


1Department of Dermatology, Medical University of Vienna, Vienna, Austria, 2The Netherlands Comprehensive Cancer Organization, Eindhoven, The Netherlands, 3Department of Dermatology, University Hospital of Athens, Athens, Greece, 4University Hospital Birmingham, Birmingham, UK, 5Department of Clinical Psychology, General Hospital of Vienna, Vienna, Austria, 6Department of Dermatology and Allergology, Kantonspital St. Gallen, St. Gallen, Switzerland, and 7Italian Group for Adult Hematologic Diseases, Data Center and Health Outcomes Research Unit, Rome, Italy
Previous studies have reported that primary cutaneous lymphomas profoundly influence patients’ health-related quality of life (HRQoL). However, assessment of this psycho-social concept is not common in routine patient care unless required within clinical trials. The aim of this review is to provide a comprehensive overview of HRQoL measures and outcomes in cutaneous lym-phomas in order to inform clinicians. Advanced-stage cutaneous lymphomas were found to be associated with worse HRQoL than early-stage disease. Specifically, progression of the disease, age, sex, psychosocial issues, educational level and therapy were related to the extent of impairment of HRQoL. Treatment response was linked to improved HRQoL, but notably ameliorated HRQoL scores were also reported despite objective disease response. However, the variety of instruments applied to measure HRQoL in cutaneous lymphomas makes it difficult to compare data directly. In conclusion, speciality-specific HRQoL instruments were superior to generic ones, which probably failed to recognize small, but relevant, changes, demonstrating the need for a disease-specific tool.
Key words: health-related quality of life; quality of life; primary cutaneous lymphomas; patient care; quality of life questionnaires.
Accepted Mar 13, 2019; E-published Mar 14, 2019
Acta Derm Venereol 2019; XX: XX–XX.
Corr: Constanze Jonak, Department of Dermatology, Medical University of Vienna, Waehringer Guertel 18-20, AT-1090 Vienna, Austria. E-mail: constanze.jonak@meduniwien.ac.at
Patients’ health-related quality of life can be impaired physi-cally or psychologically due to symptoms and/or vis-ible lesions of dermatoses. Therefore, assessment of health-related quality of life is of significant importance in patients with primary cutaneous lymphomas, which profoundly influence patients’ health-related quality of life in terms of a visible stigma and its potential lethality. Health-related quality of life in patients with cutaneous lymphomas should be considered a vital sign in the face of predominately palliative therapeutic settings. This review provides an overview of health-related quality of life data, in order to highlight the necessity of patient-reported outcomes within clinical trials and to consider the concept of health-related quality of life in routine care.
Quality of life (QoL) is a broad concept incorporating all aspects of an individual’s existence. Health-related quality of life (HRQoL) is a subset relating only to the health domain of that existence (1). Health implies “a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity” according to the WHO’s definition (2). In line with this, HRQoL is understood as an individual perception of one’s position in life, related to culture and value systems (3), and therefore may vary due to cultural and geographic differences (4, 5). HRQoL can be measured with questionnaires completed by patients themselves. Generic instruments attempt to provide a summary of HRQoL, while specific ones focus on individual diseases, patient groups, or areas of function. To gain significant data on HRQoL, measures must be both responsive/reliable (high ratio of signalling) and valid (measuring for the intended purpose) (6). Meanwhile, questionnaires scoring individual disease-related conditions are standard tools and mandatory in clinical trials (7) to evaluate changes in patients’ HRQoL in context with the efficacy of new (cancer) drugs.
HRQoL in clinical dermatology is of particular importance, although there are few life-threatening conditions. Nevertheless, the majority of dermatoses impair patients’ lives in a physical, emotional and functional manner (8). Thus, previous studies have reported a high mental burden in patients with psoriasis, eczema, cutaneous lupus erythematodes, non-melanoma skin cancer and actinic keratosis, all representing chronic dermatoses with visible stigmas (9–12).
