


1Dermatology Department, and 2Pathology Department, Pontevedra University Hospital, EOXI Pontevedra-Salnés, Centro de Especialidades Mollavao, c/ Simón Bolívar s/n., ES-36001 Pontevedra, Spain. E-mail: alvaroigpu@gmail.com
Accepted Dec 6, 2018; E-published Dec 6, 2018
Anetoderma is a rare skin condition marked by circum-scribed areas of slack skin due to the loss of dermal elastic fibres. Based on aetiology, anetoderma can be classified into 2 forms. Primary anetoderma (PA) develops in clinically normal skin (Schweninger-Buzzi type) or after a non-specific inflammatory process (Jadassohn-Pellizzari type), whereas secondary anetoderma arises from an abnormal reparative mechanism of well-defined preceding skin diseases (1, 2).
Anetoderma has been related to different immunological diseases, ranging from simple serological findings to well-defined pathologies (2). Although the connection may not be so much with systemic lupus erythematosus (SLE) as with the presence of antiphospholipid antibodies (APA) (3), patients with both conditions (anetoderma and SLE) in the absence of APA have been described (4, 5). Moreover, the pathophysiology, as well as a temporary relationship between APA, SLE development and onset of anetoderma, have not been well established.
A 43-year-old man presented with a 1-year history of gradually spreading, non-itching skin lesions that had appeared on his trunk and left arm. Regarding his previous medical history, he had been diagnosed with SLE 8 years previously due to the presence of erythema after sun exposure, discoid facial lesions, oral ulcers and consistent positive serology (antinuclear antibodies (ANA) >1/640 speckled pattern and anti-double-stranded antibodies (dsDNA) > 1/10). There was no history of vascular thrombosis, neurological disorders or heart valve defects. His condition had been treated with hydroxychloroquine for 3 years. Since he became asymptomatic, he had decided to drop out of the treatment and was lost to follow-up.
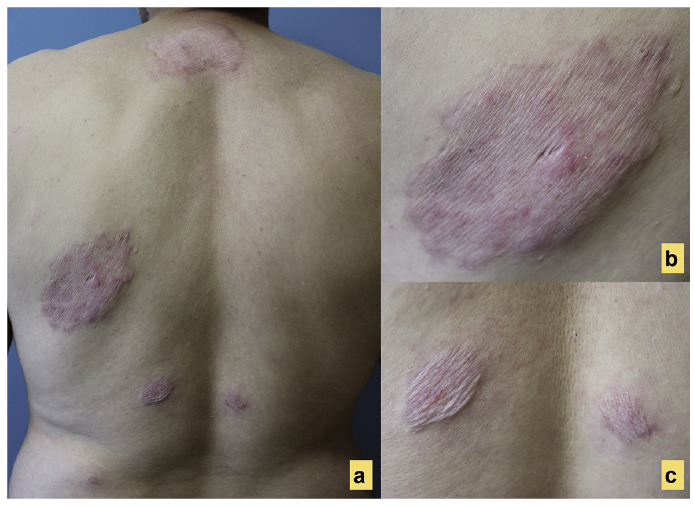
Physical examination showed well-circumscribed, erythematous round plaques with overlying wrinkled skin and herniation phenomenon on his left arm and upper and lower back. These lesions had developed on previously healthy skin according to the patient’ medical records (Fig. 1).
Fig. 1. Well-circumscribed, erythematous, round plaques with overlying wrinkled skin and herniation phenomenon on the upper and lower back.
Laboratory studies demonstrated no abnormalities except persistent lymphopaenia (lymphocytes <1,200/mm3). Immunological studies revealed a negative extractable nuclear antigen (ENA) panel, low serum levels of C3 (80 mg/dl, normal range 88–201 mg/dl) and negative APA. Serological tests, including for HIV, syphilis and Borrelia, were also negative.
A skin biopsy from a lesion on his back showed superficial and deep perivascular lymphocytic infiltrate with no thrombi detected in dermal blood vessels. Verhoeff-van Gieson staining evidenced depletion and fragmentation of elastic fibres, which was more evident in the upper dermis (Fig. 2). Direct immunofluorescence (DIF) study detected granular IgG (+++), IgM (++) and C3 (+++) deposits in the basement membrane and blood vessels of involved skin. These findings confirmed the diagnosis of anetoderma in a patient with SLE.
Based on the association of anetoderma with APA, the patient was tested for APA with a 6-month periodicity. One year later, positive results for lupus anticoagulant test (dilute Russell viper venom time (DRVVT) ratio >1.2) and beta-2-glycoprotein 1 antibodies (IgG > 46.7 IU, positive > 20 IU) were found. Regarding the absence of criteria for antiphospholipid syndrome, the patient was advised not to smoke or gain weight, and hydroxychloroquine was prescribed again.
Fig. 2. (a) Superficial and deep perivascular lymphocytic infiltrate with no thrombi in dermal blood vessels (haematoxylin and eosin ×40). (b) Verhoeff-van Gieson staining depletion and fragmentation of the elastic fibres, which was more evident in the upper dermis (Verhoeff-van Gieson staining ×40).
Anetoderma is an elastolytic disorder characterized by localized areas of wrinkled or flaccid skin due to a decrease in the amount of normal elastic tissue (5, 6). This condition has classically been connected with autoimmune diseases, such as SLE or lupus-like syndromes (2, 3). However, the most consistent reported association of anetoderma within the spectrum of autoimmune features is the presence of APA, prevalence of which in SLE is greatly increased (3, 4, 7). Anetoderma could be consequently considered as a skin manifestation of antiphospholipid syndrome (8), even though not all patients with this association will develop prothrombotic abnormalities (9, 10).
A PubMed search, of the English-language medical literature, using the keywords “systemic lupus erythematous” and “anetoderma” yielded 16 reports comprising 22 patients presenting both entities (Table SI) (1–16). Considering all those reported cases showing positive APA (19/23 cases), only 6 patients fulfilled the criteria of antiphospholipid syndrome.
Regarding the relationship between anetoderma and APA, it has been described that these antibodies may cause dermal microthromboses, which could lead to focal ischaemia and subsequent destruction of elastic tissue (9). Since microthromboses were found in only 6 out of 23 biopsy specimens, they may not necessarily cause anetoderma. However, at least 7 reported cases were found with more than 4 years of ongoing lesions. Thus, it is impossible to know whether microthromboses actually occurred, or if this finding was not seen due to the time lapse between the onset of the lesions and the biopsy (10).
Some authors believe that elastic fibres may be the target of antibodies against shared epitopes between phospholipids (probably beta-2-glycoprotein 1) and elastin (5).
On the other hand, the indispensable presence of APA for development of anetoderma could be called into question, as 4 patients presented with SLE-A and were tested negative for APA. Interestingly, one of these patients demonstrated immune deposits in the involved skin, supporting the role of additional immunological mechanisms in some cases.
The relatively few DIF studies of anetoderma lesions in patients with SLE performed to date have shown positive results in 85% cases, of which positive lupus band test was the most common finding. In 1990, Bergman et al. (17) described 9 patients with positive linear or granular immunoreactants along the dermoepidermal junction on PA-affected skin. Although none of the patients in this group fulfilled the minimum number of SLE criteria, they concluded that some patients with PA had DIF findings indistinguishable from those of SLE, which may also reinforce the hypothesis of a primary immunological event.
The temporal relationship between anetoderma, SLE and APA has not been well established. It is noteworthy that 2 patients with SLE who developed anetoderma were later found to have positive APA, which may question their causal effect on the onset of anetoderma. Since at least 7 patients with SLE-A were simultaneously diagnosed as positive for APA, the concurrence of these entities may not be coincidental. Moreover, with time, SLE has become evident in some patients with PA who previously did not fulfil the criteria for this diagnosis (7, 13).
In conclusion, this rare elastolytic disorder may be part of a wide spectrum of autoimmune disorders, the elastic fibres being one of the potential target tissues. In diagnosing patients who present with anetoderma and negative APA there is doubt about a definitive cause and effect relationship between these entities, and therefore a systemic search for autoimmune disorders and long-term follow-up should be performed in all cases.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize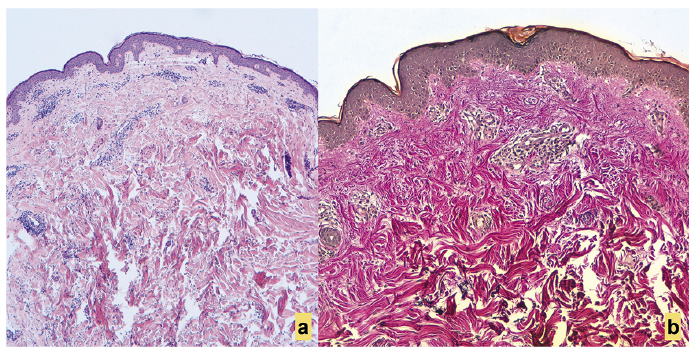 Click to show fullsize
Click to show fullsize