


1Department of Dermatology, University Hospital of Brest, and 2Laboratory of Neurosciences (EA4685), University of Western Brittany, Brest, France
Primary burning mouth syndrome is a term used for chronic oral mucosal pain with no identifiable organic cause. The aim of the study was to evaluate the usefulness of a psychiatric intervention for treating burning mouth syndrome based on a joint consultation with a psychiatrist and a dermatologist. The study was proposed to all patients who visited this consultation group between 2001 and 2017 for the treatment of primary burning mouth syndrome. The patients answered a questionnaire that was administered via mail. Of the 57 patients diagnosed with primary burning mouth syndrome, 38 were included. Seven patients (18.4%) no longer had pain; 8 (21.1%) estimated that the pain had decreased by greater than 50%; 11 (28.9%) estimated the decrease at between 30 and 50%, and 12 (31.6%) estimated a less than 30% decrease. Only 14 patients (36.8%) remained under treatment with antidepressants, as compared to 63.2% before the psychiatric intervention. This psychiatric intervention could be considered a valuable tool in the global burning mouth syndrome treatment strategy.
Key words: burning mouth syndrome; anxiety; depression; antidepressant; psychiatric intervention.
Accepted Nov 20, 2018; E-published Nov 21, 2018
Acta Derm Venereol 2019; 99:
Corr: Laurent Misery, Department of Dermatology, University Hospital, FR-29609 Brest, France. E-mail: laurent.misery@chu-brest.fr
Primary burning mouth syndrome is a term used for chronic oral mucosal pain with no identifiable organic cause. Burning mouth syndrome are frequently associated with psychiatric disorders. We conducted a monocentric study to evaluate the usefulness of a psychiatric intervention in a joint consultation with a psychiatrist and a dermatologist. Most of our patients demonstrated a significant decrease in pain and a small percentage of patients were completely symptom-free after such interventions. The psychiatric intervention seems to be a good and lasting therapeutic option, and should be integrated in the global strategy in burning mouth syndrome treatment.
Primary burning mouth syndrome (BMS) is a term used for a chronic disorder that is defined by the International Headache Society as an “intraoral burning or dysaesthetic sensation recurring daily for more than 2 h per day over more than 3 months, without clinically evident causative lesion” (1). Symptoms include burning pain or discomfort on the tongue, lips, teeth or in the entire oral cavity, occasionally associated with dysgeusia or xerostomia, without any identifiable organic cause. Its prevalence has been estimated at between 0.1 and 3.9% of the general population (2, 3). In a recent study, the incidence of BMS was 11.4 per 100,000 person-years (4). It is most common in perimenopausal or post-menopausal women (4). The pathophysiology is currently misunderstood. BMS has been shown to be associated with a neuropathic component, with underlying damage to the nerves (e.g., small-fiber neuropathies) and/or a psychiatric component, with co-morbidities (anxiety, depression or/and personality disorder) and putative triggering stressful events in the genesis of this disease (5–8). Patient quality of life is impaired (9). There are no treatment guidelines, and multiple pharmacological agents have been trialed, in particular, antidepressants (10, 11). Recently, a Cochrane review of studies of interventions for treating BMS concluded that there was insufficient evidence to support or refute the use of any interventions in managing BMS and encouraged the assessment of the role of neuropathic pain treatments and psychiatric therapies in the treatment of BMS (12).
Since 2001, in our department, we have organized a joint consultation with a psychiatrist (MC) and a dermatologist (LM then MS) (13). In this consultation, many outpatients are found to suffer from BMS. We conducted a self-reported retrospective and uncontrolled study to evaluate the usefulness of psychiatric intervention in this consultation.
