


Dermatology and Venereology Department, Geneva University Hospitals, Rue Gabrielle-Perret-Gentil 4, CH-1205 Genève, Switzerland. E-mail: Caroline.deLorenzi@hcuge.ch
A 65-year-old Egyptian man presented to our clinic with a 4-year history of increasing, multiple, painless 1-mm keratotic spiny lesions on his palms (Fig. 1a and b) and fingers (Fig. 1c) exclusively. On examination no other areas of skin involvement were noted. His medical history included diabetes mellitus type 2 controlled with metformin, dyslipidaemia treated with rosuvastatin, and benign prostatic hyperplasia treated with a plant-based preparation. His family history was negative for similar lesions or dermatological disease. A colonoscopy and fibroscan performed in 2015 showed normal results. The patient currently smokes a pipe every 2 days and works as an engineer.
A skin biopsy showed an acanthotic epidermis with elongated rete ridges and thinned granular layer, and a hyperkeratotic column with focal parakeratosis. A perivascular, mainly lymphocytic, inflammatory infiltrate was present in the dermis (Fig 2).
Multiple tests were performed to rule out a systemic cause and paraneoplastic origin for these acquired lesions. These included complete blood count, as well as hepatic tests, renal function, thyroid-stimulating hormone (TSH), glucose, prostate-specific antigen (PSA) and immunofixation, which were all within normal limits. Chest X-ray and an otolaryngology evaluation were negative for malignancy.
Complete resolution was achieved a few weeks after application of a cream containing urea (120 mg/g), tretinoin (0.3 mg/g) and dexpanthenol (10 mg/g).
What is your diagnosis? See next page for answer.
Fig. 1. (a) Multiple brownish-yellowish filiform keratotic papules on the left palm. (b) Close-up on the filiform keratotic lesions on the palm. (c) Filiform keratotic papules on the fingers.
Fig. 2. (a) Haematoxylin and eosin (H&E) original magnification ×5. Acanthotic epidermis with elongated rete ridges and a hyperkeratotic column. Dermis shows a perivascular, mainly lymphocytic, inflammatory, infiltrate. (b) H&E, original magnification ×20. Epidermis with thinned granular layer and hyperkeratotic column with focal parakeratosis.
Acta Derm Venereol 2019; 99: XX–XX.
Diagnosis: Porokeratosis punctata
Clinicopathological correlation was consistent with a diagnosis of porokeratosis punctata. Porokeratosis punctata palmaris et plantaris (PK) is a subtype of punctuate keratoderma, a subgroup of palmoplantar keratodermas, which consist in abnormal keratinization on the palms and soles (1, 2). It is characterized by multiple small horny keratotic spines a few mm in size, arising on palms, soles or both, and flexor aspects of the digits (1–3).
It was first described by Brown in 1971 (3) and numerous names can be used to describe this disease. Those include: punctuate porokeratosis, punctuate porokeratotic keratoderma, spiny keratoderma on the palms and soles, spiny keratoderma, palmoplantar filiform hyperkeratosis, filiform hyperkeratosis, music box dermatitis and minute digitate hyperkeratosis (2, 4–8).
PK has been described in association with malignant neo-plasms (bronchial, renal, rectal, breast cancer, melanoma), chronic renal failure, polycystic kidney disease, hyperlipidaemia, diabetes mellitus and Darier’s disease (5, 8). A few familial cases have also been described (7).
As PK can precede malignancy by many years, regular follow-up should be scheduled according to age and personal risk factors (5, 6).
Treatment can be challenging, as the disease may resurge if discontinued (6). Topical treatment with urea, salicylic acid, vitamin A or 5-?uorouracil cream or physical treatment, such as shaving or carbon dioxide laser vaporization, can be effective (5, 6).
In conclusion, PK consists of spiny keratotic skin lesion on the palms and soles that warrants further work-up to rule out malignancy.


 Click to show fullsize
Click to show fullsize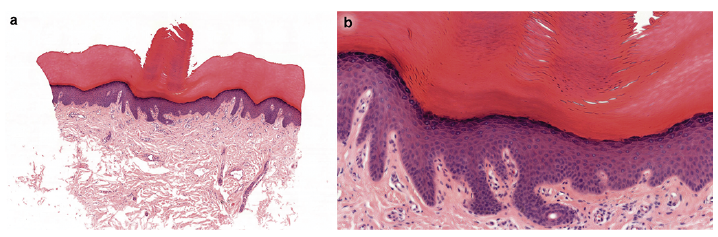 Click to show fullsize
Click to show fullsize