


1Department of Dermatology, Iwate Medical University School of Medicine, 19-1 Uchimaru, Morioka, Iwate 020-8505, and 2Institute for Environment and Gender-Specific Medicine, Juntendo University Graduate School of Medicine, Urayasu, Chiba, Japan. E-mail: dwatabe@iwate-med.ac.jp
Accepted Mar 21, 2019; E-published Mar 21, 2019
Psoriasis is an immune-mediated chronic inflammatory skin disorder in which the IL-23/Th17 pathway is considered to play a major pathogenetic role (1). However, recent studies have found evidence for interaction between the immune and nervous systems in the pathogenesis of psoriasis. We report here a case of psoriasis in which unilateral remission of the lesions was observed following myelopathy due to spinal arteriovenous malformation resulting in hypoesthesia of the right leg.
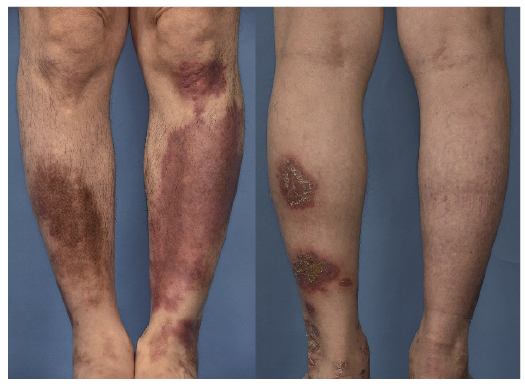
The patient was a 51-year-old Japanese man with a 10-year history of plaque psoriasis involving the trunk and bilateral lower extremities. He had been treated with topical betamethasone dipropionate and calcipotriol. Four years before presentation, he had gradually developed muscle weakness and atrophy of the right lower limbs, as well as hypoesthesia behind the right knee. Neurological examination revealed weakness of the right iliopsoas muscle, quadriceps femoris muscle, hamstrings, anterior tibial muscle and gastrocnemius muscle. Hypoesthesia and hypopallesthesia were noted in the right lower limb. The right Achilles reflex was absent. Spinal magnetic resonance imaging (MRI) revealed evidence of a spinal arteriovenous malformation (AVM) in the upper thoracic and lumbar region, and a diagnosis of myelopathy due to spinal AVM was made. At that time, physical examination revealed erythematous, indurated, slightly scaling plaques on the trunk and lower limbs. Interestingly, remission of the psoriatic plaques on the right knee and leg was observed (Fig. 1). The area of skin lesions on the right side largely resembled that on the left side before paresis. Three biopsy specimens were taken from the psoriatic plaque on the left leg, non-lesional skin on the left leg and a skin area showing remission of the psoriatic plaque in the area of neuropathy in the right leg. Histological examination of the biopsy specimen of psoriatic plaque revealed hyperkeratosis and elongation of the rete ridges with epidermal hyperplasia. An immunofluorescence study showed that nerve fibres immunoreactive for the general neuronal marker, protein gene product 9.5 (PGP 9.5), were present mainly in the papillary dermis and increased in the psoriatic plaque relative to the non-lesional skin (Fig. 2a, Figs S1a and S2a) (for details of Materials and Methods, see Appendix S1). Intraepidermal nerve fibres were seen in the skin area showing remission on the paretic leg (Fig. 2a, Figs S1c and S2c). PGP9.5-immunoreactive nerve fibres were almost absent in the non-lesional skin (Fig. 2a, Figs S1b and S2b). Nerve fibres immunoreactive for PGP9.5/Substance P (SP) and PGP9.5/calcitonin gene-related peptide (CGRP) were mainly present in the dermis and increased in the psoriatic plaque relative to the skin area showing remission on the paretic leg and almost absent in the non-lesional skin (Fig. 2b, c, Figs S1 and S2).
Fig. 1. Remission of psoriasis on the right knee and leg following myelopathy due to a spinal arteriovenous malformation resulting in hypoesthesia of the right leg.
Fig. 2. Semiquantitative analyses of the number of PGP9.5 (a), PGP9.5/SP (b) and PGP9.5/CGRP (c) immunoreactive nerve fibres in the psoriatic plaque, non-lesional skin and paretic skin. Values represent the means ± standard deviation (SD) of 9 specimens of each skin and were compared by 1-way analysis of variance (ANOVA) with Bonferroni’s comparison. *p < 0.05, **p < 0.01, ***p < 0.001.
To date, several case reports have described psoriatic lesions with acquired central or peripheral nerve damage that exhibited unilateral local clearance or improvement (2). Consistent with those clinical reports, another study using a murine model of psoriasis demonstrated that loss of cutaneous innervation via traumatic nerve injury resulted in reduction of the clinical symptoms of psoriasis (3). Immunohistochemical studies have revealed an increased cutaneous nerve density and overexpression of neuropeptides, such as SP, CGRP, vasoactive intestinal peptide (VIP), PGP 9.5 and nerve growth factor (NGF), in psoriatic plaques (4). Among them, SP and CGRP are released in response to activation of transient receptor potential vanilloid (TRPV) 1 in sensory nerve endings to induce neurogenic inflammation (5). SP, an 11-amino-acid peptide, mediates transmission of pain and itch sensation via sensory nerve fibres at the dorsal horn of the spinal cord. SP has a stimulatory effect on keratinocyte proliferation and secretion of IL-1, neutrophil chemotaxis (4), T-cell proliferation, and secretion of IL-2, which increases the Th1 response through dendritic cell (DC) secretion of IL-12 (6). CGRP, a 37-amino-acid peptide, induces microvascular dilatation resulting in increased blood flow and persistent local erythema (4). Exposure of different DCs to CGRP enhances Th2 type immunity, increasing IL-4 production while decreasing the Th1-associated cytokines IFNγ and IL-2 (7). In a murine model, TRPV1+ nociceptive neurons have been shown to be important for activation of dermal dendritic cells, which are necessary for induction of IL-17/23-dependent psoriasiform skin inflammation (8). Taken together, these findings suggest that the neuropeptides SP and CGRP play a major role in neurogenic inflammation, which results in formation of psoriatic lesions.
In the present case, PGP9.5-immunoreactive nerve fibres were increased in psoriatic plaque relative to both non-lesional skin and skin that showed remission on the paretic leg. Furthermore, the psoriatic plaque contained SP-immunoreactive and CGRP-immunoreactive nerve fibres, which were almost absent in healthy and non-lesional skin. These findings suggest that release of SP and CGRP by sensory nerves is inhibited by denervation, and that SP and CGRP release is an important factor in promoting the clinical expression of psoriasis. It is also possible that the decrease in scratching and subsequent koebnerization due to hypoesthesia might have contributed to local improvement in psoriasis.
Our findings in the present case support the concept that the nervous system plays an important role in the pathophysiology of psoriasis, and that neuropeptides are local inflammatory mediators of disease development and maintenance. Further studies to clarify the role of neuropeptides in the process of inflammation in psoriasis may help to open new therapeutic avenues.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize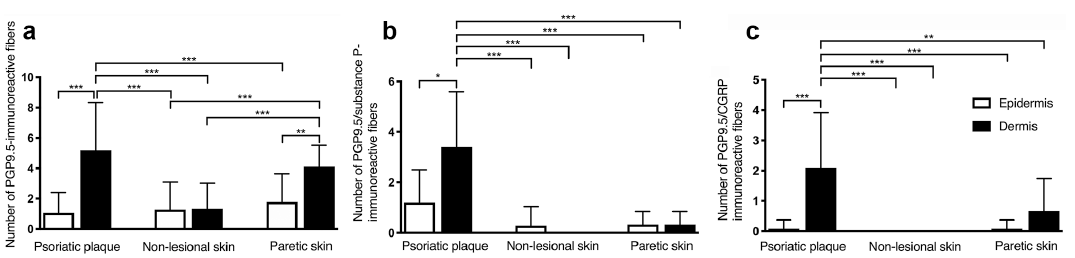 Click to show fullsize
Click to show fullsize