


1Oregon Health and Science University, Portland, OR, 2University of Miami, Miller School of Medicine, Miami, FL, 3Pfizer Inc, Groton, CT, USA, 4University Hospital Münster, 5Center for Chronic Pruritus, University Hospital Münster, Münster, Germany, 6University of California, 7Rady Children’s Hospital-San Diego, San Diego, CA, 8Pfizer Inc, Collegeville, PA, and 9Pfizer Inc, New York, NY, USA (at the time of the analysis)
Crisaborole ointment is a nonsteroidal phosphodiesterase 4 inhibitor for the treatment of mild to moderate atopic dermatitis. Using pooled data from two phase 3 studies (NCT02118766/NCT02118792), mediation modeling determined the interrelationship among pruritus, quality of life (QoL), and treatment. Patients aged ≥ 2 years received crisaborole ointment, 2%, or vehicle twice daily for 28 days. QoL measures were Dermatology Life Quality Index (DLQI) (≥ 16 years) and Children’s Dermatology Life Quality Index (CDLQI) (2–15 years). Pruritus was assessed by the Severity of Pruritus Scale (4-point scale from 0 to 3). The indirect effect of crisaborole on QoL mediated through its effect on pruritus was 51% (DLQI model, p < 0.05) and 72% (CDLQI model, p < 0.05). Direct effect (other effects) on QoL was 49% (DLQI model, p < 0.05) and 28% (CDLQI model, p > 0.05). Mediation modeling shows that crisaborole affects QoL mostly indirectly through pruritus severity reduction.
Key words: crisaborole; atopic dermatitis; quality of life; mediation; pruritus.
Accepted Mar 21, 2019; E-published Mar 21, 2019
Acta Derm Venereol
Corr: Eric L. Simpson, MD, Oregon Health and Science University, 3303 SW Bond Ave, Portland, OR 97225, USA. E-mail: simpsone@ohsu.edu
Atopic dermatitis, a skin disease characterized by inflammation and itching, has a significant impact on a patient’s quality of life. Mediation modeling can be used to find if a causal factor influences an outcome factor through a third factor, the mediator. The mediation analysis presented here shows that quality of life in patients with atopic dermatitis is mostly influenced by the effect of the treatment on itching.
Atopic dermatitis (AD) is a chronic inflammatory skin disease characterized by intensely pruritic eczematous lesions (1, 2). Pruritus is the predominant symptom of AD; approximately 91% of patients with AD report daily pruritus (3). The precise mechanism of AD-associated pruritus is complex and continues to be investigated; however, it is thought to be caused by various inflammatory and noninflammatory stimuli (4). AD-associated pruritus has a significant impact on quality of life (QoL) in children and adults (5), and, as a result, a central goal of treatment is rapid relief of pruritus flares and long-term symptom control (4).
Until recently, initial pharmaceutical treatment of AD involved topical corticosteroids (TCSs) or topical calcineurin inhibitors (TCIs), but there are potential limitations to their use (6–8). TCSs are the mainstay of AD treatment and are effective in treating active inflammatory disease (6–8). However, their broad mechanism of action can lead to adverse effects, such as skin atrophy, particularly with more potent agents. Such adverse effects have resulted in “steroid phobia” or a hesitancy of patients to use these agents (9–11). TCIs reduce body surface area involvement and signs and symptoms of AD; however, efficacy is comparable with that of low- or mid-potency TCSs (6–8). The most common adverse event with TCIs is burning and stinging, which can preclude their use in many patients, especially in children (12). As a result, there is a need for new, effective, nonsteroidal treatments that address inflammation and pruritus.
Crisaborole ointment is a nonsteroidal phosphodiesterase 4 (PDE4) inhibitor for the treatment of mild to moderate AD. Crisaborole, a novel boron-containing molecule approved to treat mild to moderate AD in patients aged ≥ 2 years, reduces pro-inflammatory cytokines via a unique mechanism of action through inhibition of PDE4 (13–15). In 2 identically designed phase 3 clinical studies (AD-301: NCT02118766; AD-302: NCT02118792), crisaborole ointment, 2%, improved global disease severity and all measured signs and symptoms of AD in significantly more patients compared with vehicle; application site pain was the most common treatment-related adverse event (13).
In prespecified and post hoc analyses, crisaborole ointment also reduced the severity of pruritus in significantly more patients compared with vehicle ointment at day 29 and at week 4 of the studies (p = 0.005 and p < 0.001, respectively) (13, 16, 17). A qualitative and psychometric analysis of the Severity of Pruritus Scale (SPS), a 4-point rating scale ranging from 0 (“no itching”) to 3 (“bothersome itching/scratching which is disturbing sleep”), used in the phase 3 studies was recently completed and supported the validity of the measure for use in AD (18). Greater mean improvement in QoL was also observed with crisaborole compared with vehicle at day 29 (19).
Mediation modeling has been used in inflammatory diseases and other diseases to establish the contributions of direct and indirect effects of a treatment on an outcome (20–23). A mediation model hypothesizes that the predictor variable, such as a treatment, not only affects the outcome variable (i.e. QoL) directly but also affects the mediator variable (i.e. pruritus), which in turn also affects the outcome variable. The mediator variable can help clarify the nature of the relationship between predictor and outcome variables (22). Because of the potential link between pruritus and QoL, and the significance of pruritus as a cardinal symptom of AD, the purpose of this analysis was to determine, through mediation modeling, the interrelationship among subject-reported pruritus, QoL, and treatment using pooled data from the AD-301 and AD-302 studies.
The data used in the mediation model came from the 2 large phase 3 studies: AD-301 and AD-302 (13). In brief, AD-301 and AD-302 were identically designed, multicenter, randomized, double-blind, phase 3 studies conducted to compare crisaborole with vehicle in the treatment of mild-to-moderate AD. Patients aged ≥ 2 years with mild-to-moderate AD per the Investigator’s Static Global Assessment (ISGA) were randomly assigned to receive either crisaborole, 2%, twice daily or vehicle for 28 days. Both studies were conducted in accordance with Good Clinical Practice Guidelines and local regulatory requirements. The institutional review boards of participating centers approved the study protocols, and all participants provided informed consent.
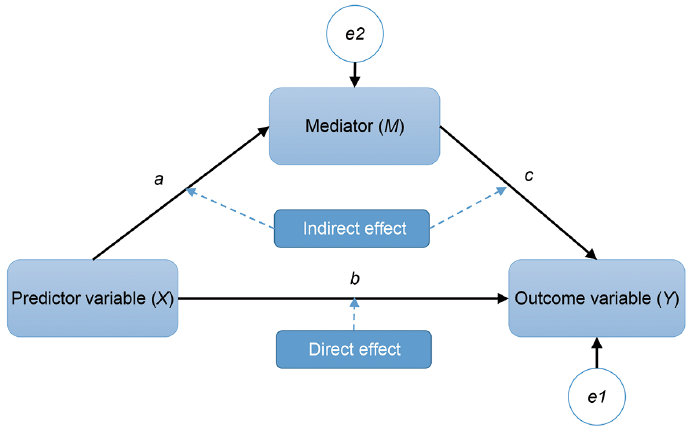
Although research is more likely to look for a correlation between a predictor variable (X) and an outcome variable (Y), mediation in its simplest form is represented by a third variable (M, the mediator), where the predictor X influences the mediator M, which, in turn, influences the outcome Y (i.e. X affects M and then M affects Y). Also included are e1 and e2, which are error terms for Y and M, respectively (Fig. 1) (22). In the current mediation model, the predictor variable was treatment (crisaborole vs vehicle), with severity of pruritus as the mediator variable and QoL as the outcome variable.
Fig. 1. Basic mediation model. In mediation modeling, a represents the effect of the predictor (independent) variable X on the mediator variable M; b represents the direct effect of the predictor variable X on the outcome variable Y; c represents the effect of the mediator variable M on the outcome variable Y; e1 and e2 are the error terms for Y and M, respectively.
Quality of life was measured using the Dermatology Life Quality Index (DLQI) in patients aged ≥ 16 years and the Children’s Dermatology Life Quality Index (CDLQI) in patients aged 2–15 years (Table I) (24, 25). DLQI and CDLQI scores from day 29 were used. Each QOL measure was used in its own mediation model.
Table I. Quality of life (QoL) assessment scales and subscales: Dermatology Life Quality Index (DLQI) and Children’s Dermatology Life Quality Index (CDLQI)
Severity of pruritus was assessed using the SPS (Table II), which was administered via electronic diary twice a day, morning and evening, with a recall period of 24 h (13). For consistency with the 1-week recall period of the DLQI and CDLQI, the SPS score used in the analysis consisted of mean SPS scores over week 4 (days 23–29) for every patient. All available data were used, and no imputations of missing data were performed. Vehicle data were included as part of the analysis, along with crisaborole, to provide a measure of the effect of crisaborole beyond that of the vehicle. p-values, which apply to all patients within the model, represent whether the percentage of the total effect that is direct or indirect is statistically different from 0%.
Table II. Severity of Pruritus Scale
In total, 1,522 patients were included in both studies: 1,016 were randomly assigned to receive crisaborole and 506 were randomly assigned to receive vehicle. There were no significant differences across treatment groups or across studies in baseline demographics and disease severity (Table III). The mean age between both groups was approximately 12.2 years. Most patients (approximately 86%) were aged 2–17 years. Approximately 55.6% of patients were female. In both groups, distribution by race was approximately 61% white, 28% black, 5% Asian, and 6% other. Most patients (approximately 61%) had moderate AD per ISGA and mean treatable percentage of affected body surface area (%BSA) was approximately 18% (range, 5% to 95%). Among those with available baseline pruritus measurement, approximately 26% had mild, 37% had moderate, and 32% had severe pruritus. Based on previously established severity bands for DLQI and CDLQI (26, 27), the mean baseline DLQI and CDLQI scores indicated that there was, on average, a “moderate effect” of AD on QoL at baseline. For the mediation model, 266 patients were included in the DLQI analysis and 1,112 patients were included in the CDLQI analysis.
Table III. Baseline demographics and disease characteristics
For both adults and children, the indirect effect through itch had a sizable influence and, at the same time, was more prominent for children than for adults. The indirect effect for adults was about half (51.4%) the total effect of treatment on DLQI (p = 0.0272), whereas the indirect effect for children was about three-fourths (72.4%) the total effect of treatment on CDLQI (p < 0.0001).
The direct effect, which represented all other effects of crisaborole on QoL other than pruritus, was less than half (49% [DLQI-based model; p = 0.0365] and 28% [CDLQI-based model; p = 0.0701]) of the total, or overall, effect of the active treatment on QoL (Figs 2 and 3).
Fig. 2. Dermatology Life Quality Index (DLQI)-based mediation model. SPS: Severity of Pruritus Scale.
Fig. 3. Children’s Dermatology Life Quality Index (CDLQI)-based mediation model. SPS: Severity of Pruritus Scale.
Quality of life is one of the most important aspects of AD that patients use to judge treatment response (28). From a broader perspective, chronic pruritus of any cause has been associated with impaired QoL and emotional well-being in population studies (29). In AD, pruritus can disrupt sleep, particularly in children, resulting in impaired functioning and worsening QoL (30, 31). In particular, pruritus has resulted in decreased motionless time asleep, decreased sleep duration, and decreased sleep quality (30), which in turn results in impaired functioning, increased irritability, and psychological problems (30). Pruritus also contributes to depression, agitation, changes in eating habits, and difficulty concentrating (30).
The current findings in the presented mediation model indicate that crisaborole affects QoL mostly indirectly through reduction in the severity of pruritus (i.e. intensity, scratching, and sleep dimensions) as opposed to directly through other effects of treatment, such as reduction in the inflammation and clinical signs of AD. Interestingly, the indirect path in the CDLQI-based model was more pronounced, possibly because of differences in item composition of the 2 QoL questionnaires (Table I). For instance, the CDLQI includes sleep as a component (25), which is highly affected by pruritus (30), whereas the DLQI does not.
