


Department of Dermatology, Bundang CHA Medical Center, CHA University School of Medicine, Seongnam 13496, Korea. E-mail: derma97@gmail.com
Accepted Nov 14, 2018; E-published Nov 14, 2018
Biologics have been increasingly used to treat psoriasis over the past decade (1). Biologics have shown excellent results in the treatment of psoriasis due to their great target specificity (2). Ustekinumab is a fully human monoclonal antibody with high specificity for the interleukin (IL)-12/23 p40 subunit. The safety profile indicates that up to 5 years of ustekinumab treatment is generally favourable and no evidence of cumulative end organ toxicity has been shown (1, 2). To the best of our knowledge, no cases of ustekinumab-associated autoimmune thyroiditis and only one case of interstitial lung disease (ILD) associated with ustekinumab have been reported (3).
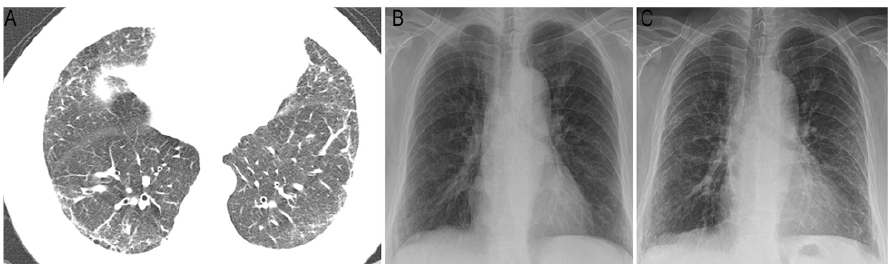
A 68-year-old Korean woman with a 10-year history of plaque psoriasis visited our clinic. Her medical history was significant for osteoarthritis of the knee. Her psoriasis was treated with narrow-band ultraviolet B (NBUVB) for 2 months, oral methotrexate (MTX) 7.5–15 mg weekly for 6 months, and cyclosporine 200 mg daily for 8 months, none of which were effective. Ustekinumab 45 mg was used initially and 4 weeks later, followed by 45 mg every 12 weeks. PASI score reduced dramatically to less than 4 after the third injection. After the fifth injection of ustekinumab, the patient reported dyspnoea and interstitial lung disease (ILD) was diagnosed based on chest computed tomography (CT) (Fig. 1A). Newly developed reticulonodular opacity in both lungs was shown compared with initial chest X-ray (Fig. 1B, C). Diffuse enlargement of the thyroid gland was also found on chest CT. In thyroid function tests, increased T3 level (2.29 ng/ml; normal 0.6–1.81) and decreased thyroid stimulating hormone (TSH) (<0.008 µIU/ml; normal 0.35–5.5) were noted. TSH receptor antibody and anti-thyroid peroxidase (anti-TPO) were all positive and anti-thyroglobulin antibody was equivocal. High uptake of radioactive iodine was also shown. Based on these findings, Graves’ disease was diagnosed and the patient was started on methimazole. After the diagnosis of ILD and Graves’ disease, the use of ustekinumab was discontinued. Respiratory symptoms improved slightly and thyroid hormone levels including autoantibodies were also normalized within 3 months after discontinuation of ustekinumab. Thyroid hormone levels including autoantibodies remain normal even after stopping methimazole.
Fig. 1. (A) Honeycombing and intralobular interstitial thickening on chest computed tomography (B) Initial chest X-ray showed no active disease. (C) Peribronchial and reticulonodular opacity in both lungs was developed after the fifth injection of ustekinumab.
The incidence of ILD associated with biologics is un-known and most cases were due to anti-tumour necrosis factor (TNF)-α agents (4, 5). Many cases of ILD associated with anti-TNF-α agents occurred in patients who were previously prescribed MTX, which has traditionally been associated with the development of drug-induced ILD (5, 6). When TNF-α is suppressed, apoptosis of infiltrating inflammatory cells cannot occur and inflammatory cells persist in the lung, resulting in ILD (6). ILD as an adverse effect of anti-TNF-α agents alone in patients with psoriasis has also been reported in the literature, but it is unclear whether anti-TNF-α agents significantly increase the risk of ILD (7).
There were no reports of ILD and autoimmune thyroiditis in large-population studies evaluating the efficacy and safety profile of ustekinumab in moderate to severe psoriasis (1, 2). Only one case of ILD in a patient with psoriasis treated with ustekinumab has been reported. A 60-year-old man who had a history of taking cyclosporine and infliximab for psoriasis was diagnosed with ILD after 2 years of ustekinumab treatment (3).
IL-12, a target cytokine of ustekinumab, has shown anti-fibrotic activity by increasing interferon (IFN)-γ production in vivo in mice (8). Other in vivo studies showed that overproduction of IL-12p40 contributed to the extension of pulmonary fibrosis through pulmonary macrophage accumulation (9). It is unclear how IL-12 affects lung inflammation and fibrotic changes based on these conflicting results.
As our patient had been prescribed MTX previously, a possible role of MTX on the development of ILD could not be ruled out. Some authors suggested that MTX could be associated with pulmonary toxicities in patients with psoriasis (10). These side-effects have been reported after 16 months to 18 years following MTX initiation. How-ever, the duration of MTX use in our patient was only 6 months (total cumulative dose 300 mg) and ustekinumab was started one year after discontinuation of MTX. Moreover, initial chest X-ray before ustekinumab injection showed no abnormal findings. These findings support the possible role of ustekinumab on the development of ILD.
As the patient had knee joint pain and rheumatoid arthritis could be associated with ILD, further tests were performed to rule out underlying rheumatoid arthritis (RA). Rheumatoid factor (RF) anti-citrullinated protein antibody (ACPA) were all negative and C-reactive protein and erythrocyte sedimentation rate were within normal ranges. The patient did not meet the diagnostic criteria for RA based on 2010 American College of Rheumatology/European League Against Rheumatism (ACR/EULAR) classification criteria for RA. Therefore, we were able to rule out RA-associated ILD.
Several case reports suggested that anti-TNF-α agents could be risk factors for autoimmune thyroid diseases, especially Graves’ disease (11, 12). Ustekinumab-associated autoimmune thyroiditis has not yet been reported. Th2-mediated pathway is thought to be mainly involved in the pathogenesis of Graves’ disease and increased Th2 activity could lead to increased production of autoantibodies directed against TSH receptors (13). They stimulate the function of thyroid follicular cells, leading to hyperthyroidism. As ustekinumab inhibits Th1/Th17-mediated pathway, we hypothesized that IL-12/23 defects may skew the Th1/Th2 balance. However, conflicting data have been reported on Th1/Th2 balance in Graves’ disease, further studies will be needed to determine the exact pathogenesis (13–15). Graves’ disease may have occurred independently regardless of ustekinumab, but the diagnosis was made after ustekinumab treatment and thyroid hormone levels including autoantibodies were normalized within 3 months after discontinuation of ustekinumab. These findings suggest that Graves’ disease in our patient could be related to ustekinumab. According to the World Health Organization Collaborating Centre for International Drug Monitoring, the Uppsala Monitoring Centre (WHO–UMC) algorithm, the causality of these side-effects is probable/likely.
We report here a case of ILD and autoimmune thyroiditis associated with ustekinumab in order to raise the awareness of these complications. The mechanism of ustekinumab-induced ILD and autoimmune thyroiditis is unknown and it is difficult to prove that it is the actual cause of these diseases. However, if patients with psoriasis using biologics are newly diagnosed with these diseases, it should be considered that biologics might be the cause of this condition. Little is known about the mechanism of ustekinumab-associated autoimmune diseases, and further studies will be needed.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize