


1Department of Dermatology and Center for Chronic Pruritus, University Hospital Münster, Münster, 2Department of Cell Physiology, Ruhr-University Bochum, 3Department of Anaesthesiology, Intensive Care and Pain Medicine, University Hospital Münster, Münster, and 4Department of Anesthesiology and Intensive Care Medicine, Medical Faculty Mannheim, University of Heidelberg, Mannheim, Germany
#These authors contributed equally and should be considered as first authors.
Chronic pruritus (CP) is often accompanied by pares-thetic sensations like warmth, burning and stinging. The aim of this study was to analyze, whether divergent sensations are linked to structural and functional skin alterations in clinically diagnosed CP patients. Clinical responses to capsaicin, histamine, and to thermal and mechanical stimulation, intraepidermal nerve fiber density, and epidermal expression of transient receptor potential (TRP)-channels were investigated in healthy controls, and in CP patients, reporting either warmth (CP-W) or neuropathic sensations (CP-N). In CP-W, pinprick hyperalgesia and increased sensitivity to capsaicin were aligned with increased epidermal TRPV1 expression, while smaller histamine axon reflex erythema matched with significantly reduced intraepidermal nerve fiber density. CP-N showed earlier onset of sensations after capsaicin stimulation, significantly increased warmth detection threshold, and higher epidermal expression of TRPV4 compared to healthy controls. The present study contributes to the neurobiological understanding of the divergence of sensory sensations in CP, indicating new treatment targets.
Key words: sensory symptoms; TRP channels; itch; pruritus neurophysiology; nerve fiber density; quantitative sensory testing.
Accepted Apr 2, 2019; E-published Apr 2, 2019
Acta Derm Venereol
Corr: Sonja Ständer, MD, Department of Dermatology and Center for Chronic Pruritus, University Hospital Münster, Von-Esmarch-Str. 58, DE-48149 Münster, Germany. E-mail: sonja.staender@uni-muenster.de
Chronic itch may be accompanied by other sensory symptoms. Some patients report warmth sensation, while others describe stinging or burning in addition to the itch. Patients reporting warmth in addition to itch showed an increased painful response to mechanical stimuli, an enhanced itch sensation after stimulation with histamine and an increased expression of TRPV1 in the skin compared to healthy controls. Patients with stinging or burning sensations showed an early response to capsaicin, a lower sensitivity to warmth and a higher expression of TRPV4 compared to controls. These factors may contribute to the diverse sensations that patients with chronic itch experience.
Chronic pruritus (CP), one of the most frequent and scientifically underrepresented symptoms in dermatology (1, 2), usually reduces quality of life. This is increasing the need to improve the understanding and therapy of this symptom.
Due to the heterogeneity of the underlying diseases, the clinical presentation of CP patients is variable (3) and the symptom itself is rarely described as pure itching. More commonly, patients describe a combination of different paresthetic sensations and sub-qualities including burning, stinging, tingling, cold and warmth (3, 4). Most often, they report burning and stinging; qualities best known in the context of neuropathic pain (5) due to the functional neuronal impairment. In addition, a considerable number of patients describe cold or warmth along with the itch sensation. This is of special interest as thermosensitive ion channels of the transient receptor potential (TRP) family such as TRPA1, TRPV1, TRPV3 and TRPV4 are involved in the cutaneous itch transmission (6, 7). For example, TRPV1 can be activated by the application of capsaicin, release of anandamide from sensory neurons, release of leukotriene B4 from keratinocytes or by acidic tissue pH, resulting in itch, warmth and burning sensation (8–11).
Interestingly, TRPV1 and TRPA1 participate directly (agonist-activated) and indirectly (after stimulation of other receptors on the same cell membrane such as histamine or interleukin (IL) 31 receptors) in the generation of nociceptive sensations including itch signals at the cutaneous sensory nerve fibers (12). Both, and likewise other TRPs, are widely expressed on keratinocytes and cutaneous immune cells also. On keratinocytes, they contribute to thermoregulation and barrier recovery (e.g., TRPV4), or to barrier destruction (TRPV1) (13). Recent studies argue in favor of involvement of the “neuron-to-keratinocyte communication” in the generation of chronic pruritus (7). Some pruritogens and growth factors released by keratinocytes may directly activate neurons and promote nerve sprouting and sensitization (7). Others recruit immune cells such as T cells and mast cells, which can activate neurons by releasing pruritogens like histamine, IL-4, and IL-31, respectively (7). Vice versa, neuropeptides released by sensory nerves (such as substance P and calcitonin gene-related peptide (CGRP)) stimulate the release of pro-inflammatory cytokines such as IL-1α and IL-8 from keratinocytes as well as epidermal thickening and keratinocyte proliferation in a CGRP-dependent manner (14, 15).
Given the multiple ways by which the pruritogens released by keratinocytes, immune cells, and neurons interact with each other and bind to receptors on these cells, it is so far unknown, how the neuron-to-keratinocyte communication patterns translates into patients’ symptoms. We speculate that the different sensorial sub-qualities might be related to certain structural and functional changes of the neuron-to-keratinocyte communication. The aim of this translational study was to identify these structural and functional alterations in a clinically defined group of patients with CP using a set of assessments such as psychophysical responses to histamine and capsaicin, determination of the intraepidermal nerve fiber density (IENFD), epidermal TRP expression, and thermal thresholds.
This was an explorative, translational, parallel group, controlled study conducted at the Center for Chronic Pruritus, Department of Dermatology, University Hospital Münster, Germany. Before inclusion into the study, all subjects, who were recruited through our pruritus ambulance, gave written informed consent. The local Ethics Committee approved the study (2009-009-f-S), which was performed according to the Declaration of Helsinki (2008).
Adult patients (18–70 years) in our clinic, with CP (≥ 6 weeks duration), either along with warmth (CP-W) or neuropathic sensations of stinging/burning (CP-N), non-lesional skin on the inner forearm, no systemic or topical treatment 4 weeks prior to the study entrance, and healthy controls (HC) were screened for inclusion into this study. Presence of simultaneous warm and cold sensations, genital, aquagenic or brachioradial pruritus, prurigo nodularis, lichen planus, atopic diathesis, chronic pain syndrome, intake of analgesics, and tendency to form keloids were all exclusion criteria.
After filling-in the Neuroderm questionnaire (16) which is descriptively recording the pruritus characteristics including intensity by the Visual Analogue Scale (VAS), the subjects underwent the first stimulation with capsaicin and histamine, followed by Quantitative Sensory Testing (QST) on another day. Finally, skin biopsies were taken.
Capsaicin cream (0.04%, Thermo Bürger, Bad Harzburg, Germany) was applied topically to a 3 × 3 cm area at the inner side of the forearm with a 20 min observational period. Every 5 min the subject evaluated the presence and intensity (using the numeric rating scale, NRS, range 0–10) (17) of itching, burning, stinging, and warmth.
Histamine 0.02 ml (0.01%, Allergopharma, Reinbek, Germany) was injected intra-cutaneously with a BD-Microfine insulin syringe to the inner side of the contralateral forearm (18–20). After a period of 20 min, erythema and wheal were manually measured by determining the mean length and width of the affected area. Pruritus sensation was evaluated by VAS.
The QST, a battery of tests used to determine possible somatosensory dysfunctions, was performed in fixed order, according to the protocol of the German Research Network for Neuropathic Pain (see Appendix S1) (21). The tests are based on thermal and mechanical stimulations, assess the superficial skin sensitivity and deep pain sensation and can determine sensorial gain (hyperalgesia, allodynia) or loss (hypoalgesia, hypoesthesia).
Four, 4 mm punch biopsies (pfm medical, Cologne, Germany) were obtained under local anesthesia (Xylonest 1% with adrenaline 1:200000; Astra Zeneca, Wedel, Germany) from the pruritic skin on the arm (n = 24, 77.4%), and, due to cosmetic reasons, from the flank or shoulder (n = 7, 22.6%). IENFD was determined following the Schuhknecht et al. method (22). TRP immunostaining for TRPV1-4, TRPA1 and TRPM8 was performed and analyzed for 5 CP-W and CP-N, each, including their matching HC. Quantitative real time polymerase chain reaction (qPCR) was performed for the evaluation of gene expression of TRPV1 (see Appendix S1).
Data were collected and encoded using Microsoft Excel for Windows and statistical analysis was done using SPSS version 24 (SPSS Inc., USA.). The Mann-Whitney U test was performed to compare independent variables as in the analysis of QST, IENFD and the clinical reaction after histamine injection. The chi-square test was used for evaluating the frequency distribution of sensitivity to capsaicin. For experimental procedures comparing two dependent variables, we employed the Cochran´s Q test, which was applied to evaluate the time course of the clinical response (i.e. the number and percentage of patients reporting a sensory sensation) after capsaicin application. The Friedman test was performed for analyzing the pruritus intensity across time after capsaicin application. For group comparisons, the Kruskal-Wallis test followed by the Dunn’s test was applied. The frequency of reactivity was calculated using the chi-square test. In the analysis of TRP immunostaining, the Wilcoxon signed-rank test was used to compare two related samples. We used the Pearson correlation coefficient for the correlation analysis of IENFD and clinical parameters. In all statistical tests, a two-sided significance test was performed and p ≤ 0.05 was considered statistically significant. Due to the explorative nature of this study, no correction of the statistical threshold for multiple comparisons was performed.
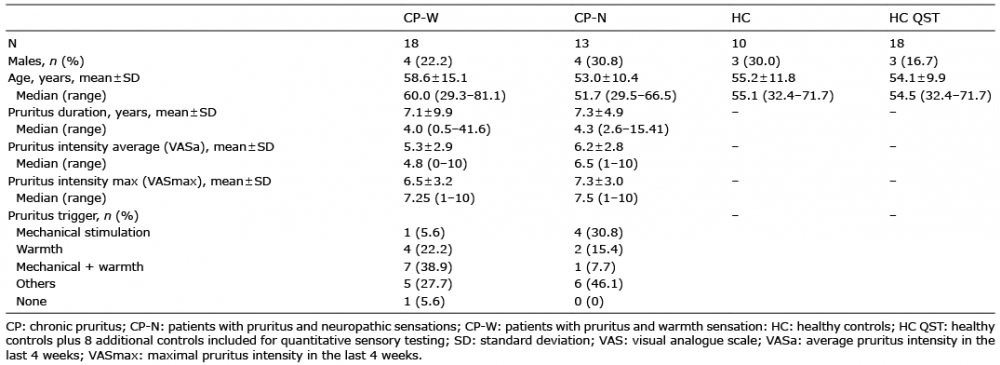
Between November 2011 and October 2012, 31 patients, of whom 13 (41.9%) experienced itch combined with neuropathic sensations (CP-N) and 18 (58%; CP-W) pruritus with sensation of warmth (Table I) were included into the study. Ten HC were matched to 5 CP-W and 5 CP-N patients, with respect to gender and age, and were stimulated on non-pruritic, non-lesional skin. Additional 8 HC controls were included for QST, so that the HC QST group consisted of 18 subjects.
Table I. Sample characteristics
The majority of the subjects (60.0–84.6%) reacted with itch, stinging, warmth or burning to the capsaicin stimulation without significant differences (n.s.) versus HC (CP-W, p = 0.677; CP-N, p = 0.341) (Table II). Thus, they were attributed to the capsaicin responder group. However, when comparing the time course and the intensity of the capsaicin-induced sensations, the CP-W and CP-N showed a different pattern than the HC. CP-W showed a continuous increase in all symptoms with a peak at 20 min, while CP-N exhibited an early rise in the intensity of all symptoms, which remained stable for burning, while the other sensations gradually declined (Fig. 1, Table II). When comparing symptom intensities, CP-N showed higher NRS values for pruritus, burning and stinging sensations than HC (Table II). Although CP-W showed a significant increase in symptom intensity with time (Fig. 1), the difference was not significant when comparing to HC.
Table II. Responses to stimulation with a topical 0.04% capsaicin cream
Fig. 1. Different sensory reaction pattern after topical application of capsaicin. Percent of subjects (A, C, E) reporting pruritus, burning or warmth sensation (clinical response) and sensation intensity (B, D, F; measured by numeric rating scale (NRS)) over time (0–20 min) after topical application of 0.04% capsaicin cream. Chronic pruritus (CP) patients with warmth sensation (CP-W) showed a continuous increase in the number of responding subjects (C) and intensity of sensations. Patients with chronic pruritus and neuropathic sensations (CP-N) exhibited an early rise, which remained stable for burning while the other sensations relieved. *p < 0.05, **p < 0.01, (clinical response, Cochran’s Q test; intensity NRS, Friedman test). HC: healthy controls.
Histamine induced a wheal, flare and itch reaction in all subjects. The wheal was smaller (CP-W, p = 0.001; CP-N, p = 0.015) in patients than in HC, while the ery-thema was less (CP-W, p = 0.003; CP-N, n.s.), the pruritus more intense (CP-W, p = 0.022; CP-N, n.s.) in CP-W compared to HC (Fig. 2). No significant difference in histamine reactivity was observed between CP-W and CP-N (Fig. 2).
Fig. 2. Different reaction to intracutaneous injected histamine in patients with chronic pruritus (CP) and healthy controls (HC). A significantly smaller wheal (A) and erythema (B), but a more intense pruritus (C) in CP-W than in HC was observed. CP-N demonstrated a significantly smaller wheal than HC. *p < 0.05, **p < 0.01, central box spans the interquartile range, line inside the box shows the median, whiskers from minimum to maximum, dots show outliers (Mann-Whitney U test). CP-W: patients with pruritus and warmth sensation; CP-N: patients with pruritus and neuropathic sensations; VAS: visual analog scale.
Compared to HC, higher mechanical pain sensitivity (MPS) in CP-W (p = 0.026) and higher warmth detection threshold (WDT) in CP-N (p = 0.027) were detected (Table III, Fig. 3). For the remaining QST parameters no differences were recorded between patient groups and controls (n.s.).
Table III. Results of quantitative sensory testing (QST) per group
Fig. 3. Patients with chronic pruritus (CP) showed alterations in mechanical pain sensitivity and warmth detection threshold. (A) CP-W demonstrated a significantly higher mechanical pain sensitivity (MPS), (B) CP-N showed a significantly increased warmth detection threshold in comparison to healthy controls (HC). *p < 0.05, central box spans the interquartile range, line inside the box shows the median, whiskers from minimum to maximum, dots show outliers (Mann-Whitney U test). CP-N: patients with pruritus and neuropathic sensations; CP-W: patients with pruritus and warmth sensation; NRS: numeric rating scale.
IENFD was significantly decreased in CP-W (p = 0.031, 8.2 ± 5.3 fibers/mm) but not in CP-N (11.0 ± 9.3 fibers/mm) when compared to HC (13.0 ± 5.3 fibers/mm). No significant difference between CP-W and CP-N was observed. IENFD of CP-W showed a statistically significant negative correlation with the maximal itch intensity (VASmax) (r=–0.57, p = 0.034) experienced in the 4 weeks prior to the study, while in both groups no correlation between IENFD and the duration of pruritus (n.s.), average pruritus intensity (n.s.) or erythema after histamine injection (n.s.) was detected.
A significantly higher expression of TRPV1, TRPV2 and TRPM8 was shown by immunostaining in the epidermis of CP-W when compared to HC (TRPV1: p = 0.034; TRPV2: p = 0.034; TRPM8: p = 0.034). By means of qPCR, we detected a significantly stronger relative gene expression (median 1.51) of TRPV1 in CP-W compared to CP-N (median 0.61; p = 0.002) and HC (median 0.87; p = 0.009). Furthermore, an up-regulation of TRPV4 could be observed in CP-N when compared to HC (p = 0.034). No differences were recorded between CP-N and CP-W.
Fig. 4. Different expression patterns of TRP channels in chronic prutitus (CP) patients with warmth sensations (CP-W) and neuropathic sensations (CP-N) by TRP immunostaining (A, B) and qPCR (C). (A) A significantly higher expression of warm (TRPV1, TRPV2) and cold (TRPM8) channels was found in CP-W. (B) An up-regulation of TRPV4 could be observed in CP-N. (C) CP-W showed significantly stronger relative gene expression to TRPV1 compared to HC and CP-N. *p < 0.05, **p < 0.01, bars are mean ± SD (Wilcoxon test). HC: healthy controls.
Based on the clinical observation that patients with CP report different sensory sub-qualities associated with itch, we conducted this translational study in clinically defined groups, trying to understand if these differences correspond to the functional and structural skin changes.
Though we only included a small number of patients, we found significant differences in cutaneous responses between the two studied groups and their matched HC. We could not verify the simplistic mechanism by which patients reporting warmth sensations, in addition to their spontaneous pruritus would have lower warmth detection thresholds or that those also reporting painful sensations would respond more sensitively to the evoked pain. This result is in-line with a mismatch of evoked vs. spontaneous pain responses found in the chronic neuropathic pain patients (23). The key differences between HC and patients were that patients had an earlier onset of sensations following topical capsaicin application, smaller erythema, yet more intense itch following the histamine stimulation, and reduced IENFD. Patients with CP-N had a particularly early onset of sensations after topical capsaicin, increased warmth detection threshold (possibly due to lower IENFD), and showed a higher epidermal expression of TRPV4, whereas in patients with CP-W epidermal expression of TRPV1 was particularly high.
Topical capsaicin induced a weak pruritic sensation in HC, a finding that has already been described by volunteers upon the first application of capsaicin (24). However, capsaicin-induced itch rapidly desensitizes upon repeated application (24). Although we saw an early onset, we did not observe more intense capsaicin-induced itch in the patients as reported after noxious skin stimulation of atopic dermatitis skin (25). However, the delay of sensation, following the topical capsaicin application was shorter in the patients, which would primarily suggest faster skin penetration due to a reduced epidermal barrier function. Interestingly, both TRPV1 (26, 27) and TRPV4 (28) have been implied in the modulation of epidermal barrier function. Thus, the higher epidermal TPRV1 levels in the CP-W group, confirmed at the molecular level (qPCR), would be consistent with the shorter delay. Increased TRPV1 expression in keratinocytes was previously described in patients with prurigo nodularis (29), itching burn scars (30), as well as herpes zoster pain (31). It is speculated that epidermal TRPV1 plays a key role in zoster-associated pain through the release of pro-inflammatory keratinocyte mediators, reduction of innervation density of the epidermis, and peripheral nerve sensitization (31). Studies on these mechanisms are scarce, however, if this holds true, it would link our findings of pinprick hyperalgesia and increased sensitivity to capsaicin to an increased epidermal TRPV1 expression.
Moreover, increased TRPV4 in the epidermis of CP-N patients could also be consistent with the shorter post-capsaicin sensation delay and the reduced barrier function. New findings also suggest that TRPV4 on keratinocytes is crucial for spontaneous scratching in the dry skin mice model (32). Another study demonstrated the role of TRPV4 in serotonin-evoked scratching (33). While the exact role of TRPV4 and its connection to the neuronal signaling await further exploration, these findings have an interesting translational relevance, as topical TRPV4 antagonists inhibited histamine-induced scratching in mice (34).
Histamine induced a smaller wheal and erythema, but a more intense pruritus in CP-W as compared to HC. The smaller axon reflex erythema could be the result of a lower release of neuropeptides, caused by permanent activation (35) and/or the significantly lower innervation density (36, 37). In these patients (CP-W), the reduced IENFD correlated negatively with the itch intensity. The increased itch sensation upon histamine stimulation remains unclear, as it could be of peripheral or central origin (38). In future studies, a 20 min observational period could be foreseen as well for the histamine test, including additionally an assessment of the expression of the H1-receptor.
A limitation of this study is the subjectivity of pruritus. Psychosocial aspects can be the result of pruritus but also its root-cause, and such aspects were not taken into account (39). The large number of clinical tests brought in relation to laboratory results in this study was interesting. The high time expenditure for the participants as a consequence of all these tests, should be considered when planning the necessary larger future studies. Since this is a study of explorative nature, future studies with a confirmatory design are needed to corroborate our findings.
In conclusion, our study demonstrated the translational relevance of clinical, psychophysical, morphological and neurophysiological phenotyping of chronic pruritus patients. Our CP patients, defined by divergent sensory sub-qualities, differed in clinical responses to chemical, thermal and mechanical stimuli, nerve fiber architecture and expression of TRP channels. Thus, the study offers valuable targets for the development of novel pruritus treatments, which are urgently needed. In addition, a thorough phenotyping of CP patients might allow generation of hypotheses of chronic pruritus neurobiology and might explain patients´ response or failure to modern therapies. Further research into the matter, including a larger cohort of patients, is strongly advised.
We thank E.R. Burnett for proofreading and editing, and M. Marziniak M.D. and H. Karajiannis for their contributions to the manuscript. This work was supported by a grant from the German Research Foundation (DFG) to SST (STA1159/4-1) and to KA (AG271/1-1).
This work was supported by a grant from the Interdisciplinary Center for Clinical Research Münster (IZKF; No: CTRP 07 to SST and EPZ).
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize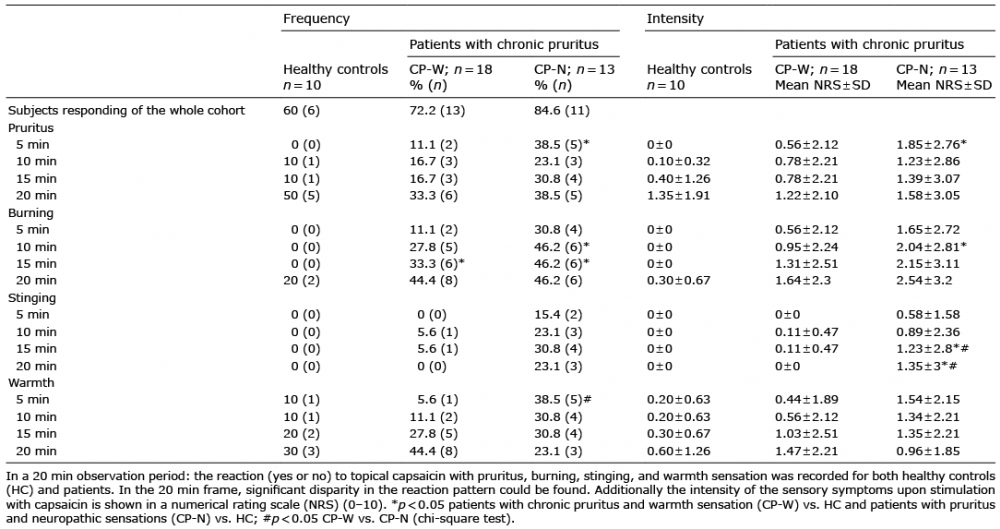 Click to show fullsize
Click to show fullsize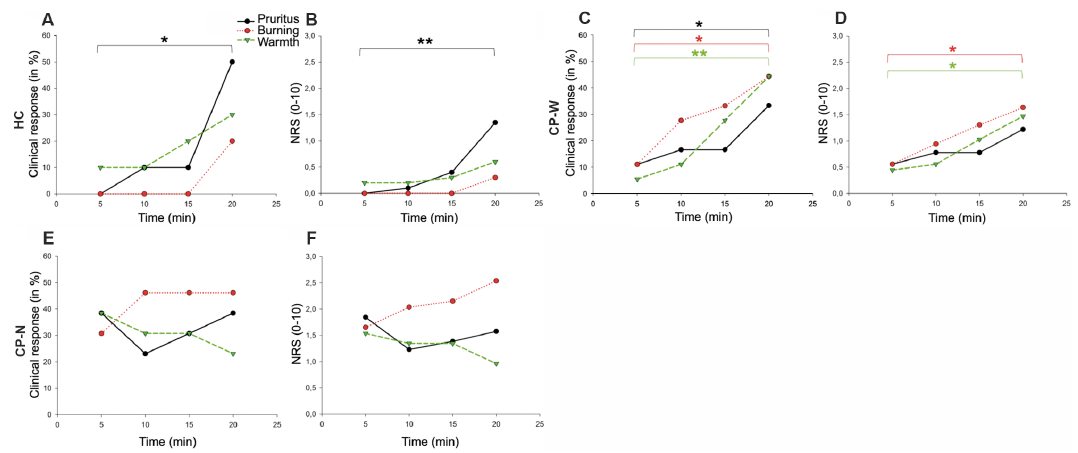 Click to show fullsize
Click to show fullsize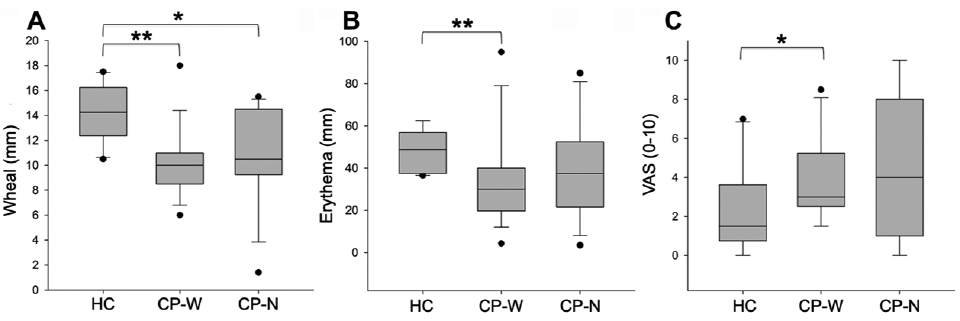 Click to show fullsize
Click to show fullsize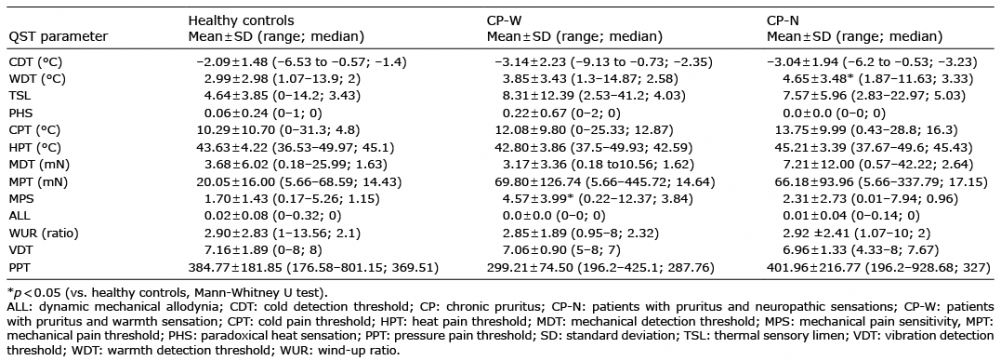 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize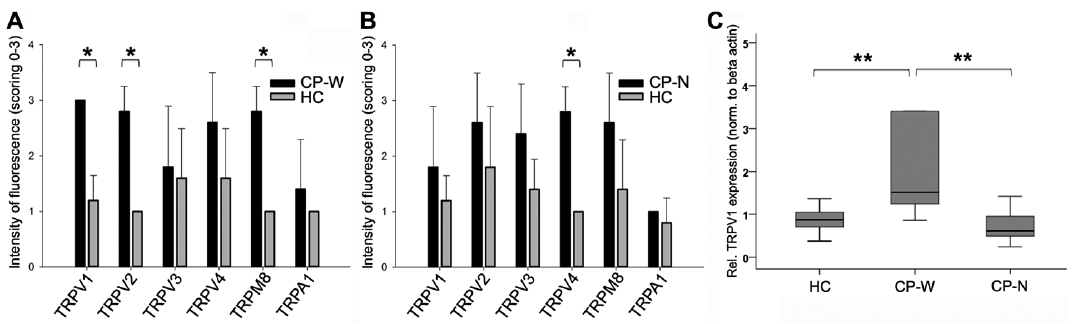 Click to show fullsize
Click to show fullsize