


1Department of Dermatology, Henri Mondor Hospital, Assistance Publique Hôpitaux de Paris, 51 avenue du Maréchal de Lattre de Tassigny, FR-94000 Créteil, 2EA EpiDermE 7379, Paris Est University, Créteil, and 3Jérôme Lejeune Institut, Paris, France. E-mail: florence.poizeau@wanadoo.fr
#These authors contributed equally to this work.
Accepted Nov 20, 2018; E-published Nov 21, 2018
Hidradenitis suppurativa (HS) is a chronic inflammatory skin disease characterized by recurrent painful deep nodules and abscesses of the axillary, breast, groin and anogenital regions (1). The estimated prevalence of HS in the European general population is 0.1–4.1% (2, 3). HS is thought to be more frequent in patients with Down syndrome (DS) (4, 5). However, the prevalence of HS in patients with DS has not been estimated in the clinical setting.
The following hypothesis of a genetic link with DS could explain the suggested increased risk of HS in this population. Gamma-secretase, a transmembrane protease, plays a key role in HS (6). Gamma-secretase cleaves the Notch receptor and amyloid precursor protein (APP). Accumulation of APP in DS may occur due to trisomy of chromosome 21 in DS, since the gene encoding APP is located on this chromosome. APP and Notch receptor are competitive substrates for γ-secretase; therefore it is possible that processing of the large amount of APP might occur at the expense of Notch signalling (5). Moreover, because another APP cleavage product stimulates keratinocyte proliferation, patients with DS might be susceptible to follicular plugging, which characterizes HS.
The aims of this study were to describe HS and to assess the prevalence of the condition in a French population with DS.
This cross-sectional study of prevalence of HS was performed in a French centre for DS. Physicians were trained in the identification of HS and, for every new DS patient aged 8 years and over, they completed a questionnaire based on the definition of HS. Participants were asked, “Have you ever had large, painful, deep-seated nodules or boils?” If the answer was “yes”, and if the lesions were recurrent and located on compatible areas (groin, armpits, genitalia, under the breasts, buttocks), the participant was considered to have HS. Epidemiological data were collected and all patients with a diagnosis of HS were referred to the department of dermatology.
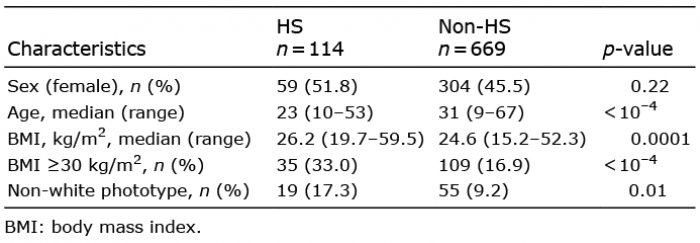
Among the 783 participants with DS included in the study from December 2015 to March 2017, 114 had HS. The estimated prevalence of HS was 14.6% (95% confidence interval 12.3–17.2%). The median age of the DS population was 29 years (range 9–67 years). The sex ratio of HS and non-HS participants was similar (Table I). Obesity (body mass index (BMI) ≥30 kg/m2) and a non-white phototype were more frequent in subjects with HS than in those without HS (Table I). Only 6/783 participants smoked.
In total, 17 patients were examined by a dermatologist, and a diagnosis of HS was confirmed in all cases. Eleven of the 17 patients were female, median age was 22 years, and median BMI 26.6 kg/m2. None of the 17 patients smoked. None had a family history of HS or an association with an inflammatory disease. The disease was mild in these patients: 9 patients had Hurley stage I disease, 7 had stage II disease, and 1 had stage III disease. The classical axillary-mammary phenotype was predominant (10 vs. 5 patients with a follicular phenotype, and 2 with a gluteal phenotype) (7).
Table I. Characteristics of patients with Down syndrome with and without hidradenitis suppurativa (HS)
The estimated prevalence of HS in the study population of 783 participants with DS was 15%. However, misclassification bias may have occurred, as not all of the patients were checked by a dermatologist. To minimize bias, the physicians in the centre underwent training in the clinical signs of HS before and during the study period. Data on any symptoms found were collected.
In addition, age may be a confounding factor, since individuals with DS are younger than the general population. The age distribution in our centre was representative of the general populations of individuals with DS. In order to make a more reliable comparison among studies and to increase the generalizability of our results, the crude prevalence was age-adjusted using the US DS population as a standard (n = 78,842 DS individuals) (8). The age-standardized prevalence of HS was 13.0% (95% CI 10.9–15.1%).
The increased prevalence of HS in DS found here is consistent with the results of previous studies (4, 9). In a retrospective study of 667 patients with HS (4), the prevalence of DS was found to be 29 times higher than in the general population. However, the number of patients with HS and DS reported in these studies was low (16 or fewer), and the prevalence of HS was not estimated (4, 9). A cross-sectional study based on a US institutional database estimated the prevalence of HS as 2.1% for DS individuals (5). However, identified cases were restricted to individuals with physician-diagnosed HS (International Classification of Diseases, 9th revision; code 705.83), which leads mainly to the identification of patients with HS requiring medical follow-up (severe HS), and could explain an underestimation of the prevalence.
The current study found an association of HS with obesity and non-white phototype in subjects with DS. This association has been described previously in patients without DS (3). In contrast, the lack of female predominance does not indicate an endocrine cause of HS in DS. This observation is in contrast to a study of cases of HS caused by mutations in γ-secretase (7).
HS is frequent in DS; an estimated prevalence of 15% was determined in this study of 783 participants with DS. Further research is needed in order to confirm the phenotype and severity of HS in DS.


 Click to show fullsize
Click to show fullsize