritus in NAFLD was 44.7%, which is higher than our result (14.3%). On the other hand, the prevalence of pruritus in AIH was previously reported to be 24.3%, which is lower than our result (54.5%). We speculate that these differences may have occurred because of the difference in the severity of liver disease of our and their cases. Furthermore, few reports have been published about the frequency of pruritus in chronic liver diseases, except for PBC and chronic HCV infection. Therefore, further examinations of this issue are necessary.
With regard to the degree of pruritus, the mean VAS scores of pruritus were 21.78 in the daytime and 27.42 at night, and 60.7% and 55.1% of patients gave their degree of pruritus as “mild” during the daytime or at night, respectively. In a previous report (6), the mean degree of pruritus with chronic liver diseases when assessed using a numerical rating scale from 0 (no pruritus) to 10 (maximum pruritus) was 4 in the day and 3 at night. These results suggest that the pruritus associated with chronic liver diseases was mild. Although regional differences in the frequencies and types of hepatic diseases are considered to be related to the different findings on the frequency and severity of itching, these studies were conducted in Japan, so global studies are needed to determine whether these findings are valid elsewhere around the world.
In patients with hepatitis C, pruritus was more frequently detected in patients with liver cirrhosis than in those with-out it. Furthermore, the VAS score at night was significantly higher in patients with liver cirrhosis than in those without it. These results are consistent with previous reports (7, 8). Akuta et al. (7) recently reported that having a lower platelet count, which reflected a status of severe fibrosis, was a significant determinant of severe pruritus; moreover, Raszeja-Wyszomirska et al. (8) found that pruritus of cirrhotic patients was more severe than that of non-cirrhotic patients. These findings suggest that liver fibrosis would be closely associated with pruritus. Lysophosphatidic acid (LPA) is an itch mediator induced by autotaxin (ATX) that is found in patients with cholestatic itch (9). ATX was also reported to promote liver fibrosis in a mouse model (10) and was shown to be associated with the severity of liver cirrhosis (11). Therefore, we speculate that the ATX-LPA axis might be one of the most important mediators of itch in patient with liver cirrhosis.


 Click to show fullsize
Click to show fullsize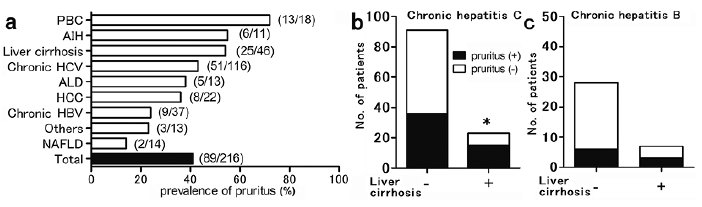 Click to show fullsize
Click to show fullsize