This review emphasizes the aspects of HRQoL in primary cutaneous lymphomas (CL), a heterogeneous group of clonal lymphoproliferative skin disorders of T-cell (CTCL) and B-cell (CBCL) origin (13); subtypes are recorded in the World Health Organization – European Organization of Research and Treatment of Cancer (WHO-EORTC) classification (14). CBCL (25%) mostly show an indolent course and CTCL (75%) also predominantly have an excellent prognosis in the early stages. In contrast, advanced-stage disease (25–33%) is associated with a 5-year survival rate of 0–39% (13–16). Patients frequently experience agonizing pruritus (60–90%) (17) and chronic skin alterations, with profound influence on HRQoL (18–21). Moreover, the diagnosis of CL demoralizes patients due to incurability, restricted therapeutics, and limited responses. In brief, patients with CTCL experience a disfiguring and potentially lethal disease, which highlights the importance of consistently assessing and monitoring HRQoL in these patients. The objectives of this review were: (i) to provide an overview of HRQoL tools that are used in CL; and (ii) to summarize and review available HRQoL data on patients with CTCL and those with CBCL in order to highlight psycho-social aspects of this orphan disease.
A state-of-the-art literature search was performed in PubMed, Medline, and Web of Science databases using the search terms (both alone and in combination with): “quality of life”, “health-related quality of life”, “dermatology”, “skin disease”, “primary cutaneous lymphomas”, “primary cutaneous T-cell lymphomas”, “primary cutaneous B-cell lymphomas”, “pruritus”, “illness perception”, “quality of life questionnaires”, and “health-related quality of life questionnaires”. The search was limited to “English” language, dated between January 1980 and January 2018. Furthermore, references from retrieved articles were searched manually to identify additional literature meeting the study criteria. Publications about the predefined subject of (health-related) QoL in general or related to dermatology and primary CLs were included, contributing to a total of 58 references. Ten studies reporting on HRQoL in CL were included in a precise analysis.
Several questionnaires have been used to measure HRQoL in CL. The Dermatology Life Quality Index (DLQI), published in 1994, was the first specialty-specific HRQoL measure (22). The DLQI measures disability in patients with dermatological conditions, providing a simple and practical method to score the impact of skin disease. Thereupon, the Skindex-29 and shorter version Skindex-16 were developed to measure patients’ experiences of illness (23, 24) and, additionally, the impact of disease-specific treatment on patients’ HRQoL. Skindex-29 assesses 3 domains, describing symptoms, functioning, and emotions on a 5-point Likert-type scale, ranging from “never” to “all the time”. Responses are transformed to a linear scale of 100, varying from 0 (no effect) to 100 (effect experienced all the time). Scores are reported as 3 scale scores, with each scale score representing the mean of patient’s responses to items in a given domain. Higher scores indicate poorer HRQoL. Valuable information can be obtained by comparisons of mean scores among patient groups with certain diseases (25, 26). Skindex-29 and Skindex-16, along with the (not validated) specific CTCL QoL questionnaire by Bisaccia (27) and the following generic tools have been used for the purpose of HRQOL in CTCL (28): the 36-Item Short Form Health Survey (SF-36) (29), Functional Assessment of Cancer Therapy General (FACT-G) (30), Quality of Life Core Questionnaire (EORTC QLQ-C30) (31), General Heath Questionnaire (GHQ-12) (32) and Spitzer Quality of Life Index (Spitzer QLI) (33).
In general, improving HRQoL is one of the treatment goals, besides improving survival, preventing progression/infection, and minimizing toxicity of treatment. Symptoms of CL (itch, shedding, pain), self-appearance (visible lesions/stigma), health worries and distress (cancer diagnosis) and psychosocial issues (relationships, livelihood, leisure) interact mutually and unavoidably with HRQoL.
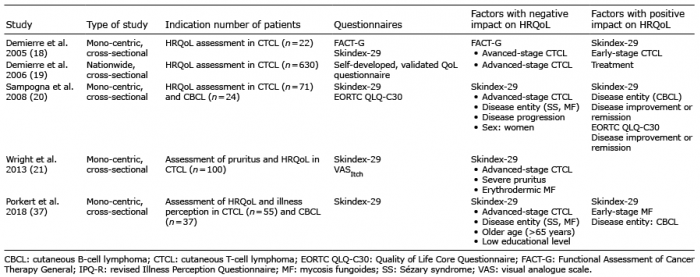
Tables I and II briefly summarize the results of the 10 studies on HRQoL in CL assessed within both epidemiological and clinical trials.
