


Department of Dermatology, Kyoto University Graduate School of Medicine, 54 Shogoin Kawahara-cho, Sakyo, Kyoto 606-8507, Japan. E-mail: dainichi@kuhp.kyoto-u.ac.jp
A 60-year-old woman with no medical history or current medications presented with scaly red papules on her extremities. The patient had visited several dermatology clinics and had been treated with topical corticosteroids, phototherapy, and oral retinoids. None of these treatments had resolved the skin eruptions. She developed generalized erythroderma 8 months after onset of the condition and was referred to our hospital for further evaluation and treatment.
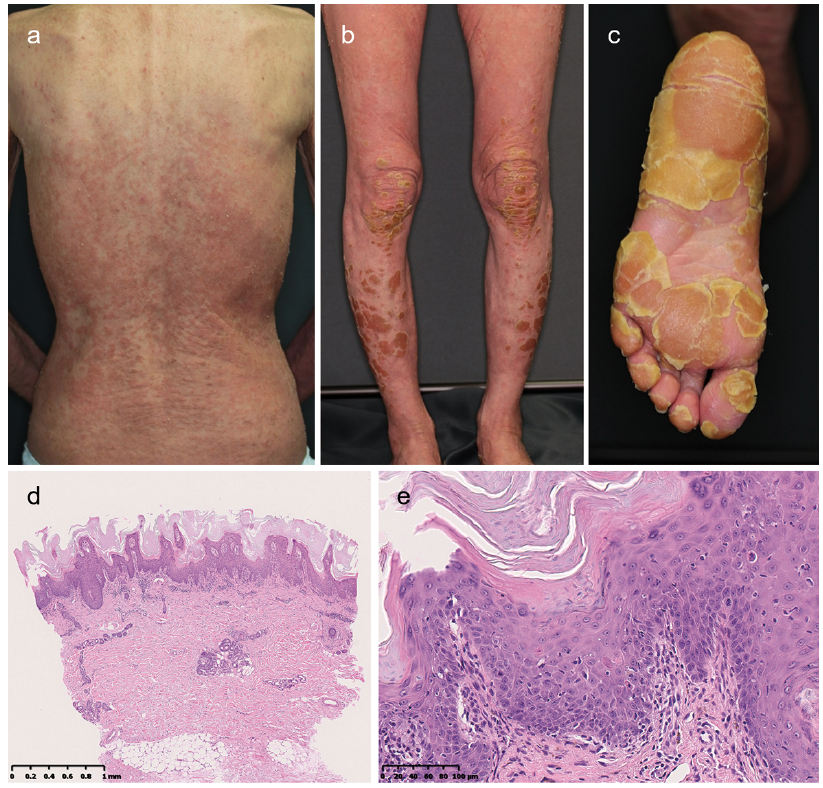
The patient exhibited confluent erythema affecting the face, trunk, and extremities with severe pruritus (Fig. 1a, b). She had hyperkeratosis on the lower extremities, especially on the soles of the feet (Fig. 1b, c). She did not report any other somatic symptoms. Laboratory analysis showed mild elevation in serum levels of liver enzymes and hypogammaglobulinaemia. Histological findings of the skin biopsy specimen revealed parakeratosis, marked papillomatous acanthosis, necrotic keratinocytes in the epidermis, and interface vacuolar changes with lymphocytic infiltration in the superficial dermis (Fig. 1d, e).
What is your diagnosis? See next page for answer.
Fig. 1. (a, b) Confluent elevated erythema with scaling on the back and lower legs. Hyperkeratosis scattered on the lower legs. (c) More severe hyperkeratosis on the soles. (d) Haematoxylin and eosin staining revealed parakeratosis and papillomatous acanthosis. (e) A number of necrotic keratinocytes were present in the epidermis, vacuolar changes and lymphocytic infiltration in the superficial dermis.
Acta Derm Venereol 2019; XX: XX–XX.
