


1Department of Dermatology, Skåne University Hospital, Department of Clinical Sciences, Dermatology and Venereology, 2Department of Surgery and 4Department of Oncology and Pathology and Cancer Epidemiology, Skåne University Hospital, Department of Clinical Sciences, Lund University, 3Faculty of Medicine, Department of Clinical Sciences, Oncology and Pathology, and 5Department of Dermatology, Helsingborg Hospital, Department of Clinical Sciences, Dermatology and Venereology, Lund University, Lund, Sweden
The incidence of cutaneous squamous cell carcinoma has increased rapidly in Sweden in the past decades. Here, we present a prospective study of the Melanoma in Southern Sweden (MISS)-cohort, with 29,460 participating women in southern Sweden that investigates the risk factors for cutaneous squamous cell carcinoma. Data on the host and skin cancer risk factors were collected through questionnaires and then matched with the National Cancer Registry. Statistical analyses were based on uni- and multivariable Cox proportional hazards models, using age as the time-scale. We found that sunbed use (hazard ratio (HR) 1.2, 95% CI: 1.1–1.4), red and light blond hair (HR 1.6, 95% CI: 1.1–2.3), freckles (HR 1.4, 95% CI: 1.1–1.8) and immunosuppressive medications (HR 2.1, 95% CI: 1.3–4.5) were independent risk factors. Furthermore, we observed a dose-dependent relationship between sunbed use and the development of cutaneous squamous cell carcinoma. Our findings support the idea of integrating dermatological follow-up examinations for immunosuppressed patients and banning the use of sunbeds in order to prevent cutaneous squamous cell carcinoma.
Key words: cutaneous squamous cell carcinoma; risk factors; sunbed; prospective cohort.
Accepted Apr 16, 2019; E-published Apr 16, 2019
Acta Derm Venereol
Corr: Gustav Boelsgaard Christensen, Department of Dermatology, Skåne University Hospital, Lasarettsgatan 15, SE-222 41 Lund, Sweden. E-mail: gustav.christensen@skane.se
There has been an increase in the number of skin cancers in Sweden in the last decades. We looked closer at one skin cancer in particular – squamous cell carcinoma. In order to be able to prevent squamous cell carcinoma, we need to understand which risk factors are most important. We studied a large group of Swedish women and looked into which risk factors play a role in getting squamous cell carcinoma. Having freckles and red or light blond hair, taking medications that suppress the immune system and using sunbeds play a part.
Over the past 10 years, there was an annual increase of 6.5% for Swedish women and 5.5% for Swedish men in the incidence of cutaneous squamous cell carcinoma (cSCC), making it the most and second most rapidly increasing malignant tumour in Sweden (1, 2). This trend has been observed for light-skinned people worldwide as well (3–6). A cSCC diagnosis can be lethal and surgical excision is the first line treatment in forms of invasive cSCCs. A patient with the suspected diagnosis is often referred from primary care to a dermatology department for diagnosis and subsequent treatment. Due to the rise in incidence, the number of patients in dermatology departments has been increasing, which represents a growing economic burden on the healthcare system.
As with most cancers, the interaction between phenotypic, genotypic, and environmental factors determines the individual risk for developing cSCC. As such, understanding these risk factors and implementing evidence-based preventive strategies are essential to combat the rising incidence of cSCC.
Analysing risk factors identified in prospective studies with no recall bias, can help to achieve this goal. The majority of the studies, examining risk factor contribution to cSCC, to date are retrospective in nature and very little focus exclusively on women. In contrast, the aim of the present study is to prospectively investigate a cohort of women and thereby elucidate the influence of both phenotypic (colour of hair and eyes, freckles and naevi count) and environmental factors (medicine intake, educational level, smoking habits and UV exposure) on cSCC incidence.
The MISS (Melanoma in Southern Sweden) cohort was established in 1990–1992 and is still followed prospectively. Swedish-born women (1,000 women per calendar year, born between 1925 and 1965), living in the Southern Sweden’s health care region, with no prior diagnosis of invasive cancer were selected for the study. The women included in the cohort were chosen through random computerized selection from the Population/Census Registry and were controlled to have no prior diagnosis of invasive cancer through the Regional Cancer Registry before the final inclusion. At baseline 40,000 women were included into the study. Non-responders were sent a reminder letter.
The invited women were asked to answer a written questionnaire on the possible risk factors for skin cancer and breast cancer. The women who entered the study provided written informed consent. The list of participants was thereafter continuously crosschecked with the Regional Cancer Registry for the occurrence of any kind of malignancy, including cSCC. Follow-up time (person-years) was measured from the beginning of the study until the diagnosis of first primary cSCC, death, immigration or the end of the study period (20 years).
This study used a standardized questionnaire that has been validated in our previous publications (7–9). The original questionnaire was developed during the 1980s for the purpose of gathering information on the possible risk factors for cutaneous malignant melanoma and breast cancer. However, the design of the questions made this survey applicable to the analysis of risk factors for cSCC, as well.
From the questionnaire, we included items on previously known and suspected risk factors for skin cancer (7). Data were collected on phenotypic characteristics including hair colour, eye colour, freckles and naevi count on one arm, in addition to the data such as potential risk factors: level of education, outdoor work, use of sunbeds and UV (ultraviolet) lamps, intake of oral contraceptives (OC), hormone replacement therapy (HRT), other medications taken for over a month, smoking habits, number of pregnancies and if they have ever lived in a sunny subtropical to tropical climate. Medications were grouped according to the International Anatomical Therapeutic Chemical (ATC) classification system. For medications considered relevant to this study, i.e. non-steroidal anti-inflammatory drugs (NSAIDs) and immunosuppressive drugs, patients were coded as “users” if they took these medications for over one month and “non-users” when they were medication-free.
Data on cancer diagnoses up to December 31, 2007 were collected from the National Cancer Registry and from the Regional Cancer Registry up to April 13, 2011. In the last period, a few women moved out of Southern Sweden’s healthcare region and had been diagnosed with cSCC between the aforementioned dates.
Incidences of cSCC (events per 100,000 person-years) are presented for each level of the hypothesized risk factors. To estimate the increased risk associated with each factor, we used a univariable cause-specific Cox regression analysis, using age as the time-scale, i.e. subjects enter the analysis at their baseline age (age at which they completed the questionnaire) and exit at their event, censoring age or death. By using age as the time-scale, confounding risk factors for age were already eliminated in the univariable analyses. Results are presented as hazard ratios (HR) with 95% confidence intervals (CI) and p-values.
For graphical illustration, we presented the cumulative incidence of cSCC and treated death as a competing event. To investigate the independent contribution of each risk factor, we used a multivariable Cox regression analysis that included information on high number of naevi, freckles, red or light blond hair, ever having smoked, sunbed use, ever having lived in a sunny climate, occupational outdoor working, use of immunosuppressive medications (over one month), higher education, ever having used OC, more than two pregnancies, ever having used HRT and NSAID use (over one month). In the main multivariable analysis, sunbed use was represented through a linear score (0 = never, 1 = 1–3 times per year, 2 = 4–10 times per year, 3 = over 10 times per year) to interrogate trends associated with each factor. To further investigate the impact of sunbed use, it was included as a factor on these 4 levels; furthermore, we performed a comparison between “ever-users” and “never-users”. Complete case analysis was used in the multivariable setting.
In both the multivariable and univariable Cox analyses, the proportional hazards assumption was tested using the Schoenfeld’s test (tests with p < 0.05 commented on in Table II). As a sensitivity analysis (not subject to the proportional hazards assumption), we calculated the univariable p-values using the log-rank test (with age as the time-scale). Because these results were comparable to those from the Cox-regression, we did not include them in this report.
