


Department of Dermatology, Teikyo University School of Medicine, 2-11-1 Kaga, Itabashi-ku, Tokyo 173-8605, Japan. *E-mail: mkamata-tky@umin.ac.jp
Accepted Apr 2, 2019; E-published Apr 2, 2019
Atopic dermatitis (AD) is a chronic inflammatory skin disease associated with pruritus and characterized by recurrent exacerbations and remissions. AD has an enormous impact on patients’ quality of life. Dupilumab, an anti-interleukin (IL)-4 receptor α antibody, recently became available for AD treatment, and is highly effective. Alopecia areata (AA) is often recurrent and refractory in some cases, but effective treatment for AA is currently limited. Here, we report a patient with severe AD, receiving dupilumab, who showed improvement of AA.
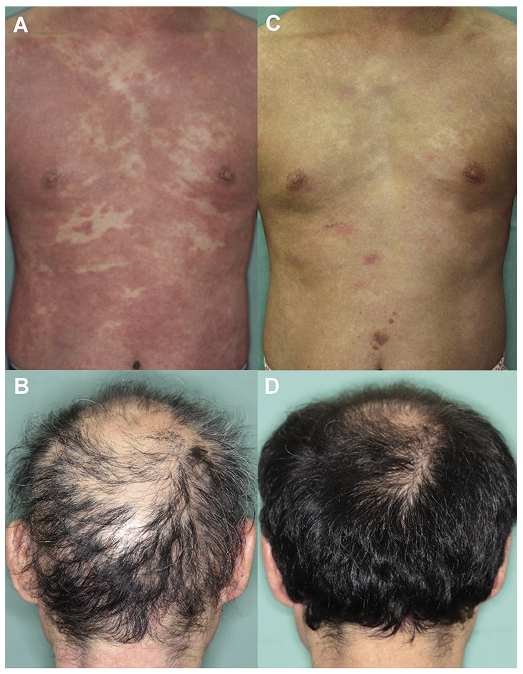
A 44-year-old man, with a history of AD since childhood, complained of focal patches of hair loss and was diagnosed clinically with AA at a local hospital 8 years prior. He had been treated for AA with a topical corticosteroid and 5 mg/day of oral prednisolone for the past 3 years, which did not result in any significant hair regrowth. As for AD, although he had been treated with topical corticosteroids, it had been difficult to control. He was referred to our department for further treatment. At his referral, he presented with erythema and lichenification, with slight scales, over the entire body (Fig. 1A), and spotty baldness on his head, which in some parts coalesced into larger areas (Fig. 1B). His eczema area and severity index (EASI) was 46.7. Body surface area (BSA) was 90%. The visual analogue scale (VAS) of pruritus was 70/100 mm. Severity of alopecia tool (SALT) score was 61.6. Laboratory tests revealed elevated serum levels of IgE (44,300 IU/ml; normal 0–99), thymus and activation-regulated chemokine (TARC; 23,339 pg/ml), lactate dehydrogenase (LDH) (441 U/l; 124–222) and normal thyroid function. Two months after his first visit to our hospital, he received 600 mg of dupilumab subcutaneously for severe AD, then 300 mg every two weeks, in addition to the treatment with a topical corticosteroid. In 3 months, he showed significant improvement of the skin manifestations associated with AD, accompanied by a reduction in pruritus (EASI 25; BSA 70%; VAS of pruritus 20/100 mm) as shown in Fig. 1C. Serum levels of IgE, TARC, and LDH decreased to 28,550 IU/ml, 653 pg/ml, and 197 U/l, respectively, while the number of circulating eosinophils increased from 110 to 712/μl. In addition to the effect of dupilumab on AD, the patient also showed significant hair regrowth (Fig. 1D). SALT score decreased to 8. The significant hair regrowth was never observed prior to dupilumab initiation.
Fig 1. Skin manifestations of atopic dermatitis on the patient’s trunk (A) and alopecia areata on his head (B) at his first visit to our hospital (two months before receiving dupilumab), and 3 months after starting dupilumab treatment (C, D).
Our case showed significant improvement of AA during dupilumab treatment for AD. To date, Darrigade et al. reported a similar case (1), and Penzi et al. (2) reported a patient with AD and alopecia totalis, both of which improved with dupilumab. Moreover, Smogorzewski et al. (3) reported a case of hair recovery of the scalp, eyebrows, axillae, and groin in a patient with long-standing alopecia universalis treated with dupilumab alone. Recent studies have identified the association of AD with AA (4–6). The pathogenesis of AA has not yet been completely elucidated; however, the contribution of Th2 (T helper 2) cells to its pathogenesis has been recently indicated (7–9). Therefore, our case and previous reports suggest potential effectiveness of dupilumab for AA, although there is another possibility that the hair regrowth may not be due to dupilumab itself but as an effect of improved inflammation in AD, therefore being an indirect effect. Moreover, several papers have indicated the association of other biologics such as adalimumab (10) and ustekinumab (11) with AA. Since the pathogenesis of AA remains to be elucidated, further accumulation of data is needed to clarify the mechanism of AA. A large clinical trial would be necessary to further evaluate the effectiveness of dupilumab for the treatment of AA.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize