


Departments of 1Dermatology, 3Obstetrics and Gynaecology and 4Pathology, Turku University Hospital and University of Turku, PO Box 52, FIN-20521 Turku, and 2Auria Biobank, University of Turku and Turku University Hospital, Turku, Finland. E-mail: niina.hieta@utu.fi
Accepted Dec 6, 2018; E-published Dec 6, 2018
Lichen sclerosus (LS) is a chronic inflammatory skin disease presenting mainly on the anogenital area. The prevalence of LS has been estimated as 1:300 to 1:900, and even higher in elderly women (1, 2). The life-time risk of female patients with LS developing vulvar squamous cell carcinoma (SCC) is 4–5% (1).
Vulvar melanoma is rare, with an incidence of 0.10–0.13 per 100,000 individuals, presenting typically in post-menopausal women (3, 4). In Finland, the incidence of vulvar melanoma between years 2010 and 2014 was 0.08–0.12 per 100,000 individuals (The Finnish Cancer Registry: data upon request), which is in line with other vulvar melanoma incidence studies. Reports on vulvar melanoma among patients with LS are few. So far, 4 cases have been described among adult patients and 6 cases in prepubertal girls (3, 5, 6). The aim of this study was to clarify the possible connection between LS and vulvar melanoma.
A data search identifying female patients with reported SNOMED Clinical Terms for LS (M58240) and vulvar melanoma (M87203) between 1 January 2000 and 1 September 2013 was conducted in Auria Biobank, Turku University Hospital (TYKS). Clinical histories were obtained from medical records. Population-based data for comparison regarding the incidence of vulvar melanoma were retrieved from the Finnish Cancer Registry. The study was approved by Auria Biobank’s Scientific Steering Committee and the Institutional Review Board of Turku University Hospital.
Formalin-fixed, paraffin-embedded specimens of primary vulvar melanomas and reoperations were obtained from Auria Biobank. Haematoxylin-eosin stained slides from the melanoma specimens were examined by a pathologist to confirm or exclude the diagnosis of LS, and to confirm the Clark stage and Breslow’s index (Fig. 1).
Survival time was calculated from date of diagnosis to date of death or 1 September 2013, whichever came first. To calculate the relative risk of vulvar melanoma among patients with LS compared with those without LS, a 2-by-2 contingency table analysis was used. To compare Breslow and Clark staging, Student’s t-test for 2 independent means for Breslow and one-way analysis of variance (ANOVA) for Clark were used. One-way ANOVA was used to compare tumour stage and the Kaplan–Meier estimator to study survival. To compare the 2 survival curves, the log-rank test was used. A p-value lower than 0.05 was considered significant.
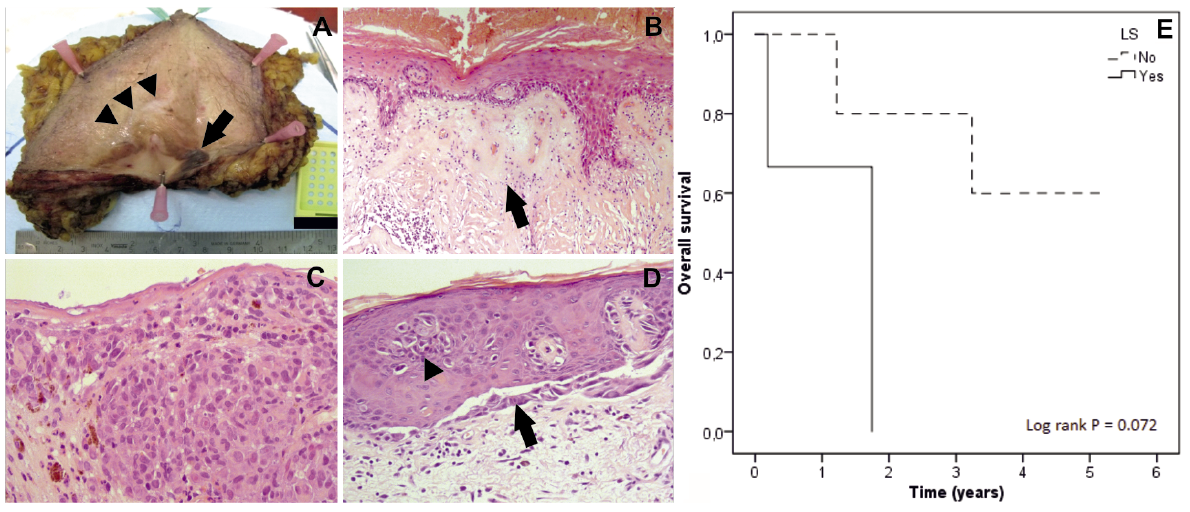
Fig. 1. (A) Vulvectomy specimen with in situ melanoma on the right lower part (arrow). The patient previously operated for an exophytic melanoma had a re-operation of the tumour area. Typical features of lichen sclerosus (LS) are seen, including a porcelain-white area above clitoral hood (arrowheads). (B) Late stage of LS with hyalinization of the dermis and deep inflammatory infiltrates. (C) Histological image of invasive vulvar melanoma with nodular growth. The tumour cells have abundant eosinophilic cytoplasm and marked nuclear atypia with enlarged nucleoli. Mitotic frequency was high and some granular pigment consistent with melanin was seen. (D) In situ melanoma with tumour cells spreading at the dermoepidermal junction (arrow) and in the epidermal layers (arrowhead). (E) Kaplan–Meier survival curves showing survival of vulvar melanoma patients with or without LS.
The data search found 249 patients with vulvar LS, confirmed by biopsy. Among these patients, 3 vulvar melanomas were identified (Table SI). As comparison, 30 cases of SCC were found among patients with LS. Representative macroscopic and histological images of the melanomas are shown in Fig. 1. The patients were not diagnosed with LS until the diagnosis of melanoma was made. Six melanomas were diagnosed among patients who did not have LS among a total population of 250,000 female subjects. The risk of vulvar melanoma among patients with LS was 341 times higher than the risk among women without LS (p < 0.001).
The survival rates of LS patients with vulvar melanoma showed a tendency towards worse survival compared with non-LS patients with vulvar melanoma, although the difference was not statistically significant (p = 0.072) (Fig. 1E). All 3 patients with LS had died within 2 years after diagnosis of melanoma, whereas only 3 out of 6 patients without LS had died of the by the end of the disease follow-up period.
Vulvar melanoma patients with LS had a mean Breslow’s index of 12.8 mm (range 9–19 mm) and median Clark stage IV. Patients without LS had a mean Breslow’s index of 5.6 mm (range 1.2–11 mm) and median Clark stage IV. There was no statistically significant difference between LS or non-LS patients with vulvar melanoma in terms of Breslow’s index (p = 0.71) or Clark stage (p = 0.35). The tumour stage was statistically significantly higher in patients with LS (p = 0.0011).
All non-LS patients, except for one, had ulceration in the tumour. Due to poor prognosis, the lymph node status was not studied in 2 melanoma patients with LS. The size of the tumour was not reported on 2 non-LS patients, and therefore no statistical analysis could be performed.
Among 9 patients with vulvar melanoma, 3 were also diagnosed with LS. The relative risk of vulvar melanoma among patients with LS is 341.
The higher incidence of vulvar SCC among patients with LS has been suggested to relate to the molecularly altered epithelium generated as a result of chronic inflammation with abnormal cytokine and growth-factor production (7). It has been shown that melanocytic naevi on LS lesions differ from ordinary naevi: they contain abundant melanin, diffusely express HMB-45, and have a higher Ki-67 labelling index (6). Little is known about the risk factors and aetiology of melanomas on areas not associated with chronic sun damage. A family history of melanoma is a risk factor for both cutaneous and mucosal melanoma (8). In the current study, there was no previous personal or family history of melanoma in any of the LS or non-LS patients. Mutations in genes regulating cellular proliferation, apoptosis, and survival are differently expressed in vulvovaginal melanomas compared with cutaneous melanomas and other mucosal melanomas (9).
The prognosis of vulval melanoma is worse than that of cutaneous melanoma. The reason for this is not known. In addition, the reason for the even worse outcome of vulvar melanoma among patients with LS is unknown. The patients with LS had a more advanced stage, but there were no statistically significant differences in Breslow or Clark classification or in histological ulceration. However, the prognosis for vulvar SCC is also worse among patients with LS compared with human papilloma virus-positive patients (10).
The presence of LS among patients with SCC is often not recognized (11). In the study with 3 adult patients with vulvar melanomas presenting with LS, LS was present in sites of melanoma-in-situ, but disappeared in sites of invasive melanoma, where dermal hyalinization was replaced by desmoplasia (3). In previous studies on vulvar melanoma this may have led to lack of recognition and, consequently, to under-reporting of LS. Also, in our 3 patients with vulvar melanoma and in the 3 adult patients described in detail previously, melanoma was at least 1.0 mm thick, and LS was present only on some parts of the vulvectomy specimen.
We report here, for the first time, an increased incidence of vulvar melanoma among patients with LS. The increased risk of vulvar malignancies other than SCC should be noted in patients with LS. Further studies are needed to evaluate the role of LS in the pathogenesis of vulvar melanoma.
This work was supported by grants from the Finnish Medical Foundation, and Turku University Hospital (project 13287).


 Click to show fullsize
Click to show fullsize