Of the initially 40,000 invited women, 29,460 agreed to participate in the study (response rate 74%). We excluded one subject with a cancer diagnosis prior to answering the questionnaire and 38 subjects with at least one cancer diagnosis prior to developing cSCC. Of the remaining 29,421 women, 333 were diagnosed with cSCC, 124 of which were invasive and 209 were in situ.
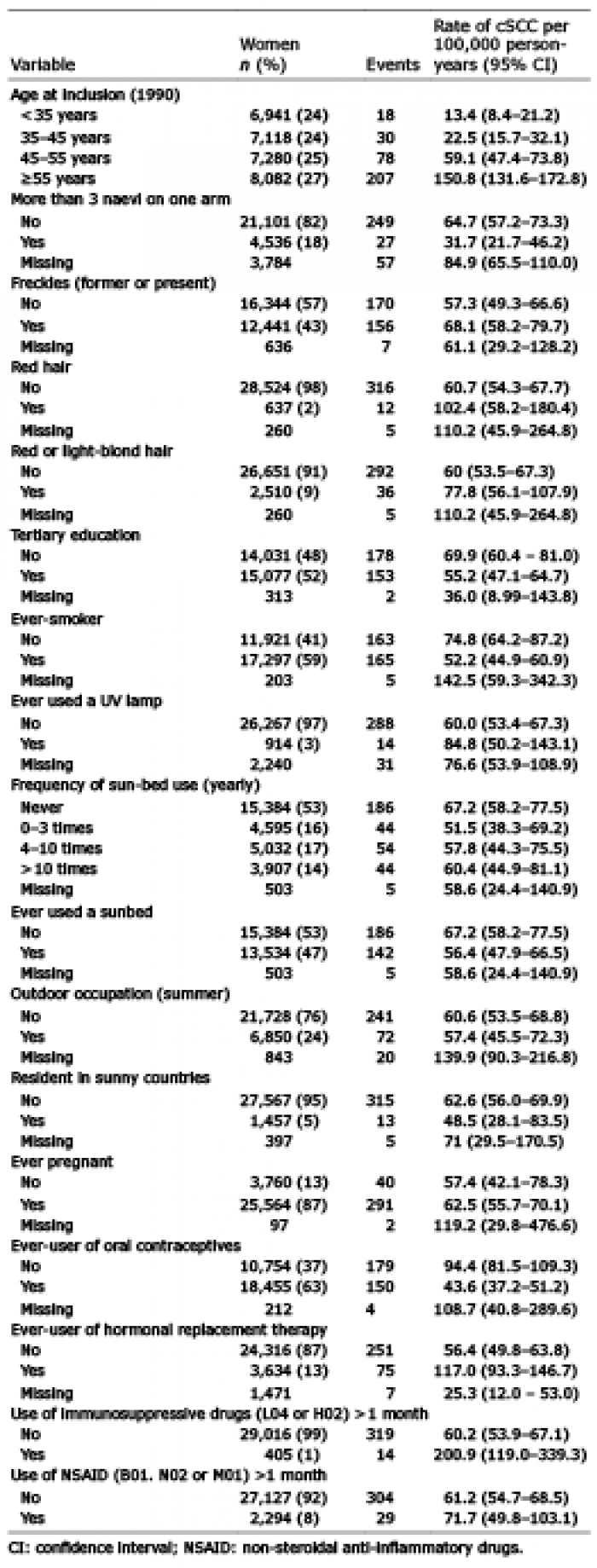
The distribution of the included risk factors and the corresponding incidence of cSCC are presented in Table I.
Table I. Group size and incidence of cutaneous squamous cell carcinoma (cSCC) separated for risk factors and base-line variables
In the univariable analysis, we compared the incidence of cSCC with its potential risk factors, using a 95% CI (Table II). The variables with the strongest crude influence on cSCC incidence were sunbed use up to 3 times per year vs never (HR 1.34), sunbed use between 4 and 10 times per year vs never (HR 1.55), sunbed use over 10 times per year vs never (HR 1.88), freckles (HR 1.53), red hair (HR 2.00), red or light blond hair (HR 1.63), use of OC (HR 1.30) and the use of immunosuppressive medications for over one month (HR 2.51). The independent effects of the risk factors were determined using a multivariable analysis, using a 95% CI (Table III). We included all of the risk factors from the univariable model, except those that represent the re-categorization of an included variable in order to avoid problems with co-linearity. To account for the possible age-dependent differences (most notably in the use of sunbeds, which did not become popular in Sweden until the 1980s), we adjusted according to the birth cohort (4 groups). We further explored the possible interaction between sunbed use and birth cohort but there was no evidence for such an interaction in our data (p = 0.7, data not shown). In the multivariable analysis, sunbeds (HR 1.18 per step in score), red or light blond hair (HR 1.58), freckles (HR 1.43) and immunosuppressive medications (HR 2.16) were associated with an increased HR for cSCC. The other variables analysed had no associations with cSCC diagnosis in this model.
Table II. Univariable Cox regression analyses of risk factors for cutaneous squamous cell carcinoma (cSCC)
Table III. Multivariable Cox regression analysis of risk factors for cutaneous squamous cell carcinoma (cSCC), based on 247 events in 22,690 women (complete case analysis)
Sunbed use. The multivariable analysis, described above, revealed a positive association between cSCC incidence and sunbed use (HR 1.18; 95% CI 1.04–1.32) for each score level (0–3). By using a more detailed multivariable analysis, we further elucidated this trend by including sunbed use as a factor on these 4 levels and compared the sunbed-users to the never-users to obtain an HR 1.38 (95% CI 0.95–2.0), HR 1.47 (95% CI 1.02–2.1), HR1.62 (95% CI 1.09–2.42) for sunbed use 0–3 times/year, 4–10 times/year and > 10 times/year, respectively. The increased risk of cSCC for sunbed users compared to never-users is illustrated graphically in Fig. 1.
Fig. 1. Curves showing the relationship between the cumulative incidence of cutaneous squamous cell carcinoma (cSCC) in ever-users and never-users of sunbeds.
The incidence of cSCC has been increasing in Sweden and globally since the last 40 years. For Swedish women this is the most rapidly increasing cancer of all. Therefore, primary and secondary prevention of cSCC have high priority. In this prospective study we have confirmed that sunbed use, having freckles, red or light blond hair and using immunosuppressive drugs are independent risk factors for developing cSCC. Our findings are in line with the literature (10–18) and confirm a distinct relationship between cSCC risk and sunbed use.
One of the strengths of our study is its prospective design with a large cohort and data collected over a long period of time. Another strength is the inclusion of cross-referencing with the National Swedish Cancer registry, where approximately 98% of all cancer diagnoses in Sweden are registered, according to the unique individual personal identification numbers.
Focusing our study solely on female participants serves as both a strength and a limitation. The former, as it is important to find possible differences in risk factors among men and women, the latter being that we cannot generalize our findings to male patients. Very few of the women in our cohort worked outdoors and this likely underlies the absence of an association between outdoor work (i.e. chronic UV exposure) and increased cSCC risk. Previous studies have described such an association between cSCC and outdoor work for men (10, 11, 19, 20). Another limitation is the lack of information on possible unknown or recently revealed confounders, as the data is based on a questionnaire constructed in the early nineties. Hence we could not adjust for all possible confounders, such as the use of sun protecting agents and we cannot comment on their possible effect on the risk. Also, we have not been able to look at family history of cSCC as a risk factor in our study.
Interestingly, for many perceived risk factors for cSCC, we found no statistical evidence for the influence of the risk in the MISS cohort. For example, our study provided no evidence of smoking being a risk factor for cSCC, which contradicts the findings from a meta-analysis (21) and from a more recent study from Australia but aligns with two other studies from Australia and Sweden, respectively (22, 23). Our findings were also contrary to those in the literature, regarding NSAID intake (23, 24), because, according to our data, this factor neither increased nor decreased cSCC risk. Both evidence from the literature and our evidence support the lack of association between cSCC risk and OC use (24, 25) or education level (26, 27).