The study was proposed to all primary BMS patients who came to the consultation with the dermatologist and psychiatrist between 2001 and 2017 in the Dermatology Department of the University Hospital of Brest, France. The inclusion criteria were BMS assessed by the presence of symptoms of pain in the oral mucosa, with or without subjective oral dryness or loss or alteration of taste sensation, normal oral mucosa and the presence of pain on most days for more than 4 months. Somatic causes, such as diabetes mellitus or vitamin or nutritional deficiency, were excluded based on standard laboratory tests. The following exclusion criteria were applied: patients younger than 18 years old, with a local or regional aetiologic explanation for the pain and systemic disorders or laboratory abnormalities known to be potentially associated with orofacial pain. When patients reported xerostomia, salivary tests and biopsies of salivary glands were performed to exclude Sjögren’s Syndrome. The study was divided into two analyses: the first was based on medical data from the patient’s file, and the second was based on a questionnaire created for the study and sent to the patients. In 2017, all patients were sent a letter containing information explaining the study and its objectives, as well as the questionnaire and a consent letter to sign. Patients answered the questionnaire by sending back the letter. They were contacted by phone if there was no response after one month. The main author collected all data. The questionnaire investigated the following 7 items:
1. Pain reduction after medical care (complete, > 50%, between 30 and 50% or < 30%);
2. Type of improvement (i.e., less intense, less common, less pervasive, or less stressful) and whether the pain was partially decreased;
3. Whether the patient was still being treated with antidepressants (yes or no);
4 Recurrence of symptoms of BMS (yes or no), and
5. If yes,
a) Whether the patient was consulting with a new specialist (i.e., a dermatologist, psychiatrist or psychologist, otorhinolaryngologist, gastroenterologist, odontologist, or other)
b) Whether the patient was undergoing new antidepressant treatment (yes or no);
6. Importance of help provided by the psychiatric intervention during the consultation (i.e., very effective, helpful or ineffective);
7. Elements that contributed to the clinical improvement after the consultation(s), patients could tick the elements that concerned us on the following list:
- being reassured by the absence of severe illness (cancer, contagious illness…),
- knowing the disease’s name,
- knowing that it is a common disease that is frequently treated in our department,
- understanding the link between pain emergence and difficult or stressful life situations,
- accepting that there are links between the psyche and the body,
- having the opportunity to express one’s feelings,
- having the opportunity to talk about oneself and be heard,
- the antidepressant treatment, and
-other;
- In addition, there was a free comment section.
The primary outcome was the pain decrease experienced after the consultations, complete or partial (> 50%, 30–50%, < 30%). According to the French Society of the Study and Treatment of Pain (Société Française d’Etude et de Traitement de la Douleur - SFETD), medical care or treatment was considered effective when chronic pain was decreased by more than 30% of the initial pain level (14). Secondary outcomes included the persistence of antidepressant treatments, medical wandering, and psychotherapeutic elements that contributed to the clinical improvement.
All data were analyzed using Microsoft Office Excel and are presented in a descriptive way.
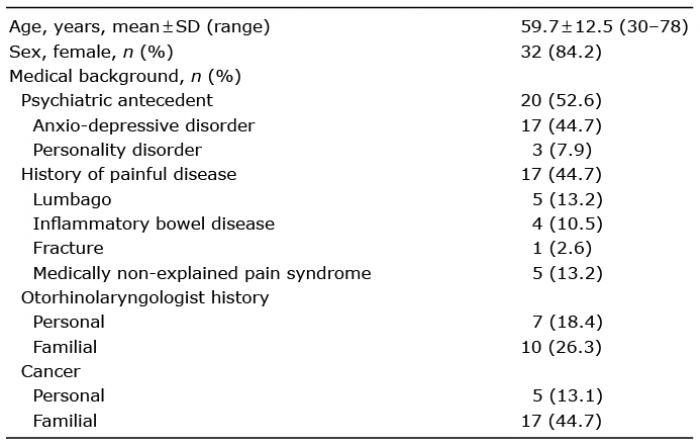
Fifty-seven patients with a diagnosis of primary BMS were seen in the joint consultation between 2001 and 2017. Among these patients, 13 could not be contacted, 4 refused to participate (one refused to sign the consent, 2 had a severe personality disorder, and 1 had already participated in a study of BMS), 1 was disabled (and could not complete the questionnaire), and 1 was deceased. In total, 38 patients were included and completed the questionnaire. Demographic data and medical backgrounds are presented in Table I.
