


1Division of Dermatology, Rabin Medical Center – Beilinson Hospital, Petach Tikva, and 2Sackler Faculty of Medicine, Tel Aviv University, Tel Aviv, Israel
Interleukin-17A inhibitors are a promising alternative to tumor necrosis factor-α inhibitors for the treatment of psoriasis. In-class switch has been hardly investigated for interleukin-17A inhibitors. We report the experience (2017–2018) of a tertiary medical center with interleukin-17A-inhibitor switch in patients with moderate-to-severe psoriasis. Patient-, disease- and outcome-related data were retrospectively collected from the electronic files of 25 patients switched to ixekizumab following secukinumab failure. Mean ± standard deviation patient age was 56.7 ± 12.2 years. Mean baseline Psoriasis Area and Severity Index was 25. Secukinumab was discontinued due to primary failure in 7 patients and secondary failure in 18. Ixekizumab was administered for 7.3 ± 2.8 months; 22 patients were still on ixekizumab at the end of the study. Mean ± standard deviation Psoriasis Area and Severity Index reduction from baseline at study end was 75.5 ± 20.0%. Patients with moderate-to-severe psoriasis seem to be amenable to treatment with ixekizumab following secukinumab failure. Further large multicenter studies are needed.
Key words: IL-17A-inhibitors; ixekizumab; secukinumab; moderate-to-severe psoriasis; drug survival; switch.
Accepted Apr 16, 2019; E-published Apr 16, 2019
Acta Derm Venereol
Corr: Lev Pavlovsky, MD PhD, Division of Dermatology, Rabin Medical Center – Beilinson Hospital, Petach Tikva 4941492, Israel. E-mail: levp@clalit.org.il
The limited arsenal of biologic treatments available for moderate-to-severe psoriasis may make IL-17A in-class switch (secukinumab-to-ixekizumab) necessary, following a primary or secondary failure. Patients with heavily pretreated moderate-to-severe psoriasis respond well to ixekizumab for a relatively long time. The number of previous lines of treatment may adversely affect ixekizumab efficacy.
Psoriasis is a chronic immune-mediated inflammatory skin disease that frequently requires life-long treatment. About 30% of psoriatic patients are considered to have a more severe disease (1). The development of tumor necrosis factor (TNF)-α inhibitors, including etanercept, adalimumab (2, 3), and anti-interleukin (IL)-12/23 ustekinumab (3), about 15 years ago, revolutionized the treatment of moderate-to-severe psoriasis. However, according to drug-survival studies, which measure the period of medication use until discontinuation, the effectiveness of all TNF-α inhibitors may be expected to decrease in the long-term (4).
IL-17A is a key cytokine in the pathogenesis of psoriasis (5). It may be selectively neutralized by secukinumab, a fully human monoclonal antibody. Secukinumab has shown considerable efficacy in the treatment of moderate-to-severe psoriasis and psoriatic arthritis, with a rapid onset of action, sustained responses, and favorable safety profile (5). However, although an extension of the original SCULPTURE study of dose regimens in psoriasis treatment reported sustained efficacy of secukinumab over 3 years of treatment (6), the findings were not always confirmed in a real-life setting. In a study of several biologic agents (adalimumab, etanercept, infliximab, ustekinumab, and secukinumab), secukinumab was associated with the lowest drug survival rate (7).
Sequential treatment with two TNF-α inhibitors has been investigated with encouraging results, albeit variable efficacy (8–14). However, data on IL-17A-inhibitor switching, from secukinumab to ixekizumab, are still preliminary and limited to the short term. Our literature search yielded 3 studies, summarizing 12 weeks of switch (15–17); a case series (n = 12) (15), a multicenter retrospective study of 17 patients (16), and a sequential study including additional 14 patients (17). In another recent multicenter retrospective real-life study of 100 psoriatic patients, treated with ixekizumab, 26 patients underwent a secukimumab-to-ixekizumab switch. Following 12–16 weeks of treatment, 20 patients (77%) achieved a 75% reduction in the Psoriasis and Severity Index (PASI) score (PASI 75) (18). The most recent results were provided by a study summarizing 24 weeks of switch of secukinumab to ixekizumab (19).
The two available IL-17A inhibitors, secukinumab and ixekizumab, were registered in Israel for the treatment of moderate-to-severe psoriasis in August 2015 and August 2017, respectively. The aim of the present study is to report an extended period, up to one-year experience of a tertiary medical center in Israel with IL-17A-inhibitor switch in patients with moderate-to-severe psoriasis.