Fair skinned individuals with red to blond hair have been reported as being at an elevated risk for developing cSCC and cutaneous malignant melanoma (cMM) (12, 16–18, 28, 29). This predisposition is supported by the data in our study as well. The accepted explanation for this phenomenon is that population’s inability to tan, which corresponds to their predominant production of yellow-reddish pheomelanin instead of brown-black eumelanin. Given that the individual phenotype cannot be altered, how can we protect our fair-skinned population from this risk? This is of particular importance to the Nordic countries, including Sweden, where this skin type is overrepresented. The answer likely includes improving primary prevention (30, 31). In this regard, more randomised, controlled prevention studies are needed, but in Australia, Green et al. (32) have already shown that daily sunscreen use can prevent cSCC.
A well-known environmental risk factor for cSCC is the use of immunosuppressive medications and several studies have shown that the risk of cSCC is markedly increased following organ transplantation (14, 15, 28). This is in line with our findings that the use of these drugs for a month increases the risk significantly. This highlights the importance of prompt as well as continuous dermatological surveillance and education about the primary prevention for patients with long-term immuno-suppression. Hence, evidence-based information to these patients, concerning the most effective way of primary prevention of cSCC, and also skin cancer screening by total body examination should be proposed and possibly standardized in future national guidelines.
The most important known risk factor for cSCC (3, 10, 12), cMM, and basal cell carcinoma (BCC) is ultraviolet radiation (UVR) exposure (10, 11, 29). In this study, we examined factors that inherently involve UVR exposure such as working outdoors, living in a sunny climate, and using UV-lamps/sunbeds. Additionally, we could not confirm that a history of being a resident of a country with a sunny climate (i.e. closer to the equator, more ambient UVR) impacted the cSCC incidence, as has been described by several previous studies (12, 33, 34). This is also likely explained by an underrepresentation of this subpopulation in our cohort or by the survey’s lack of information concerning the duration of stay in a sunny climate.
Investigating the contribution of sunbed use and cSCC risk is interesting partly because this risk factor can be influenced by information and regulation (35, 36). While age limits for sunbeds have been already enacted in several other countries such as Italy and Australia (36–38), these efforts were only recently settled in Sweden (September 2018). This represents a very promising and proactive skin cancer preventive strategy as several previous studies have shown that sunbeds contribute to melanoma and cSCC development (7, 13, 16, 39–43).
The present study confirms that the use of sunbeds is an independent risk factor for the increased cSCC incidence. Because our study is restricted to women, the confirmation of the increased risk conferred by sunbeds might be attributed to the fact that women are traditionally more prone to sunbed use or that the correlation between sunbed use and cSCC risk in other studies might have been diminished if men were studied, since men tend to use sunbeds less than women (36). In Sweden, the incidence of cSCC is somewhat higher in women than in men. Is it possible that this difference stems from the higher rates of sunbed use among women? Interestingly, we can conclude that as sunbed use increases, so does the risk of developing cSCC. This dose-response relationship confirms the negative health impact of using sunbeds.
In conclusion, this large, prospective study firmly establishes that the use of sunbeds is an independent risk factor for cSCC in Swedish women. The use of immunosuppressive medication for over one month and having freckles and red or light blond hair were also independent risk factors. Our findings support implementing regular dermatological evaluation as a standard practice for patients who are immunosuppressed, and banning the use of sunbeds.
Funding sources: Swedish Cancer Society, Swedish Research Council, ERC advanced grant 2011-294576. Mats Paulssons Trust, Stefan Paulssons Trust, S.R. Gorthon foundation, T. Zoegas foundation, Welander Finsen foundation, G. Nilsson cancer foundation, ALF grants.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize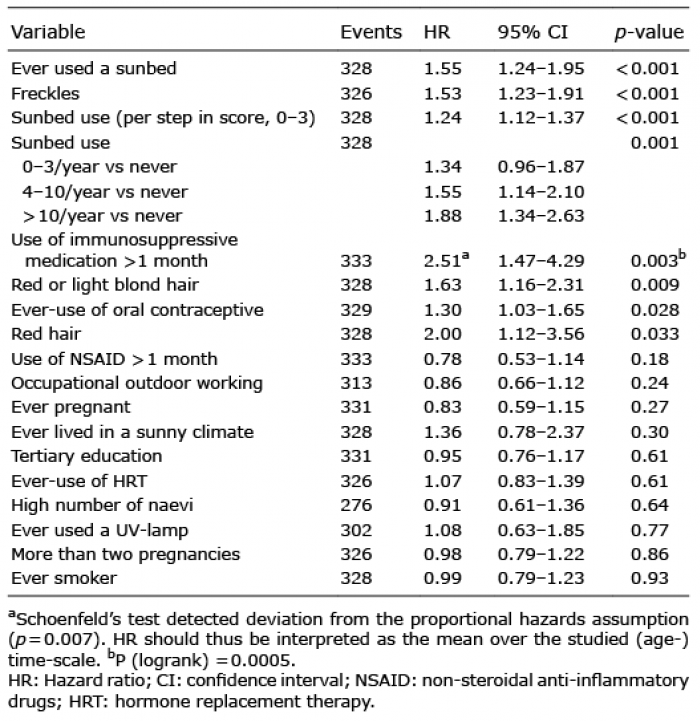 Click to show fullsize
Click to show fullsize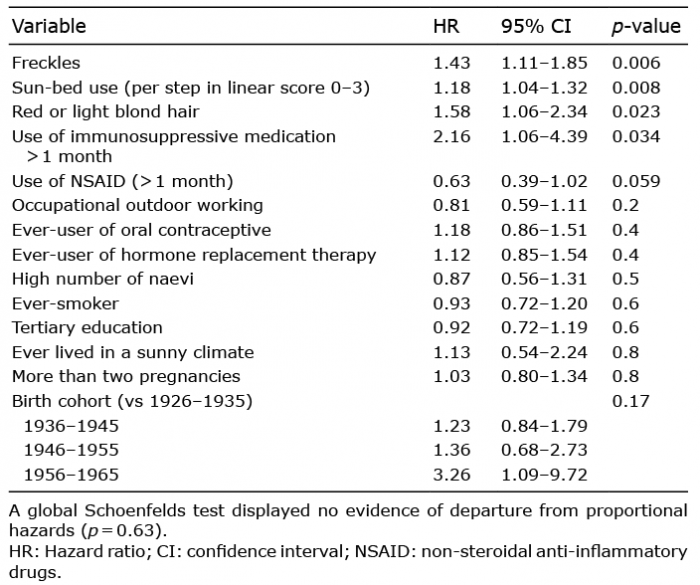 Click to show fullsize
Click to show fullsize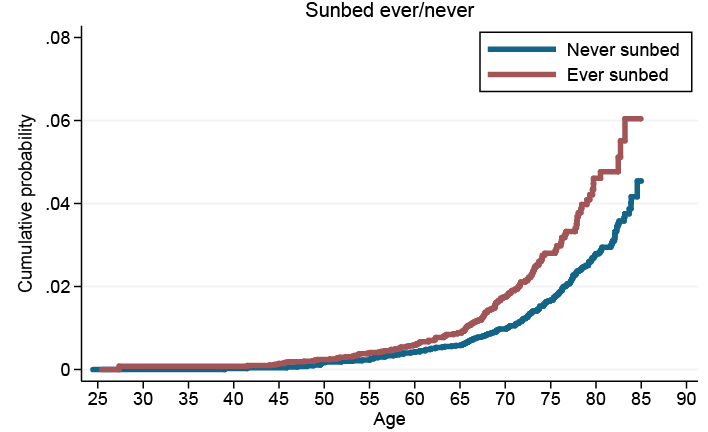 Click to show fullsize
Click to show fullsize