Mediation models are helpful in that they are used to identify and explain the mechanism that underlies observed relationships between predictors and outcomes by including a third mediator variable – in essence, by narrowing the causation of an outcome (22, 32–34). Modern approaches to mediation have been inspired by the work of Wright, in the year 1921 (35), who developed the path analysis method, which started to become popular in psychological studies in 1986 (36).
Conventional logistic and linear regression analyses are suited to examine the effect or association of a given predictor on an outcome (possibly controlling for other predictors or covariates). A single linear regression model is equipped, for example, to study the effect of treatment, along with possibly baseline demographic and clinical variables, on DLQI. But such a model is not suited or intended to assess the interrelationship of 3 or more variables simultaneously (e.g., treatment, DLQI, and itch) because it is restricted to quantifying the relationship between only one pair of variables at a time (e.g., treatment-DLQI as one pair and itch-DLQI as another pair); it does not account for the effect of (say) treatment on itch.
In addition, for a postbaseline mediator (such as postbaseline itch), the single regression model becomes misspecified (e.g., as an explanatory variable, treatment, affects another explanatory variable, postbaseline itch, as well as the outcome such as DLQI). To address these limitations, 2 regression models need to be fit simultaneously, resulting in a mediation model that is suited to assessing the interrelationship of variables simultaneously to quantify the direct effect of a predictor (e.g., treatment) on outcome (e.g., DLQI) and the indirect effect of the same predictor on the same outcome through the mediator (e.g., itch).
Our research question is not concerned with the effect of treatment on DLQI per se (or the effect of itch on DLQI), which is what a single linear regression model would produce; our research does not center on how much treatment improves QoL (as measured by DLQI). Instead, mediation modeling was used to understand what part of the treatment effect on QoL is mediated via improvement in itch and thus to understand the mechanism of action of crisaborole as it relates to itch and QoL.
Therefore, a mediation model resolves the issue of model misspecification and partitions the overall treatment effect on DLQI into a proportion of which is direct and the remaining proportion of which is indirect through itch. The effect of the treatment on itch can be correctly accounted for by adding an additional equation and solving 2 equations simultaneously. Moreover, a mediation model is flexible enough to have multiple mediators (not just one) to target the need of a research question requiring more than 3 variables based on a conceptual framework grounded in theory or a clinical rationale.
As has been previously reported, crisaborole reduces disease severity (as measured by global assessment of clinical signs and by affected %BSA) and pruritus severity and improves QoL (13). Through this mediation analysis, it can be seen that the improvements in QoL may be primarily a result of the effect of crisaborole on pruritus.
Data from few studies have been published to attempt to identify which treatment effect is most relevant to a patient’s QoL. A study conducted to explore chronic pruritus conditions did suggest a greater correlation between pruritus severity and QoL, as opposed to an association between age, sex, or origin of pruritus on QoL (37). The results from our mediation analysis add to the evidence that pruritus is one of the most important symptoms of AD, and improvement in this cardinal symptom led to relevant QoL improvement, more so than improvement in the clinical signs of the disease alone.
Limitations of this analysis include the post hoc nature of the mediation model, which was conducted using data from 2 already completed clinical studies. Additional studies are necessary to substantiate these results. In addition, the study population consisted of those with mild-to-moderate AD based on the ISGA; the majority had moderate AD at baseline, although 32% had severe pruritus at baseline based on the SPS. It is unclear how inclusion of patients with severe AD would affect the results observed. Our mediation model also assumes no unmeasured confounding between predictor and outcome, predictor and mediator, and mediator and outcome. The first 2 of these potential confounder pairs are addressed by the randomized study design, and we have no evidence to show that the third confounder pair is violated. The conclusions drawn from this analysis are based on a postulated relationship; the mediation model is plausible and clinically rational because associations between pruritus and QoL have been described previously (4, 38, 39). Another limitation is that our model does not test other specific potential mediators that could possibly help refine the model, such as sleep or affected %BSA. Regarding the QoL scales used, CDLQI has been validated for use in patients aged 4–16 years, and the current analysis is based on a population that includes patients as young as 2 years. However, another analysis of the subgroup of patients aged 4–15 years from the phase 3 crisaborole studies demonstrated that the change in CDLQI was comparable to that seen in the cohort of patients aged 2–15 years (40), and the CDLQI had been used to assess 238 patients who were aged 2–3 years. Finally, although not necessarily a limitation of the analysis itself, the SPS has been primarily used in clinical trials and is largely unknown by most clinicians, but it was recently validated (18).
