


Departments of 1Dermatology, 2Demography and 3Health Psychology, University Medical Center Groningen, University of Groningen, Groningen, and 4Department of Social Studies, University of Utrecht, Utrecht, The Netherlands
Epidermolysis bullosa (EB) is a group of rare inherited bullous skin disorders that differ in nature and severity. Currently, there is no cure for the disease. One of the complex problems of EB is the repetitive and painful care of skin wounds. The purpose of this study was to explore how adult patients and parents experienced the impact of wound care during childhood and which coping strategies they considered as helping. A qualitative study was performed, comprising semi-structured in-depth interviews with 7 adult patients and 6 parents. The impact, physically, psychologically and on daily life, was apparent for patients and parents. Helpful coping strategies were transferring care, regulating emotions, and dyadic strategies, such as supporting each other by distraction, encouragement, using rituals and collaboration. The most important finding of this study is the need for a more thorough investigation into the effectiveness of dyadic coping strategies.
Key words: chronic illness; parenting; children; skin disorders; wound care; qualitative research.
Accepted Mar 21, 2019; E-published Mar 21, 2019
Acta Derm Venereol 2019; XX: XX–XX.
Corr: Petra J. Mauritz, Department of Dermatology, University Medical Center Groningen, Hanzeplein 1, NL-9700 RB Groningen, The Netherlands. E-mail: p.j.de.graaf@umcg.nl
Wound care in children with epidermolysis bullosa is physically and psychologically stressful both for children and parents. This study aimed to gain an in-depth understanding of how adult patients and parents of adult patients experienced the impact of wound care during childhood and which coping strategies they considered as helping. For children, wound care was associated mainly with pain, itching, and anxiety, while for parents, regulating emotions, such as sadness and powerlessness, was a major issue. Dyadic coping strategies, such as supporting each other by distraction, encouragement, using rituals and collaboration, were reported to be helpful to both children and their parents. Parents and children should learn which coping strategies are helpful for themselves and for each other in the context of wound care.
Epidermolysis bullosa (EB) is a group of rare genetic bullous disorders of skin and mucous membranes. EB is characterized by the absence of a cohesion protein in the skin, so that the cellular layers are poorly connected, resulting in a fragile integument (1). EB can be divided into 4 main types, depending on which layer is affected in the skin: EB simplex (EBS), junctional EB (JEB), recessive dystrophic or dominant dystrophic EB (RDEB or DDEB), and Kindler syndrome.
In the most common variant, EBS, blistering is often limited to the hands and feet. In more clinically severe forms, such as JEB, RDEB and DDEB, blistering can be generalized, affecting both skin and mucosa (e.g. eyes and oesophagus). Wounds heal slowly and lead to scars, skin deformity and disabilities. Life expectancy may vary from normal to shortened, up to early postnatal death (2–4). EB is almost always characterized by pain (5), which can be acute (e.g. from blisters and wounds), chronic (e.g. from inflammation of the skin or contractures) or procedural (e.g. from dressing changes). There is currently no cure for EB. The treatment therefore focuses on supportive care and the prevention of complications (6, 7). EB can lead to impaired quality of life for both the child and the parent (3, 6, 8–12).
One of the reasons for impaired quality of life is the repetitive, time-consuming, and very painful wound care of children with EB. This care, which consists of changing wound dressings and cleaning the wounds, needs to be performed daily or once every 2 days. These recurring sessions can lead to excruciating pain, (anticipatory) anxiety, and a lack of control over the situation for both the child and the parent (4, 11–15). Usually, the parents are responsible for this daily task, which can be very stressful both physically and emotionally (12, 14). Although the challenges that exist in EB wound care are well documented, information regarding how children and parents cope with these challenges is limited.
Coping can be defined as thoughts and behaviours that people use to respond to internal or external stressful demands (16, 17). In the case of EB, stressful wound care cannot be avoided, but the consequences and implications of this care can be changed using coping strategies. These strategies, such as distraction or positive thinking, can help the child and the parent to adapt to the situation. Little is known, however, about which coping strategies are more adaptive than others for children and parents, and how coping strategies of the child affect parents and vice versa (i.e. dyadic coping processes).
The aim of this study was to gain an in-depth understanding of how adult patients and parents of adult patients experienced the impact of wound care during childhood and which coping strategies they considered as helping.
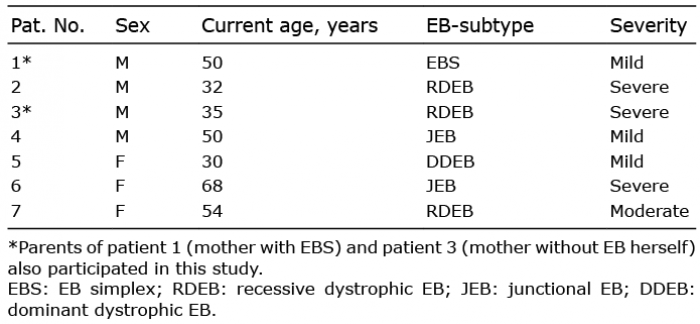
Inclusion criteria were: (i) patients with EBS, JEB, RDEB or DDEB aged > 25 years, sufficiently fluent in Dutch, registered as patient in the Netherlands where the Centre for Blistering Diseases is located, and having experience with wound care; (ii) parents of children with EBS, JEB, RDEB or DDEB aged > 25 years, sufficiently fluent in Dutch, with a child registered as a patient in the Netherlands, and being a parent who performed wound care most frequently. This study is part of a larger research project that also includes a prospective follow-up quantitative study of wound care in children with EB and their parents. As EB is a rare disease and we did not want to put too much burden on participants, we excluded patients under the age of 25 years and parents of patients under the age of 25 years from the qualitative study and invited them to join the questionnaire study. An additional reason was that the patients from the age of 25 years were best able to reflect on wound care during the course of their childhood and adolescence. The principal investigator and fourth author jointly selected 6 patients and 6 parents by using the EB dermatology database. Both within the group of patients and within the group of parents, all forms of EB were included in order to be able to explore coping with all types of wound care. The patients and parents were not relatives of each other. Two parents declined the invitation to participate. Both parents found it emotionally too stressful to talk about the wound care of their child. To supplement the sample, we approached 2 parents of children with the same subtype who agreed to participate. The final sample consisted of 13 participants because one parent dropped out without giving a reason and 2 participants spontaneously asked the investigator during the interview if the parent (EBS) and the patient (RDEB) could also be interviewed. These 2 parent–child dyads were interviewed separately. The characteristics of patients and parents per subtype EB are shown in Tables I and II.
Table I. The characteristics of patients with epidermolysis bullosa (EB) per subtype
Table II. Characteristics of parents to children with epidermolysis bullosa (EB) per subtype
Participants’ experiences were investigated through one-to-one semi-structured interviews. The interview guide was based on the characteristics of wound care described in the literature (4, 11, 12, 14). Practitioners of the multidisciplinary EB team in Groningen, 2 parents and a board member of Debra Netherlands (the patients’ association for EB) provided comments to further refine the interview guides. The interview guide for patients and parents included the same topics, but differed in perspective and partly in content. Sensitizing concepts were: (i) participant’s history, (ii) quality of life and daily functioning, (iii) coping strategies with regard to wound care, and (iv) recommendations of participants with regard to wound care.
This research was approved by the local ethics committee of the University Medical Center Groningen (UMCG) (registration number M16.189621). Patients and parents received a letter of invitation informing them about the purpose and content of the study and a consent form. All participants signed the written consent form and returned it to the UMCG in a pre-stamped envelope. Next, the principal investigator conducted the interviews at the participants’ homes, because, for some participants, the distance to the hospital was too far or physically too tiring for participants. The interviews took 45–90 min. All participants were interviewed without the presence of anyone else. Methodological objectivity was further enhanced by: (i) orally checking the findings with the respondent, (ii) member check by sending the transcribed interviews to participants; 2 participants responded by saying that it was confronting to read their own life story, but they did not want to change the content, (iii) peer debriefing of the principal investigator with the second and last author during data collection and analysis. The interviews were recorded on audio-tapes. The principal investigator stored these recordings in an online secure environment of the UMCG. Interviews took place from June 2016 until October 2016.
The qualitative data analysis formed a cyclic process, with the interim analyses modifying subsequent interviews. This procedure is well known as the constant comparative method (18). The interviews were transcribed verbatim in Microsoft Word. Next, the transcripts were analysed using Atlas-TI, a data processing program for qualitative analysis (19). Initially, open coding (20) was used: small text fragments were labelled. This label or code had a descriptive nature and closely followed the text. The next stage of analysis existed of joining the small text fragments by labelling higher level of abstraction. During the third stage of analysis, text fragments were further joined, categorized and described. Based on these categories of codes, the principal investigator and the third author independently created one thematic network for patients and one for parents, and reached consensus. The principal investigator and a research-assistant then independently coded all interviews.
The variety of subtypes of EB partly determined the differences in impact on daily life and the coping strategies of patients and parents. Despite these differences, a number of common themes emerged from the interviews.
Daily routine. Wound care was usually performed in the morning or in the evening in all patients and lasted from 30 min to 3 h a day. Due to the schedule in the morning or evening, it was not an obstacle for school or leisure time. Patients with milder forms of EB did not experience this as a major influence on their daily schedule.
”It influenced my daily routine not really. In the morning we looked at my skin and took care of it when needed, but it did not take much of my time.” Patient 1 (EBS)
However, patients with extensive wounds were forced to schedule more time for wound care. They indicated, for example, that wound care was programmed in the day, that they had to get up early to be able to perform wound care before school, or that wound care required a lot of patience, as the following quotes show.
”My daily routine was very much determined by it. The care was programmed completely. It was not possible to skip even one day.” Patient 2 (RDEB)
”When I went to school, I had to get up very early in the morning to do my bandages. I did it all by myself.” Patient 6 (JEB)
”If the wound care took a long time, you thought: ‘I want out, I want to go.’ However, you know you have to wait until it’s over.” Patient 3 (RDEB)
All parents mentioned the same recurring routine as patients with regard to wound care. Parents of patients with RDEB and 1 parent of a patient with DDEB experienced wound care as considerably influencing their daily schedule, which was partly related by having more children with EB and partly to the time required for care.
”It certainly influenced my daily routine. I always had to take into account that he had to be cared for, even in free time and on vacation. I packed suitcases full of bandages. No day passed without the wound care affecting it.” Parent 3 (RDEB)
All mothers reported that they were most involved in the wound care of their children, while most fathers also were involved, but much less. Four mothers decided not to work after having their child with EB and 1 mother did not work as a result of her own EB.
”I quit my job when he needed extra care. In this way, the necessity of wound care did influence this. I did not work anymore.” Parent 4 (JEB)
Parents of patients with moderate and more severe forms of EB indicated that wound care also affected their leisure time or social life.
Physical impact. The main physical impact of wound care on patients was pain. Patients with milder forms of EB indicated that they had little or limited pain from wound care, while patients with moderate and more severe forms indicated that they had a lot of pain from wound care. The removal of dressings was often the most painful because the bandage was mostly stuck to the wound.
”During wound care I was in pain. Removing bandages was the problem. Changing bandages hurt because the bandages had to be removed from the wounds. I wanted to postpone the removal of the bandages because I was afraid it was stuck. However, that was not possible, it had to happen.” Patient 7 (RDEB)
Despite the painful nature of the wound care, all patients indicated that they did not receive any pain medication. Itch sometimes occurred when the wounds were exposed to water or air, or when bandages were re-applied. Wound care was experienced as tiring by only 1 patient with a severe form of EB.
