


1Department of Medicine of Sensory and Motor Organs, Division of Dermatology, Faculty of Medicine, Tottori University, Tottori, and 2Department of Dermatology, National Hospital Organization Hamada Medical Center, Hamada, Japan. E-mail: itoshio@dermatol.med.kyushu-u.ac.jp
Accepted Mar 8, 2019; E-published Mar 8, 2019
Pegfilgrastim is a granulocyte-colony stimulating factor (G-CSF) that has recently been developed by using the pegylation technology, whereby a polyethylene glycol moiety is attached to filgrastim. Although filgrastim-induced Sweet’s syndrome has been often reported, pegfilgrastim-induced Sweet’s syndrome is rare. Here we report an additional case of neutrophilic dermatosis induced by pegfilgrastim. Moreover, we have confirmed, for the first time, the local expression of G-CSF and we discuss the pathophysiology of the lesion.
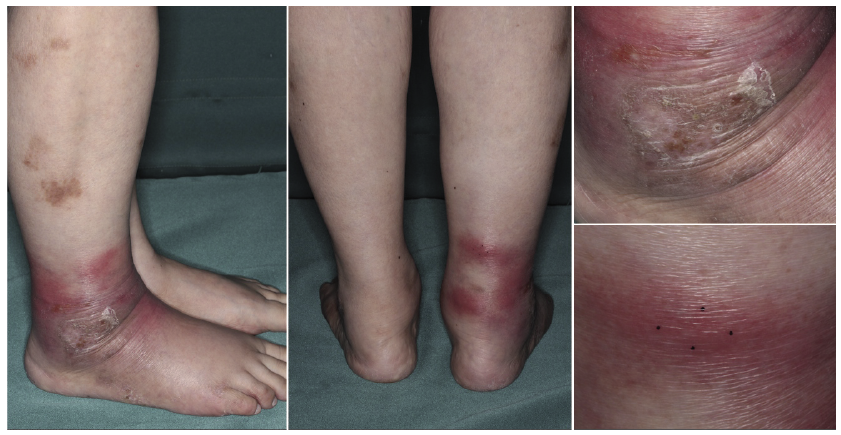
A 59-year-old woman visited us for an evaluation of a red plaque on her right ankle (Fig. 1). She had been diagnosed with breast cancer (cT4bN3aM1, Stag4) at the age of 56 and had been repeatedly treated with adjuvant chemotherapy and lenograstim (a conventional G-CSF) after a right mastectomy with a right axillary lymphadenectomy. To decrease the frequency of injections, lenograstime was replaced by pegfilgrastim. Ten days after the initial pegfilgrastim administration, she observed an eruption on her left ankle. Physical examination revealed a red plaque with a strong induration of the outer side of the right ankle, partly covered with crusts and scales (Fig. 1). Her body temperature was 37.1°C, and she had no palpable lymph nodes. Pertinent laboratory findings included a white blood cell (WBC) count of 18.0 × 103/µl with 91% neutrophils and 6% lymphocytes. C-reactive protein level was 2.77 mg/dl. Histopathologically, the biopsy specimen showed lobular neutrophilic panniculitis, without fat necrosis and a lack of nodular granulomatous phlebitis, and a dense mixed cellular infiltration, mainly composed of polymorphonulear leukocytes in the deep dermis and subcutis (Fig. 2a, b). There was also an aggregation of histiocytes (Fig. 2c). Immunohistochemically, G-CSF was detected in the cytoplasm of the infiltrating histiocytes (Fig. 2d).
Fig. 1. A red plaque with strong induration of the outer side of the right ankle partly covered with crusts and scales.
Fig. 2. Histopathology of the lesion. A: Hematoxylin and eosin (H&E) stain. A magnified image. Lobular neutrophilic panniculitis in the deep dermis and subcutis was observed. B: H&E stain, x400. Dense mixed cellular infiltration mainly composed of polymorphonuclear leukocytes. C: H&E stain x200 Histio-cytes and lymphocytes were also aggregated. D: Immuno-histochemical staining of G-CSF, x400. G-CSF was detected in the cytoplasm of the infiltrating histocytes.
Recently, diagnostic criteria for the drug-induced Sweet’s syndrome have been established, separately from those for the classic Sweet’s syndrome (1). According to these criteria, we could not make a diagnosis of the drug-induced Sweet’s syndrome because she was afebrile. Other conditions, including clinical findings, underlying cause and clinical course, fulfilled the criteria. The differential diagnosis should include erythema nodosum and erythema induratum. However, the present case shows a predominantly lobular panniculitis and a lack of a granulomatous vasculitis of arterioles, lack of fat necrosis, and a lack of nodular granulomatous phlebitis exclude these diagnoses (2–4).
Finally, we made a diagnosis of subcutaneous neutrophilic dermatosis comparable to Sweet’s syndrome. The lesion spontaneously and rapidly cleared within 2 weeks without any special treatment except for the cessation of pegfilgrastim. Instead, treatment with lenograstim was restarted and similar symptoms have not been observed for over 1 year.
We have presented a case of subcutaneous neutrophilic dermatosis comparable to Sweet’s syndrome, induced by pegfilgrastim and the existence of G-CSF in the tissue. G-CSF-induced neutrophilic dermatoses, including Sweet’s syndrome, have been often reported (5). How-ever, to the best of our knowledge, only 3 cases of Sweet’s syndrome (6–8) and one case of pyoderma gangrenosum (9) induced by pegfilgrastim have been reported so far (Table SI). There was no difference in the clinical course or symptoms between the pegfilgrastim-induced Sweet’s syndrome and the conventional G-CSF-induced Sweet’s syndrome. Although, in some patients, when the conventional G-CSF was replaced by pegfilgrastim, only the pegfilgrastim evoked Sweet’s syndrome. Moreover, in all of the patients shown in Table SI, neutrophilic dermatosis developed after the first administration of pegfilgrastim. Because 20-kD polyethylene glycol is attached to the 18.8-kD filgrastim in the pegfilgrastim preparation, it is hardly cleared by the kidney. Instead, it is removed by neutrophils through a receptor-mediated pathway. This difference in clearance may influence the onset of symptoms (6).
Although the pathogenesis of Sweet’s syndrome and other neutrophilic dermatoses remains unclear, the immunologic theory is being favored, recently. It has been hypothesized that the Th1 type cytokines, such as interleukin 1 (IL-1), stimulate macrophages to secrete more G-CSF, which causes Sweet’s syndrome (10). This hypothesis is supported by the frequent induction of Sweet’s syndrome by G-CSF. Furthermore, Kawakami et al. (11) showed that serum G-CSF levels were elevated in the active phase of Sweet’s syndrome and Behcet’s disease. Our data reveal the expression of G-CSF in histiocytes, which can be the new evidence to help elucidate the patho-genesis of Sweet’s syndrome. Thus, we assume that the present case was developed by a pathogenesis similar to that of Sweet’s syndrome. However, the exact mechanism of the development of neutrophilic dermatosis by injected G-CSF, still remains unknown. Accumulation of similar cases and further experiments are needed.
In summary, we report a rare case of pegfilgrastim-induced neutrophilic dermatosis, comparable to Sweet’s syndrome, probably related to the local G-CSF in the pathogenesis of Sweet’s syndrome.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize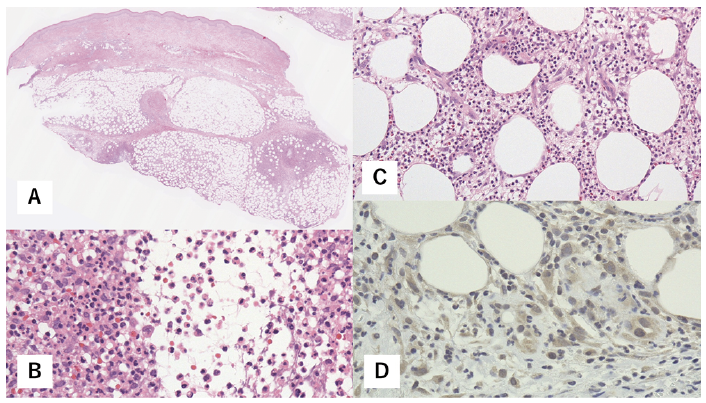 Click to show fullsize
Click to show fullsize