Table I. Assessment of health-related quality of life (HRQoL) in cutaneous lymphomas in epidemiological studies
Table II. Assessment of health-related quality of life (HRQoL) in cutaneous lymphomas in clinical trials
Epidemiological studies (n = 5). Demierre et al., in 2005 (18), were the first to publish on reduced HRQoL in CL (34). By combining Skindex-29 and FACT-G, both general health concepts and specific issues relevant to patients with CTCL were addressed. This mono-centre, cross-sectional HRQoL study of 22 patients with CTCL showed that advanced disease was significantly associated with more effects on general health (FACT-G), particularly in the physical, emotional and functional domains (18). In contrast, early-stage patients had better scores for HRQoL overall and for each specific domain. Moreover, the HRQoL of patients with CTCL was more impaired compared with FACT-G results for non-melanoma skin cancer historical controls.
A follow-up study by Demierre et al. in 2006 (19) included a 4-page self-administered questionnaire comprising 5 domains (symptoms, functioning, emotions, health distress, satisfaction with treatment), which was collected either online or by post. Respondents (n = 630) predominantly had mycosis fungoides (MF; 89%), the most common form of CTCL (35), followed by the CTCL subtype Sézary syndrome (SS) (4%) and CD-30-positive lymphoproliferative disorders (2%). The median age of respondents was 57 years, with the majority being white. The survey concluded that health distress was significant in CTCL, with 94% worrying about prognosis and 80% about dying from the disease. Furthermore, the emotional and functional impact was evident, as 88% of respondents reported itch, 66% were affected by choice of clothes and sleep disturbance/fatigue, and 62% experienced psychosocial effects (depression, frustration, anger). HRQoL scores (n = 245) were worse in advanced-stage disease (IIB–IV) vs. early-stage (IA–IIA). Eighty-five percent of respondents reported that their treatment made their disease seem more manageable, but 61% felt financially burdened (19), which was verified recently by risk adjustment showing that CTCL consistently ranked in the top 3 positions of financial burden due to skin diseases (36). Wright et al. (21) confirmed these data, showing that advanced-stage disease and more severe pruritus were associated with poorer HRQoL in CTCL. However, the findings of HRQoL research should guide our practice, with the ultimate goal of improving patients’ lives as they relate to therapy either positively or negatively, and even the dimension of spirituality as a component of the dying process should be considered (19, 34).
Sampogna et al. (20) were the first to include CBCL (n = 24) in addition to patients with MF/SS (n = 71) using the Skindex-29 and EORTC QLQ-C30. HRQoL was evaluated and related to disease entity, disease stage, sex, age, psychosocial status, and disease-specific
therapy. HRQoL was worse in SS, followed by MF and CBCL, with impairment in the scales for symptoms and emotions in both MF/SS and CBCL. Comparison of Skindex-29 mean scores with other dermatological diseases showed highest scores for SS, followed by psoriasis, MF and vitiligo. Although benign, psoriasis and vitiligo are highly visible and therefore have a similar impact on patients’ psychosocial life to CTCL, as mentioned previously. Impairment in HRQoL was associated with disease stage, with higher stages having worse HRQoL scores. HRQoL was worse in women than in men, in patients with probable anxiety or depression, and when the disease progressed. In patients treated with systemic steroids and interferon the prevalence of probable anxiety or depression was highest. The most frequent items reported in Skindex-29 were itch, being troubled by the disease, worrying about worsening of the disease, affected interactions, and impaired sexual life. The EORTC QLQ-C30 analysis revealed that fatigue, pain and insomnia were the most frequent problems. Sampogna stated that, not only the total score, but also relationships between HRQoL and clinical variables and treatment may provide important information.
The clinical relevance of the relationships between illness perception and HRQoL in CTCL and CBCL were investigated recently (37). The Revised Illness Perception Questionnaire has been shown to assess illness perception reproducibly in CTCL (38). Illness perception reflects patients’ individual concepts of understanding and interpretation of the disease (39–41). Illness perception affects HRQoL (39, 42–45), which, in turn, is influenced by how patients with cancer perceive and respond to their illness (46). The study by Porkert et al. in 2018 (37) comprised 55 patients with CTCL and 37 with CBCL, illustrating that illness perception was significantly associated with HRQoL. Both illness perception and HRQoL correlated with disease entity, stage and socio-demographics. The highest impairment in HRQoL was found in advanced MF/SS and lowest in CBCL, with significance between early-stage MF and advanced MF/SS in Skindex-29 total (sum of the 3 scales) and functioning. This finding implicates that patients with advanced MF/SS are more compromised in their daily routines. Moreover, stage-dependent correlation in MF/SS was found for Skindex-29 total, symptoms, and functioning. In addition, older age (> 65 years) and low educational level (without qualification for university) were associated with a significantly worse (higher) HRQoL scores in emotions. For data visualization, available raw data for Skindex-29 scores for the 3 studies mentioned above (18, 21, 37) are shown graphically and, for comparison, in spider charts in Fig. 1. It is evident that HRQoL, reported by the latest study from 2018 (37), was more affected than shown in previous publications (18, 20, 21), which might be explained by different patient characteristics and socioeconomic factors, ongoing lifestyle changes (47, 48), and growing health consciousness besides cultural and geographical differences (4, 5) or selection bias. However, reproducible information was gathered, as 80% of respondents reported worrying about the seriousness and progression of the disease and 50% were bothered by sleeping disorders, difficulties at work or leisure, and social life (37).
Fig. 1. Spider chart showing a direct comparison of the 3 Skindex-29 domains emotions, symptoms, and functioning in 3 different health-related quality of life (HRQoL) studies (18, 21, 37). (a) Comparison of all patients with cutaneous T-cell lymphoma (CTCL) (stage IA–IVB), (b) early-stage (IA–IIA), and (c) advanced-stage CTCL patients (IIB–IV). Data indicate higher HRQoL impairment in advanced-stage CTCL and that patients reported by Porkert et al. 2018 (37) were more affected among all Skindex-29 domains compared with 2 previously published studies.
Clinical studies (n = 5). HRQoL is a patient-reported outcome in clinical trials, used to document whether study drugs are able to improve HRQoL from the perspective of patients. For this purpose, HRQoL measurements provide valuable information on the benefit-risk assessment, not at least for regulatory authorities (7).
Table II summarizes 5 clinical studies on HRQoL assessed as a secondary endpoint. The clinical study by Duvic et al. in 2002 (49), reporting on HRQoL in advanced and/or recurrent CTCL, is a multicentre, randomized phase III trial. In total, 71 patients receiving the study drug denileukin diftitox (objective response rate (ORR)=31%) completed the FACT-G questionnaire, assessed skin appearance on a 7-point scale, and pruritus severity with a VAS. In documented responders (n = 21) HRQoL increased gradually during the study period, generally reaching statistical significance after 3 cycles of therapy, and was significantly higher than in non-responders at endpoint. In addition, for responders, assessments of skin severity and pruritus severity showed significant improvements at study endpoint compared with baseline (49), demonstrating that HRQoL improvement is linked to the efficacy of therapy.
Another clinical trial by Duvic et al. in 2001 (50) assessed HRQoL using the Spitzer QLI and a not validated CTCL-specific instrument in the approval study of bexarotene (ORR 45–55%), an oral rexinoid, in patients with CTCL (IIB–IVB). The CTCL status evaluated with the specific tool was improved in 79–82%, and 72–91% reported treatment satisfaction, both regardless of clinical response in advanced-stage disease.