”If I had many wounds, especially on the feet, wound care was quite extensive and exhausting. After this, I sometimes did not feel well and I had to recover one to two hours.” Patient 3 (RDEB)
Two parents of children with moderate and severe forms of EB experienced wound care as tiring due to the preparation of wound care, performing the wound care itself and cleaning up afterwards. The other parents did not indicate that the wound care was physically tiring for them.
”I felt tired afterwards. Yes, I always had to recover downstairs. When he was gone, I always sat down for half an hour. A moment to recover.” Parent 6 (RDEB)
In addition, the recurring character made it more difficult for these parents to recover because they could not be relieved of this task for a longer period.
Emotional impact. Knowing that wound care was unavoidable and painful often caused emotions of anxiety for patients that seemed to take a dominant role compared with other negative emotions. Four patients mentioned that they experienced anticipatory anxiety; that is, fear of the pain that had still to come.
”I was so scared that I thought: “Oh the bandages will be removed.” and I already started crying because I knew it’s going to hurt.” Patient 6 (JEB)
Patients noticed the inescapabilty of wound care by considering it to be something that had to be done or indicated that they had never known differently from birth.
”I do not know anything else. I did not think when I woke up: Now I have to change my bandages again.” Patient 2 (RDEB)
Despite the feelings of anxiety, the wound care also provided some patients with positive emotions, such as experiencing cosiness or happiness.
”Yes, we were just happy during wound care, it was not a negative thing. And my sister was often there too. It was no annoying moment.” Patient 5 (DDEB)
Parents showed a wide range of negative emotions related to wound care, such as powerlessness, sadness, and suffering.
”Doing bandages, I found it terrible. The powerlessness that you feel is horrible.” Parent 5 (DDEB)
”You became very sad. You did not want it, but it had to happen. And when your child could not see it, you cried.” Parent 1 (DDEB)
In particular, having to hurt their own child caused distress in all parents. The negative emotions dominated when parents talked about wound care during the interviews. This was noticeable because they cried or indicated that it was difficult to talk about it. Despite this, some parents indicated that wound care was not only misery, but also could provide moments of happiness.
”Despite the painful aspects of wound care, it really was not constant misery. We really liked to sing together.” Parent 3 (RDEB)
All participants, regardless of type of EB, used several similar coping strategies, with parents being more aware of using coping strategies than patients.
Transferring care. The transfer of care was primarily a strategy of parents to cope with the impact of wound care. However, the patients with the more severe forms of EB had relevant experience with, and a clear opinion about others who had performed their wound care. For example, one patient preferred his mother performing wound care because he felt that only she had the right skills to take care of his wounds quickly and carefully. Another patient described how he got used to home nursing since puberty and what advantage this brought him in the end.
”In the beginning I did not like home nurses because I did not want any strangers to [touch] my body. Nevertheless, in the end I was glad that the care had been separated from my mother. This separation has strengthened my independence.” Patient 3 (RDEB)
Parents described that they had made a well-considered choice to transfer or not to transfer the care by weighing up the advantages and disadvantages. Because this wound care required so many skills, it was not easy for most of them to trust other caregivers. Most parents believed they were the people who were best able to do the wound care of their child and some felt guilty to leave the care to others.
”You know exactly your child and you also think that you can do it best. And that is true. That just makes it difficult to transfer care. They are so vulnerable.” Parent 6 (RDEB)
”They hurt my child, that’s how it felt. Even if my husband did it. And if I said on a Saturday: “You do it today. I’m leaving”, I felt a bit guilty about that.” Parent 5 (DDEB)
Two parents decided to transfer the care because they felt the degree to which their child needed care left them no other choice. This decision enabled them to fulfil other aspects of being a parent or to take physically more rest to be better able to cope with the situation.
”In the end, we called for help. A young student, a fantastic girl, came to help me four times a week. In the morning, she prepared everything and afterwards we did the wound care together. I also had to go out for my child very often in the night. Because of her help, I could have some more rest in the morning.” Parent 6 (RDEB)
Regulation of emotions. Several patients explained how emotions, such as anxiety, determined their thoughts or behaviours, but most patients had not been aware of deliberately regulating their emotions or could not remember it. Patients described how their parents often understood and tolerated their expressions of emotions, e.g. crying, caused by wound care.
”I sometimes cried during the dressing changes. I remember that my mother did not say anything about it. She did not say: Keep your mouth shut. She just said: We have to do this.” Patient 6 (JEB)
On the contrary, all parents emphasized the importance of hiding their negative emotions, for example by turning off their emotions, feeling emotions but not showing them, or focusing on something else that suppressed emotions. According to parents these strategies helped both their child and themselves endure wound care.
”I really did not know if my child was aware of my emotions during wound care. I deliberately hid my emotions. No, I did not show them. I would never do that. That was impossible. Then we would all go down underneath.” Parent 5 (DDEB)
One parent mentioned that she focused on positive feelings by making the atmosphere during the wound care as cheerful as possible.
”Those wound care sessions are already serious enough. I would try to make it as happy and as light as possible. Also the decoration of the bathroom. Keep it a little cozy, not all white, but colorful curtain, nice colored bath towels. It may sound silly but it helps.” Parent 3 (RDEB)
Supporting each other. All participants showed that they experienced distraction, rituals, encouragement and collaboration as helpful to support each other.
Patients did not often mention that they themselves sought distraction, but described how they got used to the help of their parents.
”I think my mother and my grandparents were excellent in providing distraction. They made a game of the wound care, but I did not distract myself.” Patient 7 (RDEB)
Parents offered a wide variety of distractions to their children. According to these parents, the provision of distraction was an effective way to make wound care more bearable for both of them.
”We always had a cassette or radio program that we both listened to. This was meant to distract us both.” Parent 3 (RDEB)
Several patients described that they were used to the rituals surrounding wound care and therefore exactly knew what was coming, but mostly their parents initiated these rituals. These rituals often related to the time when wound care had to be done, the room in which it happened, the sequence of actions and the way distraction was provided. The rituals were often taken over by the children as the following quote shows.
”Every evening I asked my mother to put the itch away. And she always said: “Then we do [put] all the itch in a jar.” We did that. And that also helped. If you believe in it, it will help.” Patient 5 (DDEB)
Parents found it important to apply certain rituals, even if there was not always a special medical need for it. They experienced these rituals as helpful to start the wound care and to have control over the situation during wound care.
”We always had fixed times for it. Always before diner. Then we did the wound care followed by dinner. During dinner he could forget the trouble a little before he went to sleep.” Parent 2 (EBS)
Patients expressed that supportive comments of their parents were very helpful to them, but none of them mentioned they had supported their parents themselves.
”She encouraged me with words. She said: “You know that it hurts when air comes to the wound, but about five minutes it’s over again”. This helped me to endure the pain.” Patient 1 (EBS)
Parents explained that they encouraged their children by giving compliments, phasing the wound care, promising some reward in the future, or comforting them with physical proximity. It became clear that some parents not only gave encouragement but also received encouragement from their children.
”What I sometimes notice when I’m worried – and I do of course – then she says: Mom, you do not have to. From her youth, she always has had that. Like: You do not have to worry. In fact, she comforts me in a little bit like: “If I do not find it a problem, you do not have to find a problem either.” She really helps me in such a way!” Parent 6 (RDEB)
Patients and parents also stressed the importance of collaboration, but the extent to which parents and children worked together differed greatly between participants. Not only did parents see themselves as an expert, some patients too considered themselves as important participants in changing bandages.