According to the Israeli regulatory guidelines for the treatment of psoriasis, the sequential failure of 2 out of 4 medications (TNF-α inhibitors etanercept, adalimumab, or infliximab, or apremilast) is required before ustekinumab or an IL-17A-inhibitor can be approved (4) as the third line (at least) treatment. Both secukinumab and ixekizumab are administered as specified by the US Food and Drug Administration-approved label.
The present retrospective observational cohort study was conducted between August 1, 2017 and July 31, 2018. The cohort included patients with moderate-to-severe psoriasis attending a tertiary outpatient psoriasis clinic, which underwent secukinumab-to ixekizumab switch. Data were collected from the clinic’s electronic registry, in the manner previously described (20): demographic and baseline characteristics, presence of psoriatic arthritis, comorbidities, previous biologic treatments for psoriasis, baseline scales, assessing disease severity (body surface area (BSA), PASI), duration (in months) of secukinumab and ixekizumab treat-ment and reason for their discontinuation. Primary failure was defined as the inability to achieve PASI 50 within 3 months, and secondary failure, as the loss of an adequate response, requiring treatment discontinuation. To quantitatively evaluate treatment effectiveness, we measured the PASI response at the end of the study period (July 31, 2018). The duration of effective ongoing treatment was calculated from the date of treatment onset to the closest follow-up visit (usually within a month) before the end of the study period or a preset time point (12, 24, 48 weeks). In cases of treatment failure, drug survival was calculated, in months, from drug initiation to date of withdrawal.
The study was approved by the local Institutional Review Board, which waived the need for informed consent.
Continuous quantitative variables (age, body mass index, PASI, BSA, treatment duration) are presented as mean ± standard deviation (SD), median and interquartile range (IQR). Pearson correlation analysis was used to assess correlations between the numeric variables. A two-tailed p-value < 0.05 was considered to be statistically significant. The statistical analysis was conducted with SPSS ver. 21.
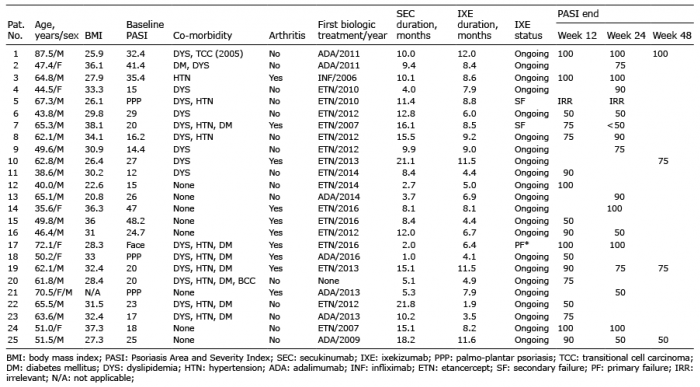
The cohort consisted of 25 patients, 18 men and 7 women, of mean ± SD age 56.8 ± 12.4 years (range 35.6–87.5 years, median 61.8). The characteristics of the individual patients are presented in Table I. Chronic plaque-type psoriasis was diagnosed in 22 patients, including 3 with severe involvement of the face, and mainly palmo-plantar psoriasis was diagnosed in 3 patients. Mean baseline PASI was 25.1 (range 12–48.2; median 23), and mean baseline BSA was 61% (n = 15; range 45–90%; median 60%). Mean ± SD BMI was 30.7 ± 4.5.
Table I. Characteristics of 25 patients with moderate-to-severe psoriasis
Secukinumab was initiated after a mean of 3.8 prior immunobiologic medications (range 3–6, median 4) failed. The most utilized first- and second-line immunobiologic drugs were etanercept (n = 16) and adalimumab (n = 7), and the most common third-line drug was ustekinumab (n = 17). The mean ± SD duration of biologic treatment prior to the initiation of secukinumab was 5.8 ± 2.9 years (range 2–12 years; median 6 years, IQR 3.5), and the mean ± SD duration of secukinumab treatment was 10.9 ± 5.9 months (median 10.2 months, IQR 7.9). Secukinumab was discontinued because of primary failure in 7 patients, after at least 3 months of treatment, and secondary loss of efficacy in 18 patients, after a mean of 10.6 ± 5.9 months of treatment (median 10.1 months, IQR 8.7). In no case were side effects the reason for secukinumab discontinuation.
All study participants, except one, were switched to ixekizumab after secukinumab failure without an intervening biologic treatment; in one patient (patient 20, Table I), ixekizumab was started after a single dose of ustekinumab. The overall mean ± SD duration of ixekizumab treatment was 7.3 ± 2.8 months (range 1.9–12 months, median 7.9, IQR 4.2). At the end of the study surveillance period (July 31, 2018), 22 of the 25 patients were still receiving ixekizumab, for a mean ± SD duration of 7.4 ± 2.8 months (median 7.9 months, IQR 4.2); 4 patients were receiving the drug for at least 48 weeks. Ixekizumab was discontinued in one patient due to the exacerbation of psoriatic arthritis, and in 2 patients, because of loss of efficacy after 8.5 and 8.8 months, respectively. The mean ± SD reduction in PASI score at the end of the surveillance period was 75.5 ± 20.0 (range 50–100; median 75); 15 patients (68%) achieved PASI 75 or higher, 9 (41%) achieved PASI 90 or higher, and 5 (23%) PASI 100. Fig. 1 depicts the distribution of the patients by response to treatment. Table I elaborates the PASI data for the patients with a documented visit at preset time points after switching. Among 17 patients evaluated at 12 weeks, 13 (76%) achieved PASI 75; 9 (53%) PASI 90; and 5 (29%) PASI 100; mean ± SD PASI reduction was 80 ± 19.5 (median 90). Among 15 patients evaluated at 24 weeks, 11 (73%) achieved PASI 75; 8 (53%) PASI 90; and 5 (33%) PASI 100; mean ± SD PASI reduction was 79.7 ± 20.7 (median 90). Among 4 patients evaluated at 48 weeks, 3 (75%) achieved PASI 75; 1 (25%) PASI 90, and 1 (25%) PASI 100; mean ± SD PASI reduction was 75 ± 20.4 (median 75). Loss or decrease in efficacy was noticeable shortly after the end of the loading period (12 weeks) in 4 patients (Table I, patients 7, 16, 19, 25). There was a positive correlation between the number of previous failed biologic treatments and ixekizumab survival to the end of the surveillance period (Pearson r = 0.557, p = 0.007). There was no correlation between baseline PASI, BSA, psoriatic arthritis, or patient age and ixekizumab efficacy or survival. In the patient with primary failure of ixekizumab (patient 17), ixekinumab was discontinued due to the exacerbation of psoriatic arthritis, not the skin condition. The two patients with secondary failure of ixekizumab had an overall moderate PASI but significant involvement of sensitive areas: patient 5 had palmo-plantar psoriasis, and patient 7 had a PASI of 20 (lower by 20% than the mean PASI) and has had a previous primary failure of secukinumab treatment.
Fig. 1. Distribution of 25 patients with moderate-to-severe psoriasis by response to ixekizumab following failure of secukinumab. SEC: secukinumab; IXE: ixekizumab. *failure due to psoriatic arthritis, not cutaneous psoriasis.
Switching between biologic therapies in patients with psoriasis is a well-accepted dermatologic practice, with a reported rate of 17% in a national sample of Medicare beneficiaries, followed for 12 months (21). It has been found to improve both disease management and patient outcomes (8). Experience in in-class switching was initially gained with TNF-α inhibitors (mostly etanercept-to-adalimumab). Most trials reported beneficial results with variable efficacy (8–14), although they differed in population size, follow-up period, and study design. One study reported psoriasis flare in 4 patients after switching (22).
Since the publication of these studies, the therapeutic armamentarium of psoriasis has been expanded to include two biologic drugs (secukinumab, ixekizumab) targeting IL-17A, a key cytokine in the pathogenesis of the disease. Phase III trials showed greater efficacy of IL-17A inhibitors than anti-TNF-α inhibitors (23) and ustekinumab (24). The benefit of a secukinumab-to-ixekizumab switch has been investigated in only a few studies to date, with good results (15–19). The latest multicenter study from Italy included 69 patients of whom 56 achieved PASI 75 at 12 weeks, and 40 at 24 weeks (19). The number of previous lines of treatment was not mentioned. In a sequential retrospective study of 31 patients, 22 (71.0%) achieved PASI 75 or a Physician Global Assessment score of 0/1 at 12 weeks (17). Recently, Deza et al. (18) conducted a real-life study of the efficacy and safety of ixekizumab over a one-year observation period. A switch from secukinumab for a short term was reported in 26 patients (12–16 weeks). The overall mean number of previous biologic treatment failures was 2.6; 77% of patients achieved PASI 75 (18). In our cohort, a mean of 4.8 immunobiologic agents were administered prior to ixekizumab and 68% of patients achieved a PASI 75 response.
The present study is the first to investigate drug switch from secukinumab to ixekizumab in psoriatic patients, heavily pretreated with biologic agents for an extended period (up to one year). The rationale for switching, apart from the scarcity of available treatments, is based on a meta-analysis indirectly comparing secukinumab and ixekizumab wherein ixekizumab treatment was associated with higher PASI scores (PASI 90, PASI 100) than secukinumab treatment at 12 weeks (25). Accordingly, we found that 22 of 25 patients who had previously failed secukinumab were still on ixekizumab by the end of the study period, with a mean reduction in PASI of 75.5% (median PASI 75). However, our rates of PASI 75 and PASI 90 were lower than reported in clinical trials (68% versus 89% and 41% versus 77%, respectively) (26). On the Pearson correlation analysis, the number of previous lines of treatment correlated positively (r = 0.56, p = 0.007) with the duration of ixekizumab treatment but not with the efficacy of treatment. This finding is not surprising, since the lack of alternative options for patients given the newest available treatment may drive treatment persistence (21).
It is noteworthy that Georgakopoulos et al. (17), using a multicenter retrospective design, also observed a smaller reduction in PASI compared to previous randomized controlled trials of IL-17A-naïve patients (71% vs 87.3–89.7%). They suggested that the difference might be attributable to the number of previous biologic treatments (mean 3.6) and not merely the switch between the IL-17A antagonists.
We adhere to the suggestion of Conti et al. (19) that the higher immunogenicity of ixekizumab, a humanized antibody, may account for its effectiveness even after the failure of secukinumab, a fully human antibody belonging to the same class. Another potential explanation for the effectiveness of rescue treatment may be the different epitopes targeted by these medications.
Our study was limited by its retrospective nature, which may explain why we had no documentation for the regular follow-up visits every 12 weeks for some of the patients. Furthermore, owing to the relatively small sample size, the study may have been underpowered to achieve statistical significance for some of the correlations.
This study summarizes our extended (up to one year) single-center experience with IL-17A inhibitor switching, from secukinumab to ixekizumab, in patients with psoriasis. Ixekizumab treatment failed in only a minority of patients during the surveillance period despite the similar mechanism of action to secukinumab. We believe that patients with moderate-to-severe psoriasis are amenable to treatment with ixekizumab following secukinumab failure. Larger multicenter studies are needed to corroborate our findings.
Conflicts of interest: LP has served as an investigator for Abbvie, Coherus, Novartis, Janssen Biotech, and as an adviser, consultant and/or invited lecturer for Abbvie, Janssen Biotech, Novartis Pharmaceuticals Corporation, PfizerInc, Dexcell Pharma, Eli Lilly. SS, ESC, IAL, EH have no conflict of interest to declare.
IRB approval status: The study was conducted in accordance with the principles of the Declaration of Helsinki and approved by the Institutional Review Board. Informed consent was waived owing to the retrospective study design.


 Click to show fullsize
Click to show fullsize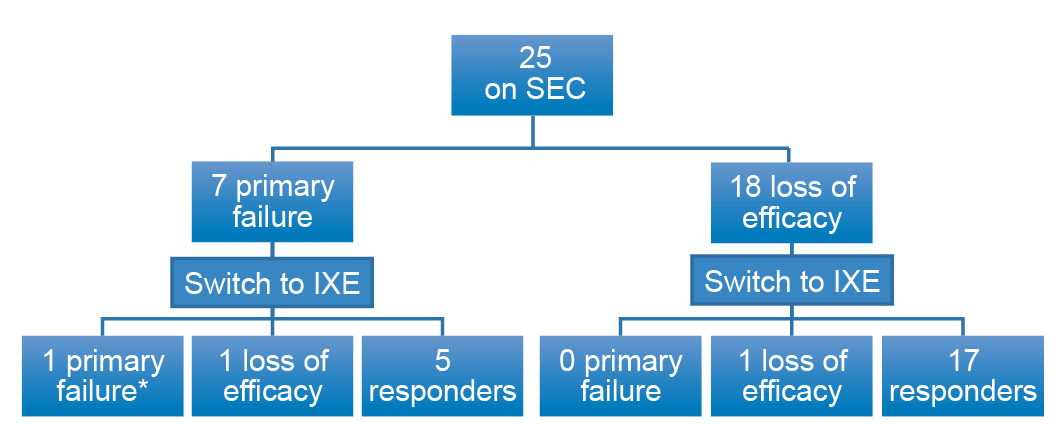 Click to show fullsize
Click to show fullsize