


1Center for Dermatoepidemiology-111D, Veterans Affairs Medical Center, 830 Chalkstone Avenue, Providence, RI 02908-4799, 2Department of Dermatology, Alpert Medical School of Brown University, Providence, RI, 3George Washington University School of Medicine, Washington, DC, and 4Department of Dermatology, Medical College of Wisconsin, Milwaukee, Wisconsin, USA. E-mail: mbeatson@gwu.edu
Accepted Mar 21, 2019; E-published Mar 21, 2019
It was recently reported that 5-fluorouracil (5-FU) is effective for prevention of squamous cell carcinoma (SCC) for one year, but not for basal cell carcinoma (BCC) (1). Additionally, a history of 5-FU exposure has been associated with more aggressive BCC subtypes, and we wanted to confirm this finding prospectively by determining the influence of 5-FU on the histopathologic characteristics of BCC and SCC (2). We evaluated whether 5-FU was effective for prevention of specific subtypes of BCC or SCC or was effective in specific subpopulations of our high risk group of veterans with at least 2 prior keratinocyte carcinomas (KCs) in the Veterans Affairs Keratinocyte Carcinoma Chemoprevention (VAKCC) Trial.
The VAKCC Trial followed 932 veterans at high risk for development of KC for a median of 2.8 years, where participants were randomized to apply topical 5-FU or vehicle control cream to the face and ears twice daily for up to 4 and at least 2 weeks (1). All participants were free of suspicious skin lesions suggestive of any type of skin cancer at the initial full body skin examination. Total body skin examinations, with biopsies as clinically indicated, were performed every 6–12 months. All skin biopsies were read by a single central board-certified dermatopathologist. The Veteran’s Affairs Central Institutional Review Board approved this trial, all participants gave written, informed consent, and Declaration of Helsinki Principles were followed, as described elsewhere (1).
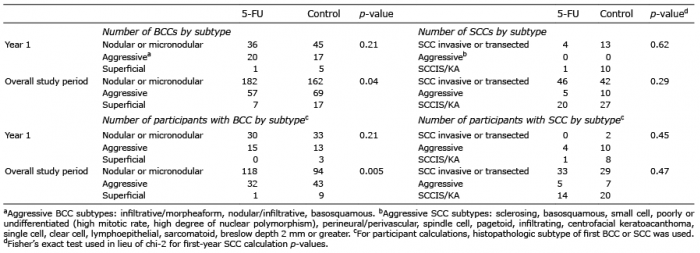
Data for patient age, tumor size, anatomic location, and histopathologic subtypes were collected (1). Anatomic locations were first divided into left and right halves of the head, and then sub-classified based on eye, ear, nose, cheek, chin, forehead, temple, or mouth location. Histopathologic subtypes were classified according to commonly utilized dermatopathology criteria noted in the legend of Table I (3).
Table I. Histopathologic subtype of basal cell carcinoma (BCC) and squamous cell carcinoma (SCC)
All analyses were done using Stata statistical software (release 8.0, StataCorp, College Station, TX). To determine the characteristics of BCC and SCC in year 1 and overall, t-tests were performed comparing 5-FU to control groups for lesion size by individual participant and total lesion count. Age was stratified a posteriori into “very old” ≥ 85 years old, as defined by Linos et al. (4) and “not very old” (< 85 years old). Pearson’s chi-squared tests and Fischer’s exact tests were performed comparing 5-FU to control groups for development of BCC and SCC by location and histopathologic subtype by participant and total lesion count in year 1 and overall. We assigned an alpha value of 0.05. This alpha value should be interpreted in the context of our exploratory examination with multiple comparisons performed.
Participants had a mean age of 71.1 years and 98% were men (1). There were no significant differences between the 5-FU and control groups with respect to other demographic characteristics such as age, education, military service history, self-reported Fitzpatrick skin type, sunburn, marital status, geographic residence, weight, height, or skin cancer history, as previously reported (1).
There were fewer superficial BCCs in the 5-FU group vs. control group (Table I). In year 1, there was a smaller number of total BCCs among those at least 85 years old in the 5-FU group vs. control group, but there was no substantial difference in the risk of these individuals at least 85 years old developing a BCC (Table II). One of the BCCs in the participants ≥ 85 years old was superficial type. Among the same elderly group, there was also a smaller number of SCCs in the 5-FU group vs. control group, but the reliability of either of these findings is uncertain given the multiple comparisons and small numbers (Table II). There were no differences between the 5-FU and control groups for mean age of development, mean size, and anatomic location of the tumor.
We were unable to confirm a previously reported association of more aggressive BCC subtypes with a history of 5-FU exposure (2)
Table II. Age, stratified into ≥ 85 years old vs < 85 years old
Our findings suggest that 5-FU may be effective for the prevention of superficial subtype of BCCs even though there was no effect on BCCs overall (1). 5-FU has an indication for treatment of superficial BCCs although 5% imiquimod cream may be superior for that purpose (5–8).
5-FU may additionally mitigate BCC risk in the ≥ 85 year old population, although this finding is much less clear due to possible inadequate powering of the study. The decrease in risk of BCCs in participants ≥ 85 years old treated with topical 5-FU suggests that this elderly population may derive the most benefit from 5-FU. Furthermore, given concerns that very old adults may not require aggressive surgical treatment for slow-growing skin cancers such as BCC, these results highlight how 5-FU may decrease the need for costly and labor intensive surgical treatments for BCC (4, 9, 10).
Strengths of this double-blinded randomized control trial include its longitudinal follow-up and standardized histopathologic analysis. Despite the large size of the VAKCC trial, sample sizes for individual histopathologic subtype and anatomic location subpopulations may not have been large enough to detect more subtle effects of topical 5-FU in these subgroups. Another limitation is the relative homogeneity of the study population in age and particularly gender, which prevents generalizability of these results to other groups. Generalizability is also limited by the post-hoc analyses.
Funding and support: This study was supported by the Office of Research and Development Cooperative Studies Program, US Department of Veterans Affairs.
Trial registration: ClinicalTrials.gov: NCT00847912.
Information about key personnel of the VAKCC Trial is listed in Appendix S1.
Conflict of interest: MW served as a consultant to AbbVie and Celgene. These pharmaceutical companies were not involved in design and conduct of the study, collection/management/analysis/interpretation of the data, preparation/review/approval of the manuscript, or decision to submit the manuscript for publication.
The other authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize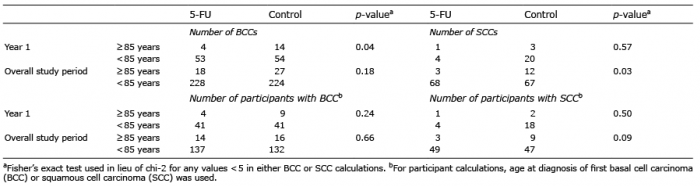 Click to show fullsize
Click to show fullsize