


Department of Dermatology, University of Franche-Comte, EA-3181, Teaching Hospital, 3 Bd Fleming, FR-25030 Besancon cedex, France. E-mail: charleenardin@hotmail.fr
Accepted Apr 16, 2019; E-published Apr 16, 2019
Vitiligo is an autoimmune skin disorder characterized by hypopigmented skin lesions, originating from the loss of functional melanocytes in the epidermis. Vitiligo can occur in patients suffering from melanoma and has long been recognized as an independent favourable prognostic factor for melanoma patients, correlating with improved overall and tumour-free survival rates (1). Vitiligo has been reported in patients suffering from advanced melanoma, treated with immune checkpoint inhibitors (ICI) (2, 3). Furthermore, the onset of vitiligo in patients treated with the anti-PD-1 (programmed cell death 1 protein) antibody for advanced melanoma is associated with improved response and better outcomes (4–8). Here, we report a case of vitiligo re-pigmentation, which was associated with disease progression in a patient treated with pembrolizumab for metastatic melanoma.
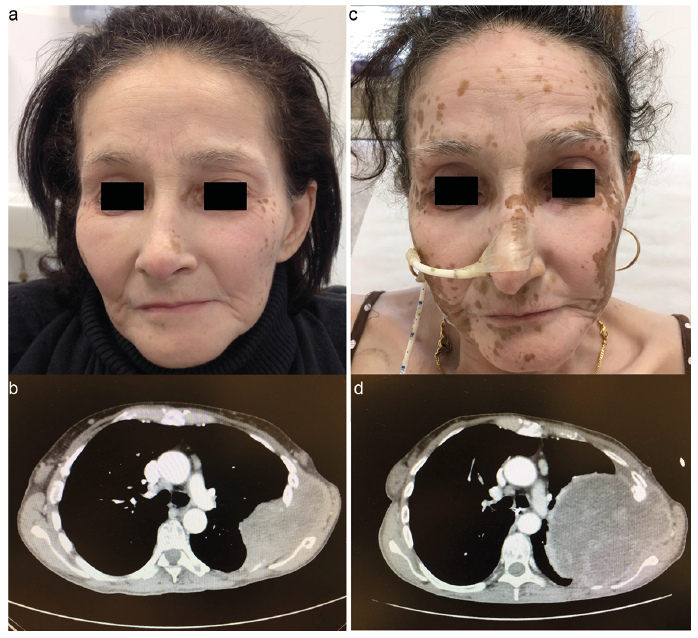
A 50-year-old woman presented to our hospital with metastatic melanoma. She had a past medical history of left uveal melanoma, treated with surgery one year earlier. Molecular analysis of the metastatic liver lesion revealed a GNAQ mutation. She had no medical and family history of autoimmune diseases. A computed tomography (CT) scan showed liver, lung, brain, lymph nodes, subcutaneous, medullar and bone metastases with spinal cord compression. Pembrolizumab was initiated (2 mg/kg, every 3 weeks) simultaneously with radiation therapy for vertebral metastases. Paracetamol was prescribed for back pain. One month after pembrolizumab initiation, she developed extensive vitiligo (Fig. 1A). In addition, she developed hypothyroidism, without thyroid antibodies, and was treated with thyroid hormone therapy. At 3 months follow-up, CT scan showed stable disease (Fig. 1B). However, after 16 infusions of pembrolizumab (46 weeks of treatment), partial vitiligo re-pigmentation was observed on the face only. Of note, this occurred in the winter without any specific treatment or sun exposure (Fig. 1C). Lactate dehydrogenase (LDH) levels increased concomitantly (Fig. 2). CT scan was performed, and revealed disease progression (Fig. 1D).
Fig. 1. Vitiligo re-pigmentation associated with melanoma progression during pembrolizumab treatment. (a) Extensive vitiligo in a patient treated with pembrolizumab for metastatic melanoma. (b) Axial CT section demonstrating stable disease with thoracic metastasis associated with extensive vitiligo. (c) Partial re-pigmentation of vitiligo after 16 infusions of pembrolizumab. (d) Axial CT section demonstrating disease progression with an increase in thoracic metastasis associated with vitiligo re-pigmentation.
Fig. 2. Kinetics of serum biomarkers over time. Lactate dehydrogenase (LDH) rate only seemed to decrease with vitiligo and disease control while rising at the time of vitiligo re-pigmentation and disease progression.
Vitiligo is one of the most frequent dermatologic adverse events of the anti-PD-1 therapy in cancer immuno-therapy (2). In a meta-analysis, the incidence of all-grade vitiligo was around 8% with immunotherapy (2). The incidence of vitiligo in melanoma patients, treated with pembrolizumab, has been reported to be up to 25% (4). As compared to patients under chemotherapy, vitiligo is reported to be more frequent in patients treated with nivolumab or pembrolizumab (2). In the literature, melanoma-associated vitiligo had a rather generalized distribution as in the present observation (4). However, time to vitiligo onset after the anti-PD-1 therapy is usually reported longer (ranged from 52 to 453 days (median, 126)) (4). Furthermore, the occurrence of vitiligo has been previously associated with prolonged overall and progression free survivals in immunotherapy-treated advanced melanoma patients (5–8).
Data on vitiligo re-pigmentation in patients with metastatic melanoma are scarce. To the best of our knowledge, this observation is the first report of vitiligo re-pigmentation associated with disease progression during treatment with pembrolizumab for metastatic melanoma.
The current observation showed a striking case of extensive vitiligo, associated with disease control, in a metastatic cancer patient with high tumour burden and vitiligo re-pigmentation, associated with tumour relapse. This suggests that vitiligo re-pigmentation might be a surrogate marker of disease progression or recurrence in case of a response to anti-PD-1 therapy.
This case is similar to one previously reported with nivolumab (9). This patient who received nivolumab for metastatic melanoma developed vitiligo spots along with tumour response. Eight months after treatment cessation, vitiligo re-pigmentation occurred and brain metastases were diagnosed on the CT scan.
The mechanism underlying tumour relapse and concomitant vitiligo re-pigmentation has not been studied. Two elements suggest an autoimmune mechanism. First, the same clone of CD8 T cells was found both in tumour cells and vitiligo lesions. Second, circulating antibodies against melanoma-associated antigens shared by melanoma cells and normal melanocytes are found in the setting of the PD-1 inhibitor-induced vitiligo (10, 11). Anti-PD-1 therapy activates the immune response by preventing an inhibitory signal and probably induces tumour response against antigens shared by melanomas and normal melanocytes. Thus, this immune response may lead to the occurrence of vitiligo (4). The mechanism occurring when patients develop resistance to the anti-PD-1 therapy may be similar in melanomas and normal melanocytes. One could hypothesize that tumour cells and normal melanocytes may overcome PD1 inhibition by down-regulating anti-melanocytic antibodies expression leading to vitiligo re-pigmentation and tumour re-lapse, as autoimmune T cells against melanocytes have been implicated in vitiligo induced by anti-PD-1. Finally, an increase in T regulatory cells (T-regs) in the skin is observed in the event of disease progression. This skin infiltration by T-regs might be associated with vitiligo re-pigmentation, as recently reported in mice (12, 13).
However, vitiligo re-pigmentation may be spontaneous or due to involuntary sun exposure (natural ultraviolet light exposure). The association of vitiligo re-pigmentation with melanoma progression may be coincidental and conclusion cannot be drawn from this case.
In conclusion, the occurrence of vitiligo may be a good surrogate marker for tumour response to the anti-PD-1 therapy in melanoma patients. Conversely, in case of vitiligo re-pigmentation, disease recurrence might be suspected and should be ruled out. However, conclusions cannot be drawn from this case report and further studies are necessary to assess if progression is correlated with vitiligo re-pigmentation in melanoma patients treated with anti-PD-1 antibodies.


 Click to show fullsize
Click to show fullsize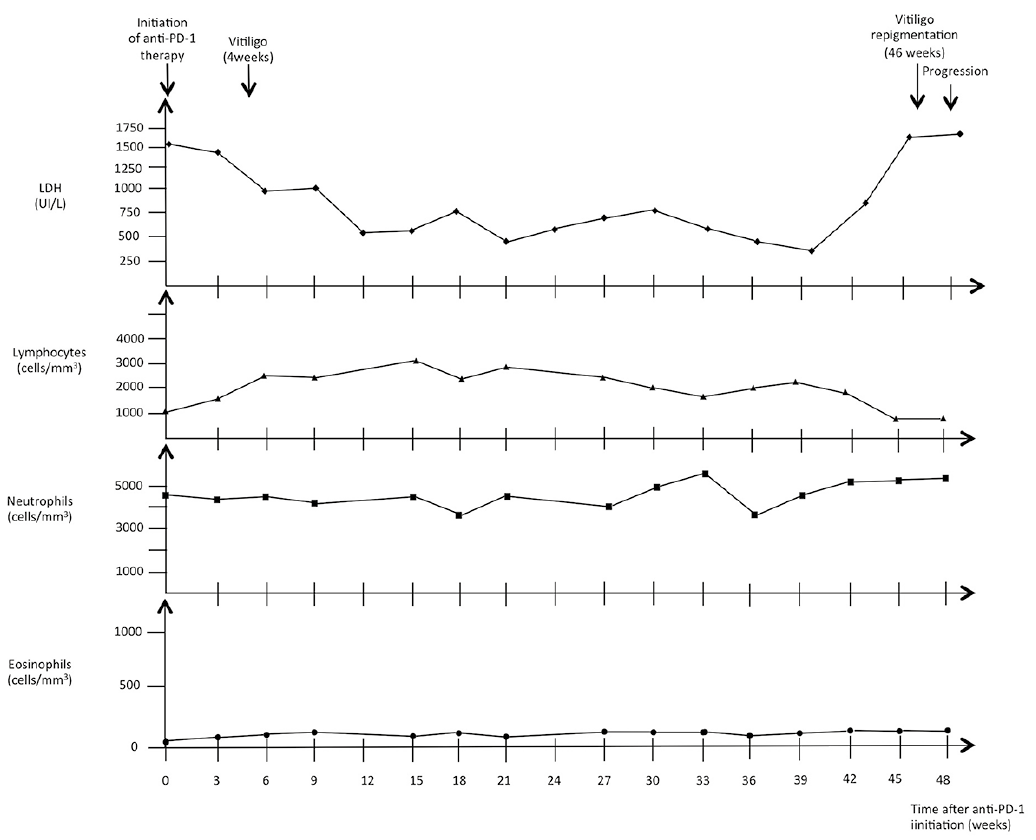 Click to show fullsize
Click to show fullsize