Similar results with the same questionnaires were obtained by Heald et al. in 2003 (51) for topical bexarotene (ORR 54%) in 50 patients with CTCL diagnosed with early-stage CTCL. No detailed information is available on the CTCL-specific HRQoL tool used in both studies. However, another not validated CTCL-specific HRQoL questionnaire was applied by Bisaccia et al. in 2000 (27) in a single institution, retrospective study in 69 patients with CTCL (IB–IV) receiving extracorporeal photochemotherapy (ECP; photopheresis) alone or with adjuvant therapy (ORR 54%). This specific tool comprises 20 items split to 4 domains (physical function, social function, psychological function, general well-being) with 4 possible answers for each question, ranging from 0 (a lot/poor) to 3 (none/excellent). Comparison of concurrent skin stages was used to test the validity of the questionnaire, but there were no data on reliability, test–retest reliability, internal consistency, or responsiveness to change. The latest clinical trial by Prince et al. in 2017 (52) for CD-30-positive CTCL, comparing Brentuximab vedotin (BV) with physician’s choice of methotrexate or bexarotene (ORR4=56.3%, lasting at least 4 months) applied Skindex-29 and FACT-G to measure HRQoL as defined secondary key endpoints. FACT-G revealed no differences between the 2 treatment arms for total or any subscale score. In contrast, Skindex-29 showed that patients who received BV reported significantly greater symptom reduction compared with the physician’s choice group. No substantial difference in Skindex-29 domains emotions and functioning were observed over time, but skin disease at the end of treatment had less of an effect in the BV arm for both domains. This demonstrates that a generic HRQoL tool, FACT-G, failed to capture information that was retrieved only by the Skindex-29, a specialty specific instrument.
Clinicians and policymakers recognize the importance of measuring HRQoL in order to inform patient management and policy decisions, but challenges remain in selecting the most appropriate HRQoL questionnaire for use in a specific setting. It is suggested that HRQoL tools should measure the current gap between one’s hopes and expectations based on the individual’s experiences. HRQoL can only be described by the individual and must take into account many aspects of life (6, 53). A critical and comprehensive review of HRQoL in CL, describing the past and present situation, is therefore paramount for future scientific development in this field.
The current review examined HRQoL data obtained within both epidemiological and clinical studies. Conclusions drawn from clinical trials assessing HRQoL are limited to determine whether HRQoL changes upon treatment (Table II), whereas epidemiological studies primarily aim to identify socio-demographic factors associated with changes in HRQoL (Table I) (18–21, 37). Thus, HRQoL is significantly impaired in CTCL and reduced in CBCL and indolent CL subtypes (18–21, 37). Moreover, disease entity (20, 37), disease stage (18–21, 37), disease progression (20), age (37), sex (20), psychosocial issues (20), educational level (37), and therapy (20) are related to the extent of impairment of HRQoL. It is notable that HRQoL in CTCL compared with psoriasis was similar in the functioning domain and better in emotions and symptoms. HRQoL research in psoriasis revealed that patients with psoriasis experience the same deterioration in HRQoL as those with other serious chronic diseases, including cancer (54). Furthermore, treatment success was linked to ameliorated HRQoL scores (27, 49, 52) (Table II), although it is noteworthy that HRQoL also improved without an objective treatment response (50). HRQoL scores were unchanged throughout one study, implicating that the applied measure failed to recognize small changes in patients’ HRQoL despite reported treatment satisfaction (51). Thus, we conclude that a disease-specific HRQoL tool addressing disease-relevant issues might serve best to assess and monitor HRQoL in CL.
PatientsLikeMe® and Actelion® developed the MF/SS-specific HRQoL tool, validated in a small sample size skewed towards early-stage disease, which might not be representative for advanced-stage CTCL. Discrimination between low and high levels of HRQoL interference, correlation with Skindex-29 and disease stage, and no evidence of significant bias based on age, sex, or ethnicity were stated by the authors (55).