Table I. Demographic data and medical background (n = 38)
All patients had previously consulted with a specialist (Fig. 1). Twenty patients (52.6%) met with a dermatologist and an odontologist associated with another joint consultation. Seven patients (18.4%) resorted to other methods: hypnosis (3 patients), relaxation therapy (2 patients), acupuncture (2 patients) and/or magnetizer (2 patients). Twenty-six patients (68.4%) underwent psychotropic treatment: an antidepressant in 24 cases (11 selective serotonin reuptake inhibitor, 5 serotonin and norepinephrine reuptake inhibitors, 4 tricyclics and 4 of other drug classes) and an anxiolytic (benzodiazepines) in 14 cases (in association with antidepressants for 12 patients).
Fig. 1. Previous doctors consulted. *neurologist, rehabilitation doctor, psychiatrist, chronic pain specialist.
In mean, the patients suffered from mouth pain for 3.7 years (range 0.3–28 years). Twenty-six patients (68.4%) described a stressful life event as a triggering factor. The pain was primarily focused on the tongue (47%) and to a lesser extent, in other mucosal regions (Fig. 2). Ten patients (26.3%) reported somatic symptoms: xerostomia (8 patients), ageusia (2 patients), and/or dysgeusia (3 patients).
Fig. 2. Symptom locations.
Nineteen patients (50%) presented with depressive symptoms. Twenty-five (65.8%) had a psychiatric diagnosis in association with BMS, which was diagnosed by the psychiatric partner of the joint consultation: thymic disorders (36.8%), eating disorders (5.3%), personality disorders (26.3%), others (phobic disorders, obsessive-compulsive disorder, and anxiety: 10.5%). Nosophobia was reported by 36.8% of patients, primarily concerning cancer (64.3%). Ten patients (26.3%) declared that their symptoms were related to a dental intervention, although it was not confirmed in the other joint consultation by the dermatologist and the odontologist. Alexithymia was noted in 14 patients (36.8%) who had difficulties verbalizing their affects.
Twenty-four patients (63.2%) were treated with antidepressants before coming to the psychodermatological consultation (see details in the care path section). This treatment was prescribed in 3 patients (7.9%) after the first consultation. Eleven patients (28.9%) did not receive any psychotropic treatment. A psychological or psychiatric follow-up was proposed for 30 patients (78.9%): 20 patients were followed-up in the dedicated consultation, 4 patients benefited from external monitoring, and 6 patients stopped the follow-up.
The patients benefited from in mean 3 consultations (range 1–14) with the dermatologist and psychiatrist. Nine patients (23.7%) continued to consult with different specialists, including an otorhinolaryngologist (4 patients), odontologist (2 patients), neurologist (2 patients), chronic pain specialist (1 patient), or another dermatologist in joint consultation with an odontologist (2 patients). Eleven patients (28.9%) noticed improvements in affect verbalization. The medical monitoring lasted for in mean 16 months (min 2 months, max 60 months). The answers to the various items are presented in Table II.
Table II. Responses to the questionnaire (n = 38)
Our study is the first to evaluate the usefulness of a psychiatric intervention in the specific context of a joint consultation with a psychiatrist and a dermatologist in patients suffering from BMS. Many of the patients in our study presented with an associated identified psychiatric diagnosis (65.6%), primarily anxio-depressive disorder (36.8%). The presence of a psychiatrist helped to provide the associated diagnosis of depressive disorders. Rojo et al. (15) reported that 51% of patients with BMS had a psychiatric illness diagnosed in association with BMS. In other studies, Sevrain et al. (5) showed that 25.7% of patients experienced depressive disorders, and Schiavone et al. (16) suggested that BMS patients have statistically significant higher scores of depression. In addition, De Souza et al. (17) found a higher frequency of current major depressive disorder in BMS patients (46.7%) and suggested screening for psychiatric disorders to treat patients appropriately.
Considering the primary outcome: most of our patients demonstrated a significant decrease in pain, and a small percentage of patients were completely symptom-free. These results are similar to studies about other psychiatric interventions, such as cognitive behavioural therapies or group psychotherapies (18–20), and regarding local or systemic treatments, the results are more encouraging than some of those reported in the literature (10, 21).