”When changing bandages, my mother did not do it alone. We did it together. Then my mother did the knee and I the other knee. So we did it together. It was ... I think it is good to do the changing of bandages together.” Patient 2 (RDEB)
Parents were also convinced that good cooperation during wound care, in which the child had his or her own role, could help to reduce the pain.
”When she got older, I allowed my child to remove the bandages by herself. She felt the pain so that she could better determine how and at what pace the bandage went off.” Parent 1 (DDEB)
This study highlights the fact that wound care has a considerable impact on the daily routine of patients with moderate and severe forms of EB and parents of patients with moderate and severe forms of EB. While for patients with mild forms of EB, pain due to wound care was limited, patients with severe or moderate forms of EB experienced a lot of pain. Despite the differences in pain experience, it is striking that anxiety, especially, occurred in most patients irrespective of the type of EB. In all parents, also regardless of the type of EB, a much broader spectrum of negative emotions was associated with wound care. Besides this, it is remarkable that several participants also experienced positive feelings with regard to wound care. A number of previous studies also support the fact that wound care is a burden both for children with EB and for parents (4, 11, 14, 15, 21). However, in the existing literature, it has hardly been discussed which positive and negative emotions occur with respect to wound care in patients with EB, on the one hand, and their parents, on the other hand.
The coping strategies transferring care, distraction and the involvement of children in wound care have also been mentioned as helpful in previous studies (15, 22). It is noteworthy that the majority of parents find it difficult to transfer care, even if this seems necessary. The deliberate hiding of negative emotions by parents and the use of rituals and encouragement, on the other hand, have hardly been discussed in the existing literature as helpful strategies for wound care.
The findings of this study further indicate that wound care is a dyadic rather than an individual task. Dyadic coping can be defined as the attempts of one member of the dyad to help reduce the stress experienced by the other member of the dyad, and the combined efforts to cope with stress in the relationship (23). In the current literature little attention is paid to dyadic coping in parent–child dyads. The results of this study draws attention to the fact that children and parents in the case of wound care may also use dyadic strategies. Although parents seem to have a leading role in implementing these strategies, the coping strategies of children also appear to be helpful for parents.
The results of this study suggest that the burden of wound care should be examined more broadly and also underlines the need for a more thorough investigation into the helpfulness of the described coping strategies transferring care, regulation of emotions and helping each other.
This is a small study with a wide variety of types with EB, which makes it difficult to make statements that relate to the larger EB population. The retrospective nature of the study may have resulted in some recall bias, such as the fact that patients are further removed from their childhood experiences and their wound care is different from the current children with EB. These differences in wound care may also have influenced the perception and coping strategies of children and parents. It is also an incompleteness that the experiences of fathers with regard to wound care could not be taken into account. Although the current study was explorative, the qualitative approach made it possible to gain an in-depth understanding of the impact of wound care on children and parents.
Given that wound care in children and parents is accompanied by anxiety and various negative emotions, it is desirable that attention be paid to the psychological support of children and parents in wound care. In addition, it is recommended that parents and children are supported by healthcare professionals, such as doctors and psychologists, when discussing coping strategies to alleviate wound care.
This study was funded by the foundations Eleven Flowers, Debra Netherlands and Vlinderkind.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize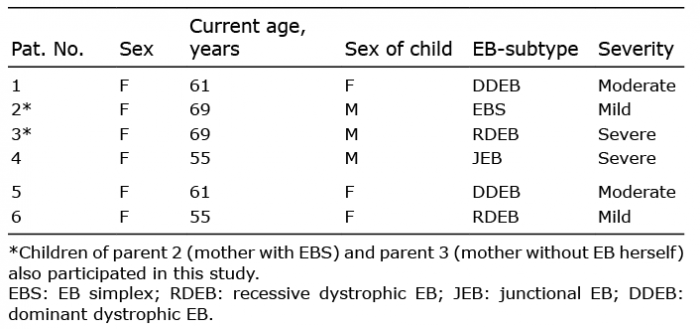 Click to show fullsize
Click to show fullsize