Interestingly, question 5 queries how confident the patients felt in managing their disease, which might even be related to illness perception. Perceiving personal control (over the disease) is associated with better adherence to therapeutic regimens in patients with hypertension (56). Therefore, confidence in managing one’s disease might help to improve adherence to treatment by supporting patients’ self-control (38). However, the self-administered CTCL-specific questionnaire by Bisaccia et al. (27) comprised unique items within its psychological domain compared with Skindex-29. This non-validated tool specifically queries worries about dying, difficulties with treatment regimens, financial hardship, and treatment satisfaction. Difficulties in following treatment regimens or satisfaction with therapy are obvious issues that are important to patients with CTCL and thus patients’ perspective of treatment should also be taken into account when evaluating HRQoL. In line with this, total skin electron beam is perceived to be a successful therapy for CTCL, although is difficult to undergo and recover from compared with other treatments (57).
Interestingly, no HRQoL instruments were used in the multicentre approval trial comparing mechlorethamine gel with mechlorethamine ointment (58). Currently, a number of HRQoL tools are used in clinical trials, typically 3, to capture the generic, skin, emotional, functional, and pruritus impact of the disease. The variety of instruments applied to measure HRQoL in these patients makes it difficult to compare HRQoL data among clinical trials and epidemiological studies. Issues of elaborate diagnosis and treatment, disease progression, mortality, isolation, and financial burden should also be taken in account when evaluating patients’ HRQoL. Therefore, a validated disease-specific instrument to measure HRQoL in patients with CL, which is suitable for early and advanced-stage disease, is highly needed.
Therapeutic success is associated with improvement in HRQoL in CTCL (49, 50, 52), but disease management in CL remains challenging, not least because of chronicity and a not durable treatment response. The fact that ameliorated HRQoL was reported by patients without objective response (50) raises the questions whether HRQoL scores should be considered when calculating the disease response, or whether HRQoL might be implemented as a primary endpoint in clinical trials. Moreover, elucidating patients’ overall HRQoL might be as important as analysing each question within a questionnaire in order to identify problematic issues that should be addressed to improve patient care.
In daily clinical routine the assessment of HRQoL is not very popular, probably due to a lack of information, oversupply of (generic) HRQoL tools, and/or its foreseen time-consuming process. However, intensified physician-patient communication might be sufficient to capture HRQoL for the purpose of clinical practice, without the need for the data reproducibility and comparability that is required in clinical studies. Nevertheless, assessment of HRQoL and/or detailed personal conversations with patients are essential in order to determine the psycho-social impact of the disease, which is a step towards improving patients’ HRQoL.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize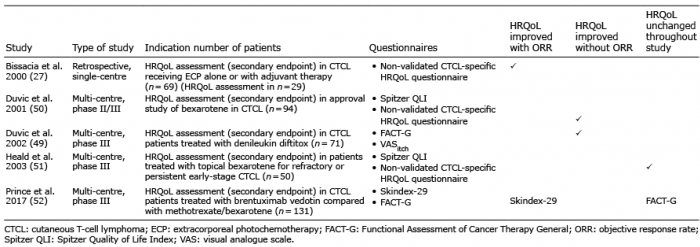 Click to show fullsize
Click to show fullsize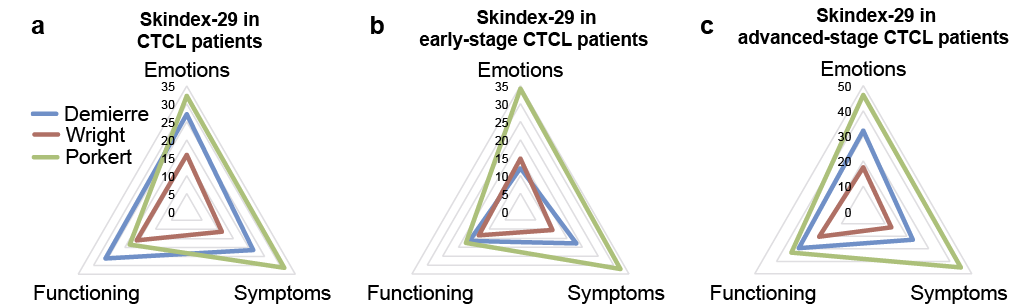 Click to show fullsize
Click to show fullsize