Psychiatric interventions are interesting because chronic conditions, such as primary BMS, are frequently associated with psychiatric disorders. A recent literature review of the therapeutic options for idiopathic BMS reported that cognitive therapy is a good and lasting therapeutic option, with the advantage of having no side effects, and can be combined with pharmacologic therapy (18, 22). Furthermore, a Cochrane review of the treatments for primary BMS has found that cognitive-behavioral therapy was one of only 3 interventions that reduced BMS symptoms (12). Arpone et al. (23) also suggested taking a biopsychosocial approach in a joint medical-psychiatric consultation model, with a different specialist (an odontologist rather than a dermatologist). This binomial approach has the advantage of considering the multiple factors involved in BMS onset and persistence. A recent study has concluded that information and reassurance can result in a positive shift of pain perception in patients with primary BMS. The reduction of symptoms, along with a better quality of life, was comparable to that provided by the pharmacological treatment (24). To evaluate the psychiatric intervention, we used another procedure. We studied pain evolution, medical wandering, use of antidepressants, and patient satisfaction. In that manner, a recent study has highlighted that a combination of antidepressants and cognitive behaviour therapy is more effective (25).
In this study, 74% of the patients were satisfied with the psychiatric intervention: 58% of the patients thought that it was helpful, and 16% thought that it was very effective. In our joint consultation, the psychiatric approach focused on listening to the patient, which could allow the patients to understand their symptoms. We searched for the psychological elements that were helpful for symptom improvement. It seems to be important to reassure the patients about the absence of severe illness and to propose psychiatric management through a dedicated consultation to help them make a putative link between pain emergence and stressful life events, to allow them to express their feelings, talk about themselves and be heard. Arpone et al. (23) have suggested listening to, and expanding a patient’s complaints to approach their suffering and provide global medical care. Brailo et al. (24) have suggested reassuring patients with concerns about the etiology (malignant, infectious or allergic in nature) of their disease.
In our study, all patients had already consulted with a specialist and continued to consult with them for the same symptoms. This point shows the refractory nature of primary BMS and suggests that the presence of psychiatric symptoms might significantly interfere in its treatment (17, 26, 27). However, another study reported that only 11% of patients with chronic orofacial pain were referred to psychiatric care or psychotherapy (28). Furthermore, it is easier for patients to obtain psychiatric advice in a joint consultation. The interdisciplinary character of the consultation offers a progressive transition from the soma to the psyche. In a direct consultation with a psychiatrist, the patient might think that their somatic complaint has not been heard.
Interestingly, symptom recurrence was reported by 55.3% of patients, and most did not consult a new specialist. This point shows that they learned to recognize and understand their symptoms. However, 9 patients needed new advice and a new antidepressant treatment. This might reflect the chronic aspect of BMS and the fact that the physiopathology may be partially understood.
An increasing number of BMS studies have suggested the existence of neuropathic components in pain genesis (5–7, 29). Sevrain et al. (5) reported that 31% of patients had an abbreviated Douleur Neuropathique 4 questionnaire score in favour of neuropathic pain. Moreover, Jääskeläinen (7) highlighted 3 distinct subclasses of neurophysiologically characterized BMS: peripheral small fibre neuropathy, subclinical major trigeminal neuropathy, and central pain that might be related to deficient dopaminergic top-down inhibition. The efficacy of topical neuropathic pain treatment (clonazepam and capsaicin) (30) in certain forms of the disease provides evidence for neuropathic involvement. In addition, Zakrzewska (31) raised the neuropathic role in BMS physiopathology. This author also underlined the importance of the multi-dimensional character of this chronic pain. Hence, the association between BMS and psychological and psychiatric components, even if they are not the cause of trouble, must be considered by the clinician.
Our study has some limitations. First, this was a monocentric study. As an uncontrolled self-reported retrospective study, recall bias may exist. The questionnaire is not a validated tool and was sent only once (no comparative data are available for before and after the intervention) on the same date. Consequently, the time course differed from patient to patient. Another limitation is that some of the patients underwent previous psychiatric treatment, which is the referent treatment in BMS. Although no patient reported an increase in symptoms during treatment, it should be emphasized that anticholinergic molecules might increase xerostomia symptoms. Moreover, the evaluation of pain decrease is subjective; however, primary BMS patients describe discomfort more than real pain. In hindsight, performing a new, prospective study would provide better statistical power. To support these findings, it would be interesting to perform a study with a control group to compare pain evolution with and without psychiatric intervention.
In concluson, primary BMS deserves multidisciplinary management. A psychiatric component frequently occurs in patients with primary BMS. Psychiatric management should be part of medical care in primary BMS, particularly because no efficient pharmacological treatment is available. In addition, the problem has serious repercussions on quality of life, due to the chronic pain. A dedicated psychiatric intervention should be considered as an additional tool in the global strategy for BMS treatment. A multidisciplinary approach appears to be a valuable tool for such an intervention, in particular, that with a dermatologist and a psychiatrist; however, other disciplines may also be involved.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize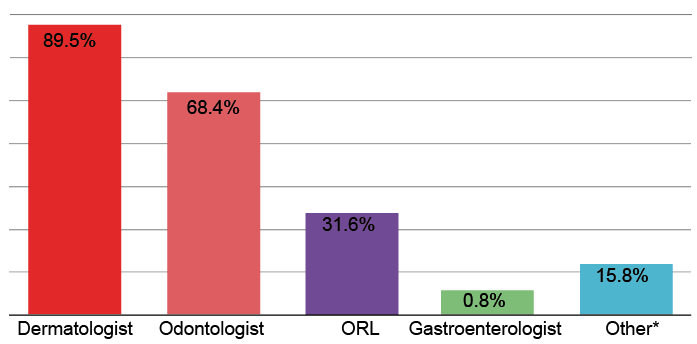 Click to show fullsize
Click to show fullsize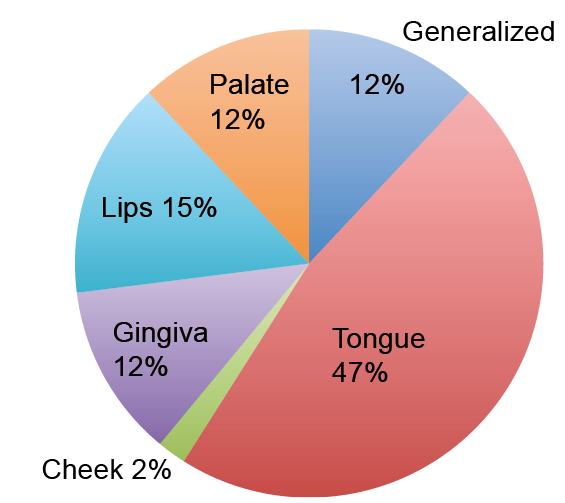 Click to show fullsize
Click to show fullsize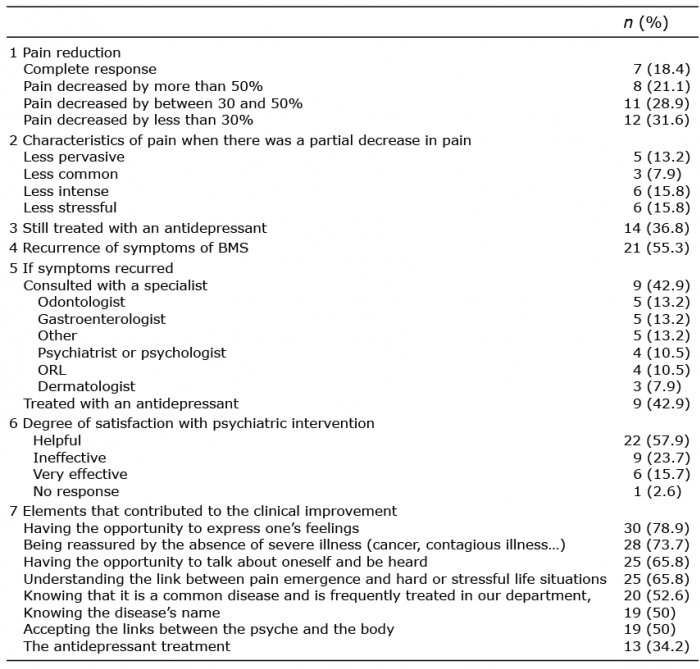 Click to show fullsize
Click to show fullsize