Diagnosis: Thymoma-associated multiorgan autoimmunity
A screening X-ray of the chest revealed a mass in the mediastinum, and computed tomography scan revealed an 11 × 9.5 × 7 cm-sized tumour in the anterior mediastinum (Fig. 2). A needle biopsy from the tumour in the anterior mediastinum indicated thymoma. These therefore confirmed the diagnosis of thymoma-associated multiorgan autoimmunity (TAMA), which is consistent with the skin symptoms, as well as the liver injury and hypogammaglobulinaemia detected by laboratory tests. The patient also had a positive anti-acetylcholine receptor antibody titre, which was also considered to be related to thymoma, without muscle weakness. The patient received total thymectomy (confirmed as WHO type AB, Masaoka stage IIa). Approximately 2 weeks after surgery, the patient developed muscle weakness and was diagnosed with myasthenic crisis. Intravenous immunoglobulin followed by oral prednisolone and tacrolimus was effective, and the skin lesions also improved.
Fig. 2. A computed tomography scan of the chest revealed a solid mass in the anterior mediastinum.
Thymoma patients can develop various autoimmune diseases, such as myasthenia gravis, pure red cell aplasia, and acquired hypogammaglobulinaemia. TAMA, firstly described as graft-versus-host disease (GVHD)-like colitis, is currently defined as the rare disorder that leads to the development of GVHD-like symptoms, such as liver dysfunction, gastrointestinal symptoms, and skin manifestations, in the setting of thymoma (1). Although the mechanism of TAMA remains unknown, the disordered thymic education with defective expression of autoimmune regulator (AIRE) in thymoma and decrease in regulatory T cells might be involved (2). Thymoma originates from thymic epithelial cells, which provide an environment for the thymic education of T cells. The negative selection of self-reactive T cells largely depends on the expression of AIRE, which controls the ectopic expression of a wide range of peripheral organ-specific genes by medullary thymic epithelial cells.
The diagnosis of TAMA is based on clinical signs, results of histopathological findings, and detection of thymoma. Cutaneous manifestations of TAMA are described as keratotic papules, scaly plaques, morbilliform eruptions, psoriasiform lesions, or erythroderma (3–5). In histopathology, TAMA is characterized by interface and perivascular dermatitis with necrotic keratinocytes throughout the epidermis (6). Imaging of the chest is indispensable for the diagnosis of TAMA. An X-ray of the chest is usually sufficient to detect thymoma and computed tomography imaging of the chest can provide definitive information for the diagnosis.
As a clinical problem, clinicopathological skin manifestations of TAMA may be difficult to distinguish from those of other types of dermatitis with histological interface changes and necrotic keratinocytes without radiological imaging tests. Indeed, in our case, we considered the following skin diseases in the differential diagnoses: pityriasis lichenoides chronica (PLC), dermatomyositis (DM) and pityriasis rubra pilaris (PRP). The current case presented with scaly papules in the early phase and had been misdiagnosed clinically and histologically with PLC. We excluded a diagnosis of PLC because it does not develop erythroderma. DM, particularly associated with cancer, may show similar histopathological findings and has the potential to cause erythroderma, but we did not find any other specific skin manifestations of DM, such as heliotrope rash, Gottron’s papules, or mechanic’s hands, nor did we detect specific autoantibodies related to DM in the present case. Evaluation of the lungs is important, because interstitial lung disease can be a highly progressive and lethal complication, particularly in amyopathic dermatomyositis, which should be ruled out in the current case. PRP was also considered as a differential diagnosis for clinical cutaneous manifestations in the current case, but the biopsy specimen did not present histopathological findings specific for PRP.
Treatments for TAMA have not yet been established: surgical resection, chemotherapies, and radiotherapies for thymoma, and immunosuppressive therapies and photo-therapies for the skin have previously been reported (3, 5, 7–9). Despite these treatments, however, patients have a progressive course with fatal outcome in some cases (3, 10, 11).
Physicians should consider the accompanying neoplasms when presented with a patient with progressive erythroderma. Imaging tests may provide crucial information in the cases where clinicopathological findings cannot result in a definitive diagnosis.


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize