


1Noguchi Dermatology Clinic, 1834-1 Namazu, Kashima-machi, Kamimashiki-gun, Kumamoto 861-3101, 2Ochanomizu Institute for Medical Mycology and Allergology, Tokyo, 3Department of Dermatology, Juntendo University Urayasu Hospital, 4Division of Bio-resources, Medical Mycology Research Center, Chiba University, Chiba, and 5Department of Dermatology and Plastic Surgery, Faculty of Life Sciences, Kumamoto University, Kumamoto, Japan. E-mail: derma@nogcli.jp
Accepted Apr 29, 2019; E-published Apr 29, 2019
The term “Intertrigo” refers simple intertrigo, bacterial intertrigo, candidal intertrigo, interdigital tinea pedis, and intertrigo complicated with erythrasma (1). Interdigital fungal intertrigo is most caused by dermatophytes. In Senegal, Fusarium species are the second most frequently isolated fungi after Candida albicans (2). Human-pathogenic members of the genus Fusarium primarily belong to 8 species complexes, of which the Fusarium solani species complex (FSSC) and F. oxysporum species complex account for 60% and 20% (3). Hyalohyphomycosis and phaeohyphomycosis were umbrella terms to cover a growing number of opportunistic mycoses caused by moulds and yeasts whose septate mycelial tissue forms were either hyaline (Gr.’huálinos’), or phaeoid (Gr. ‘phaios’), respectively (4). Here, we provide the first report of interdigital hyalohyphomycosis caused by a member of the FSSC in Japan.
Case 1. A 58-year-old, female homemaker with a > 2-year history of an interdigital lesion visited our clinic in February 2017. She presented with maceration, erosion, scales, and itching in the left 3rd interdigital area (Fig. 1a). Direct microscopy revealed irregularly distorted septate hyphae (diameter 3–8 µm) and intercalary and terminal chlamydoconidia (Fig. 1b). Neither Candida species nor dermatophytes were isolated. Periodic acid-Schiff (PAS)-stained tissue showed septate hyphae. Hematoxylin and eosin (H&E) staining revealed basophilic hyphae (Fig. 1c). Plate culture on Sabouraud’s dextrose agar yielded a white felt-like colony with pale-yellow colored reverse after 7-day incubation at 25°C (Fig. 1d). Slide culture on potato dextrose agar yielded abundant unicellular oval microconidia and septate crescent macroconidia from verticillate conidiophores after 4-day incubation at 25°C. The internal transcribed spacer 1 (ITS-1) region of the rRNA gene and the translation elongation factor 1 alpha (EF-1α) gene sequences showed 100% (206/206 bp) and 100% (702/702 bp) homologies, with Fusarium petroliphilum type strain NF 4475 (NRRL 22268 = FRC S-2176) (5) (Mycobank no. MB802539). Based on its morphological characteristics and the gene analysis results, we identified the isolate as F. petroliphilum (Q.T. Chen & X.H. Fu) Geiser, O’Donnell, D.P.G. Short & N. Zhang, which belongs to the FSSC. The patient was diagnosed with interdigital hyalohyphomycosis. Antifungal susceptibility testing was performed according to the Clinical and Laboratory Standards Institute (CLSI) M38-A2 protocol (6). The minimum inhibitory concentrations (MICs) for the isolate were: amorolfine, 2 μg/ml; amphotericin B, 2 μg/ml; efinaconazole, 2 μg/ml; itraconazole, > 16 μg/ml; ketoconazole, > 16 μg/ml; terbinafine, > 16 μg/ml; and voriconazole, 8 μg/ml. Routine test results were within the normal ranges. The patient was treated with 2% ketoconazole cream and her symptoms disappeared in 4 months. The follow-up culture was negative and she showed no recurrence, as of December 2018.
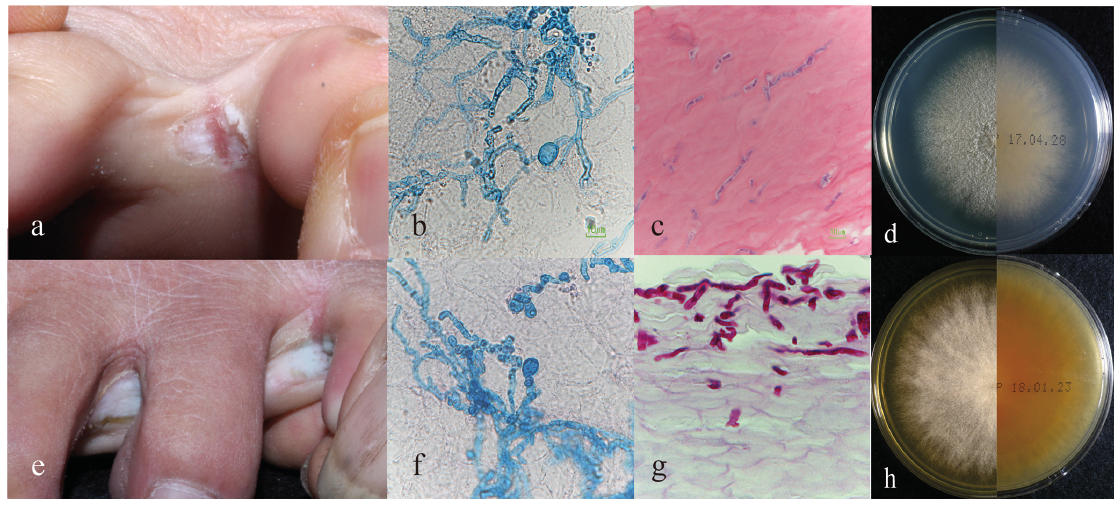
Fig. 1 (a) Case 1: Maceration, erosion, and scales on the left 3rd interdigital area. (b) Septate hyphae and intercalary chlamydoconidia (potassium hydroxide (KOH) with Parker ink, original magnification ×400). (c) Basophilic septate hyphae (hematoxylin and eosin stain, ×400). (d) Plate culture of Fusarium petroliphilum, a white felt-like colony with pale-yellow-coloured reverse. (e) Case 2: Maceration and desquamation on the left 3rd and 4th interdigital area. (f) Septate hyphae and intercalary chlamydoconidia (Parker ink-KOH, ×400). (g) Septate hyphae in the upper stratum corneum (Periodic acid-Schiff-stain, ×400). (h) Plate culture of Fusarium keratoplasticum, a white floccose colony with brown-coloured reverse.
Case 2. An 81-year-old, male farmer had noticed an interdigital lesion in 2014. He applied 1% lanoconazole cream, which had no effect. In March 2017, maceration and desquamation in the 3rd and 4th interdigital lesions were observed (Fig. 1e). Direct microscopy revealed septate hyphae and chlamydoconidia (Fig. 1f). PAS and H&E-stained tissue also showed septate hyphae (Fig. 1g). Plate culture on Sabouraud’s dextrose agar yielded a white floccose colony with brown-coloured reverse after 14-day incubation at 25°C (Fig. 1h). Slide culture on potato dextrose agar showed unicellular microconidia and 2- to 4-celled crescent macroconidia after 7-day incubation at 25°C. The ITS-1 region of the rRNA gene and EF-1α gene sequences showed 100% (207/207 bp) and 100% (696/696 bp) homologies, to F. keratoplasticum type strain (CBS 490.63=NRRL 22661) (5) (Mycobank no. 802390). We identified the isolate as F. keratoplasticum D. Geiser, O’Donnell, Short & Ning Zhang, which belongs to the FSSC. The MICs for the isolate were: amorolfine, > 16 μg/ml; amphotericin B, 2 μg/ml; efinaconazole, 4 μg/ml; itraconazole, > 16 μg/ml; ketoconazole, > 16 μg/ml; terbinafine, > 16 μg/ml; and voriconazole, 8 μg/ml (6). Routine test results were in the normal range. Topical ketoconazole was applied for 3 months, but no improvement was seen. Owing to the presence of tinea unguium caused by Trichophyton rubrum in the right first toenail, oral terbinafine was administered for 6 months, which helped to resolve this condition. However, the interdigital lesion did not change. A 3-month treatment with 10% efinaconazole solution was started in December 2017. The patient was cured, and showed no recurrence after a period of one year and a half.
Interdigital lesion caused by Fusarium species precisely coincide with the definition of hyalohyphomycosis. The FSSC includes over 60 species distributed worldwide belonging the genus Fusarium, family Nectriaceae, order Hypocreales, class Sordariomycetes, phylum Ascomycota, and kingdom Fungi (7). Member of FSSC, including F. petroliphilum, F. keratoplasticum, and F. falciforme, are common in soil and causative agents of plants, shrimp, and human (7). In Japan, they account for 72.6% (53/73) of the Fusarium species isolated from humans (8). Fusarium falciforme occasionally causes keratomycosis. Fusarium petroliphilum and F. keratoplasticum are found in environments and cause invasive pulmonary infection or sinusitis in immunocompromised patients, which may disseminate to other organs and causes sepsis (7, 8). FSSC members degrade keratin, with lower ability than dermato-phytes (9), and cause superficial cutaneous inflammation (10).
The diagnosis of interdigital hyalohyphomycosis requires as the same of non-dermatophyte onychomycosis described by Gupta et al. (11). Although our cases were skin not nail infection, they satisfied the criteria.
Interdigital hyalohyphomycosis caused by Fusarium species has been reported in 12 patients, including our two cases, 6 cases from Senegal (12, 13) and one case each from Italy (13), Brazil, India, and Iran; these 12 cases involved 7 men and 5 women with a mean age of 41.2 years. Of the 6 patients in Senegal, 4 lived barefoot. None of the patients had significant underlying diseases. Seven patients had a disease duration of ≥2 years. The affected sites included the 3rd, 4th, and both 3rd and 4th interdigital areas in 9, 8, and 7 of 10 patients, respectively. Fusarium solani and F. oxysporum were the causative organisms in 6 and 5 patients, respectively. Data on treatment were available for 8 patients; terbinafine 250 mg/day or itraconazole 200 mg/day was administered orally for 6–24 weeks, after which one patient was cured but 3 did not, and 6 showed recurrence 6–10 months after treatment termination. Ketoconazole was effective in Case 1; however, follow-up is necessary because of a dissociation between clinical efficacy and MIC values. Case 2 was treated with efinaconazole, a topical antifungal medicine developed for the treatment of onychomycosis. The MIC of efinaconazole against FSSC member is lower than that of terbinafine and itraconazole (14). Clinical symptoms are not reliable for distinguishing hyalohyphomycosis caused by FSSC members from interdigital tinea pedis or interdigital candidiasis; thus culture or molecular diagnostic confirmation is indispensable. Interdigital hyalohyphomycosis is one of the recalcitrant interdigital conditions.
This research was partially supported by the Japan Agency for Medical Research and Development (AMED) under grant number JP19fk0108094.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize