


1Department of Medicine of Sensory and Motor Organs, Division of Dermatology, Faculty of Medicine, Tottori University, 86 Nishi-Cho, Yonago, Tottori 683-8503, 2Department of Pathology and Oncology, School of Medicine, University of Occupational and Environmental Health, 3Division of Dermatology, Department of Internal Related, Kobe University Graduate School of Medicine, Kobe, and 4Division of Dermatology, National Hospital Organization Hamada Medical Center, Japan. E-mail: higaki.h@med.tottori-u.ac.jp
Accepted Dec 13, 2018; E-published Dec 13, 2018
Multiple clustered dermatofibroma (MCD) is a rare variant of dermatofibroma (1). Clinically, there are multiple nodules grouped or arranged in a linear pattern on a single anatomical site, mainly in the bottom half of the body (1). We present here an unusual case of congenital MCD that developed on the face.
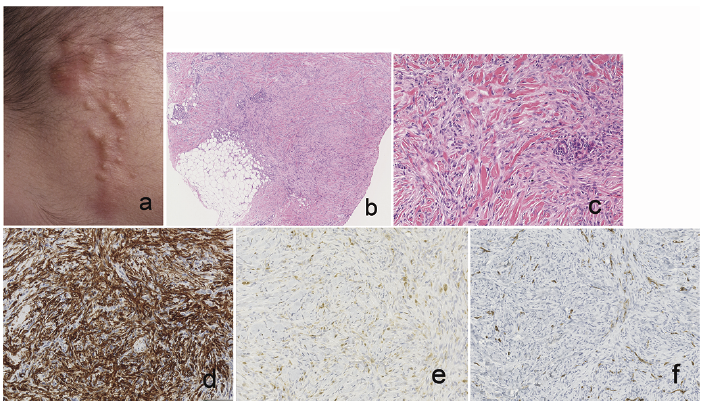
A 13-month-old boy was referred to us for examination of multiple nodules on his right forehead. The lesions were first noticed at birth and had increased during the past several months. On physical examination, firm, pink-tan nodules, ranging in size from 2 to 10 mm were clustered in a linear arrangement (Fig. 1a). Dermoscopy showed a homogenous pigment network (not shown). A biopsy specimen showed a nodular lesion in the reticular dermis and superficial subcutis (Fig. 1b). The tumour consisted of short fascicles of lightly eosinophilic spindle cells intermingled with collagen bundles (Fig. 1c). There was no significant atypia or pleomorphism in the tumour cells. The overlying epidermis showed slight acanthosis with basal hyperpigmentation. Immunohistochemistry studies showed strong positivity for alpha-smooth muscle actin (α-SMA) (Fig. 1d) and moderate positivity for factor XIIIa (Fig. 1e) and D2-40. The tumour cells were negative for CD34 (Fig. 1f), S-100 protein, SOX10, pancytokeratin (AE1/3), ERG, epithelial membrane antigen and factor VIII. Expression of trimethylation of histone H3 lysine 27 was intact. Thus, this case was diagnosed as MCD.
Fig. 1. (a) Clinical appearance of nodules on the forehead. (b) Histopathological feature. The nodular lesion consisted of spindle cells in the reticular dermis and superficial subcutis (haematoxylin and eosin (HE), original magnification ×100). (c) Proliferation of spindle cells with collagen trapping (HE ×200). (d) Immunostaining for alpha-smooth muscle actin (original magnification ×200). (e) Immunostaining for factor XIIIa (×200). (f) Immunostaining for CD34 (×200).
Malignant tumours, including dermatofibrosarcoma protuberans (DFSP), pseudomyogenic haemangioendothelioma and low-grade malignant peripheral nerve sheath tumour, had to be ruled out in the differential diagnosis of this case. DFSP is commonly composed of CD34-positive and factor XIIIa-negative spindle cells arranged in a storiform pattern. D2-40 is negative in most cases of DFSP. Pseudomyogenic haemangioendothelioma and low-grade malignant peripheral nerve sheath tumour may occur as multiple nodules composed of spindle cells. Immunohistochemistry and cell morphology are helpful to rule out these 2 diseases. Other diagnoses considered were fibroblastic connective tissue naevus, infantile myofibromatosis, dermatomyofibroma, and plaque-like myofibroblastic tumour. Fibroblastic connective tissue naevus is a rare benign lesion of fibroblastic/myofibroblastic lineage that has been recognized recently (2, 3). Typically, CD34-positive spindle cells proliferate in the reticular dermis and superficial subcutis with epidermal papillomatosis. Adipose tissue is frequently seen in the reticular dermis. Infantile myofibromatosis and dermatomyofibroma show characteristic histopathological patterns. Most cases of infantile myofibromatosis show a nodular proliferation of plump spindle cells with pale eosinophilic cytoplasm arranged in short fascicles or whorls. Hemangiopericytoma-like components are also seen in the central part of the nodule. Dermatomyofibroma consists of fascicles of fibroblastic spindled cells arranged parallel to the overlying epidermis. Plaque-like myofibroblastic tumour was first described in 2007 (4). The tumour presents as firm nodules or plaques arising mainly on the lower back of infants and children, and the tumour shares many histopathological features with dermatofibroma. A plaque-like myofibroblastic tumour characteristically shows strong positivity for α-SMA. However, dermatofibroma sometimes expresses α-SMA. Thus, α-SMA expression is not helpful for differential diagnosis between these 2 entities. It has been suggested that MCD and plaque-like myofibroblastic tumour belong to a part of the same disease spectrum (5).
The current case showed many small nodules on the right forehead. The term “multiple clustered” may be more appropriate than “plaque-like” to describe this clinical feature. Although most cases of MCD have a benign course, a rapid growth phase is seen in some cases. During the rapid growth phase, the lesions expand progressively over a period of a few months. Long-term follow-up is necessary to exclude other diseases, including malignancies. It is important for clinicians to take MCD into account in the differential diagnosis of infantile multiple nodules.


 Click to show fullsize
Click to show fullsize