As shown in this mediation model, crisaborole improves QoL by reducing the severity of pruritus. Future studies could test other measurable mediators to further refine the model.
Medical writing support under the guidance of the authors was provided by Robert J. Schoen, PharmD, and Corey Mandel, PhD, at ApotheCom, San Francisco, CA, USA, and was funded by Pfizer Inc., New York, NY, USA, in accordance with Good Publication Practice (GPP3) guidelines (Ann Intern Med 2015;163:461–4).
This study was supported by Pfizer Inc.
Conflicts of interest: ELS is a consultant for Eli Lilly, Galderma, Celgene, Leo Pharma, GlaxoSmithKline, AbbVie, Pfizer, Regeneron, and Menlo Therapeutics and a principal investigator for Leo Pharma, AbbVie, GlaxoSmithKline, Regeneron, Novartis, Tioga Pharmaceuticals, and Vanda Pharmaceuticals. GY is a consultant for OPKO Health, Castle Creek Pharmaceuticals; a member of scientific advisory boards for Menlo Therapeutics, Trevi Therapeutics, Sanofi, Galderma, Eli Lilly, Novartis, and Sienna Biopharmaceuticals; and a principal investigator for Pfizer, Allergan, the Leo Foundation, Sun Pharmaceutical Industries, Vanda Pharmaceuticals, and Menlo Therapeutics. TL is an investigator for AbbVie, Celgene, Eli Lilly, Novartis, Pfizer, Sandoz, Menlo Therapeutics, and Leo Pharma; is a member of scientific advisory boards for AbbVie, Argenx, Celgene, Ceres Pharma, Galderma, Eli Lilly, Jansen-Cilag, La Roche-Posay, Mylan/Meda AB, Novartis, Pfizer, Sandoz, Sanofi-Aventis, Symrise, Menlo Therapeutics, Leo Pharma, Pierre Fabre, and Piqur Therapeutics; and has received funding from AbbVie, Celgene, Jansen-Cilag, Mylan/Meda AB, Merck Sharp & Dohme, Novartis, Pfizer, and Wolff Laboratories. SS is a principal investigator for Dermasence, Menlo Therapeutics, Trevi Therapeutics, Galderma, and Novartis; a member of scientific advisory boards for Beiersdorf, Celgene, Galderma, Kiniksa Pharmaceuticals, Menlo Therapeutics, NeRRe Therapeutics, Sienna Biopharmaceuticals, and Trevi Therapeutics; and a consultant for Novartis. WLT is a principal investigator for Pfizer, Regeneron, Medimetriks Pharmaceuticals, Incyte Corporation, Celgene, Janssen Pharmaceuticals, Promius Pharma, and Dermira. RAG, JCC, HT, WCP, and AB are employees and stockholders of Pfizer Inc. AMT is a former employee and stockholder of Pfizer Inc.


 Click to show fullsize
Click to show fullsize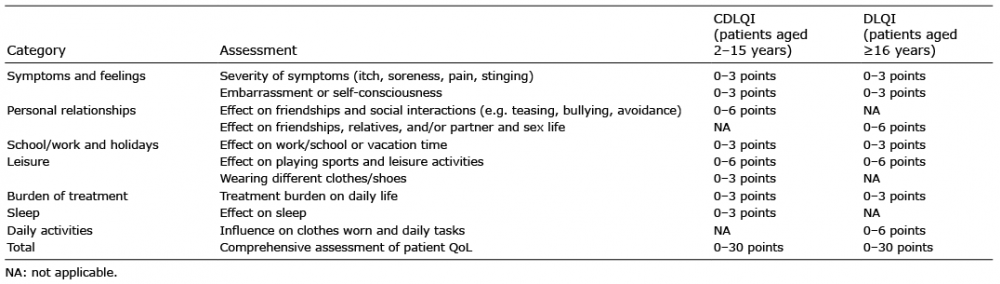 Click to show fullsize
Click to show fullsize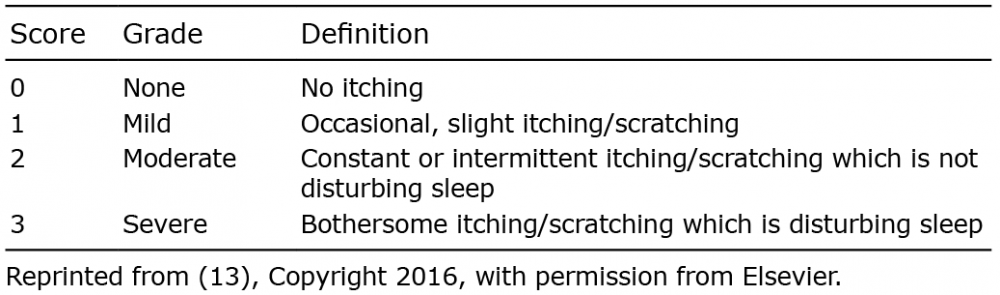 Click to show fullsize
Click to show fullsize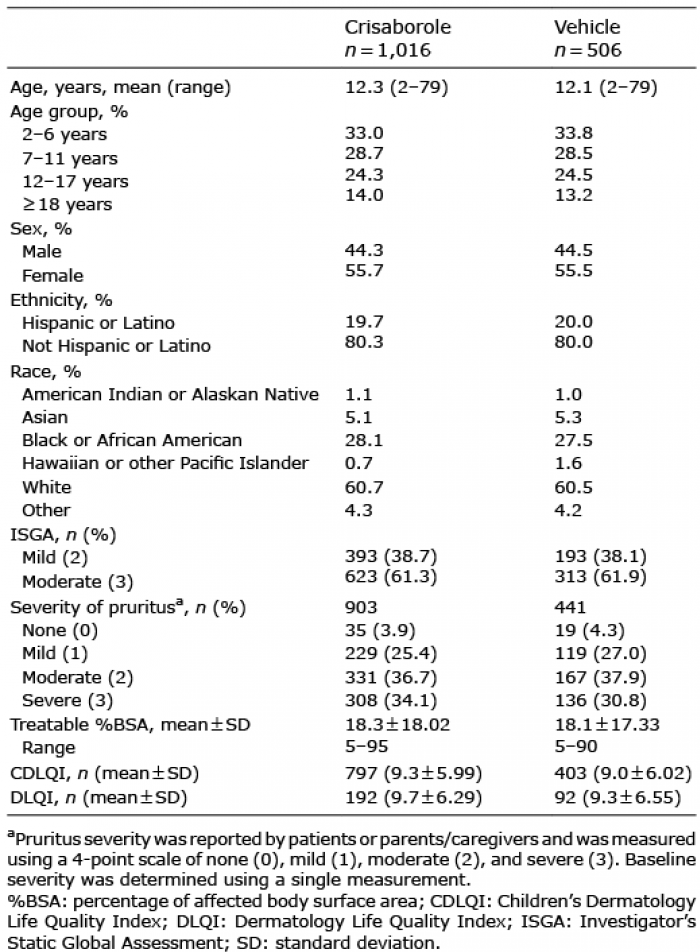 Click to show fullsize
Click to show fullsize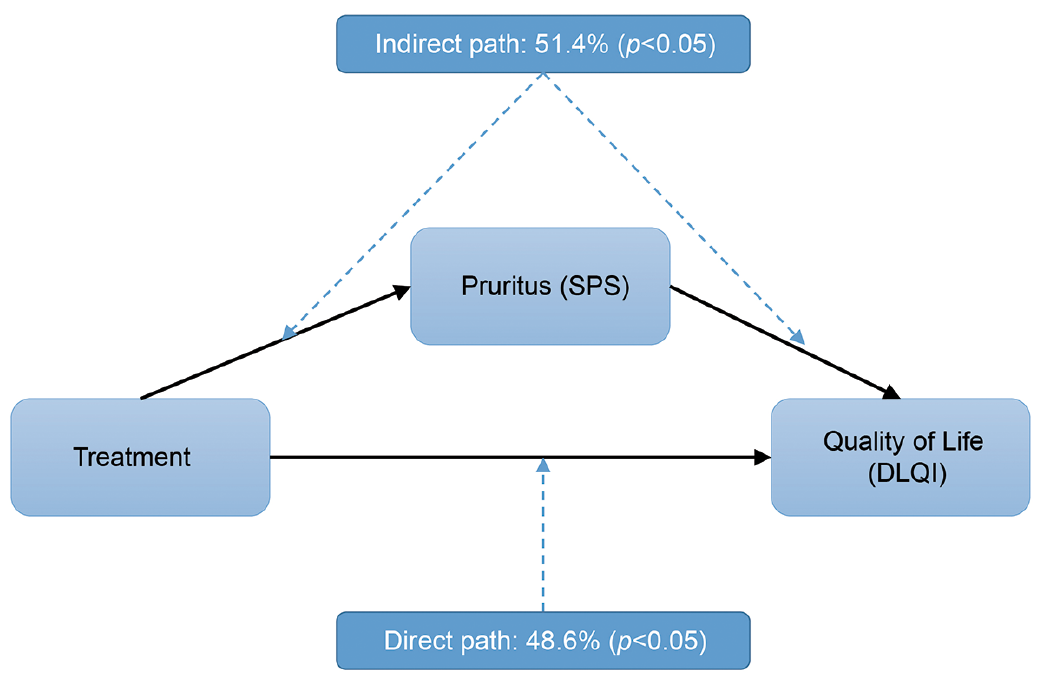 Click to show fullsize
Click to show fullsize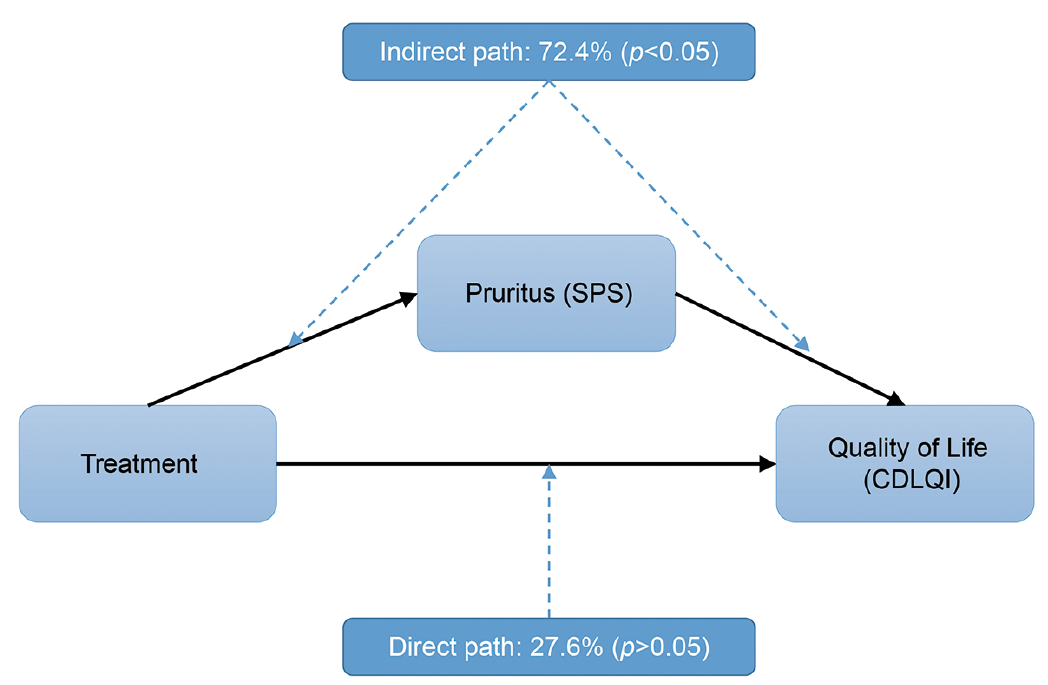 Click to show fullsize
Click to show fullsize