


1Department of Dermatology, South Infirmary Victoria University Hospital, Old Blackrock Road, 2School of Medicine, University College, 3Department of Histopathology, Cork University Hospital, and 4Department of Medical Oncology, Bon Secours Hospital, Cork, Ireland. E-mail: catherine_quinlan2000@yahoo.com
Accepted Mar 21, 2019; E-published Mar 21, 2019
The incidence of melanoma is increasing and is projected to continue to do so (1). In Ireland, 20 people per 100,000 of the population develop invasive melanoma every year and 159 die from it (2).
Despite improvements in early detection (3), the number of deep poor prognosis melanomas remains high (4). Older age, male sex (5), living alone and lower education level (6), have been identified as factors associated with thick melanomas. There has been much focus on the role of general practitioners in melanoma screening strategies. However, the role of non-dermatology hospital services in detecting melanoma has been poorly explored. The aim of this project was to determine if an opportunity exists for detection of melanoma in secondary care facilities.
Ethical approval was obtained from the Cork Research Ethics Committee.
A retrospective case review was conducted at 5 hospitals across the region. The pathology database at Cork University Hospital (CUH), which processes histology samples from all 5 hospitals, was searched. The inclusion criteria were patients with a Cork/Kerry address, diagnosed with primary cutaneous melanoma ≥ 1 mm Breslow depth, between January 2013 and December 2014. Each clinical site was visited and hospital utilization data for each patient at each of the 5 clinical sites was collected.
There were 106 patients included in the study; 51 men (48%) and 55 women (52%). The mean age was 63 years at time of diagnosis.
The median Breslow depth was 2.3 mm with a range from 1.0 mm to 41 mm. Twenty-three (22%) were > 5 mm Breslow depth at time of diagnosis. Sixty-seven percent (n = 71) of patients were seen in secondary care in the 5 years prior to their diagnosis of melanoma. There were a total of 901 healthcare interactions. The majority of these interactions were in the outpatient setting (57.5%). However, almost one third (31%) had an inpatient admission in the 5 years prior to diagnosis with a mean length of stay of 6 days.
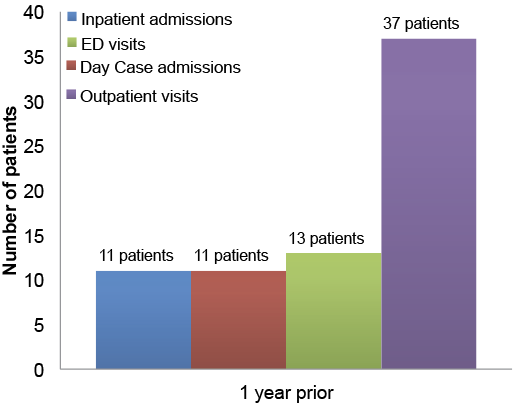
Forty-five patients (42.5%) were seen in secondary care in the year prior to diagnosis. Results are illustrated in Fig. 1. There were a total of 214 healthcare interactions. Thirty-five percent (n = 37) were seen in outpatient clinics and 10.4% (n = 11) had an inpatient admission. The median Breslow depth in this group was 2.5 mm. Forty percent (n = 18) of these patients had melanomas located on the head and neck.
Head and neck was the most common anatomical location (n =32) followed by lower limb (n =30), upper limb (n =22) and trunk (n =22). Of the 32 patients with a head and neck melanoma, 18 (56%) had been seen in secondary care in the year prior to their diagnosis.
In terms of histological subtype, the majority were superficial spreading type (n =48) followed by nodular (n =30), lentigo maligna (n =18), other (n =6) and acral lentiginous (n =4).
The specialties with the most patient interactions in the year prior to diagnosis were ophthalmology, orthopaedics, and emergency medicine.
Fig. 1. Secondary care interactions in the year prior to melanoma diagnosis. (ED=Emergency Department).
This study has identified that patients with thick melanomas are being seen in hospital in the year prior to their diagnosis. Research on the use of health services in the year prior to diagnosis of melanoma have found similar results (7, 8), but these studies did not isolate for interactions in secondary care. Outpatient visits contributed to the majority of healthcare interactions in our study. While there may be limited opportunity for full skin examination in an outpatient setting, studies have shown that even opportunistic partial skin examinations have been effective in detecting melanoma at a thinner stage (9).
The majority of melanomas in our study were located on the head and neck region and would therefore have been readily identifiable without the need for full skin examination.
While it is impossible to say how long a melanoma may have been present prior to diagnosis, the majority of melanomas in this study were superficial spreading subtype and a significant number were lentigo maligna subtype, suggesting that these lesions had likely been present for a significant period of time prior to diagnosis.
Significant opportunity exists to improve early detection of melanoma by healthcare providers in secondary care. Strategies to promote this would include greater emphasis on melanoma detection in medical student curriculum, and continuous professional development modules on opportunistic skin cancer detection for healthcare providers. Dermatologists should work with these groups to promote further education and awareness.
A larger study is needed to explore this issue further in other countries and populations.
The authors have no conflicts of interest to declare


 Click to show fullsize
Click to show fullsize