


1Department of Dermatology, University of Tokyo Graduate School of Medicine, Tokyo, and 2Department of Dermatology, International University of Health and Welfare, Chiba, Japan
Tumor cells in cutaneous T-cell lymphoma express limited numbers of chemokine receptors. We investigated the expression patterns of CXCR3, CCR3, CCR4 and CCR10 in mycosis fungoides, Sézary syndrome, lympho-matoid papulosis and anaplastic large cell lymphoma in 121 skin biopsy samples. CXCR3 was expressed in 86% of mycosis fungoides cases but in no anaplastic large cell lymphoma cases. CCR3 was expressed in 73% of cases of CD30+ lymphoproliferative disorders such as lymphomatoid papulosis and anaplastic large cell lymphoma. Mycosis fungoides/Sézary syndrome patients with high CCR3 or CCR4 expression had a poorer survival prognosis than mycosis fungoides/Sézary syndrome patients whose tumor cells did not express these receptors. CCR10 was expressed in 50% of mycosis fungoides/Sézary syndrome cases and in 13% of cases with CD30+ lymphoproliferative disorders. These results suggest that differential patterns of CXCR3, CCR3, CCR4 and CCR10 expression are useful for the diagnosis of cutaneous T-cell lymphoma. Moreover, expression of CCR3 or CCR4 suggests a poor prognosis in mycosis fungoides/Sézary syndrome.
Key words: CTCL; CXCR3; CCR3; CCR4; CCR10.
Accepted Apr 30, 2019; E-published May 2, 2019
Acta Derm Venereol
Corr: Hiraku Suga, M.D., Ph.D., Department of Dermatology, University of Tokyo Graduate School of Medicine, 7-3-1 Hongo, Bunkyo-ku, Tokyo 113-8655, Japan. E-mail: sugah-der@h.u-tokyo.ac.jp
Cutaneous T-cell lymphomas are a heterogeneous group of extranodal non-Hodgkin’s lymphomas that are characterized by a cutaneous infiltration of malignant monoclonal T lymphocytes. Tumor cells in cutaneous T-cell lymphoma express limited numbers of chemokine receptors on their cell surface. We analyzed the expression patterns of CXCR3, CCR3, CCR4 and CCR10 in skin samples from patients with cutaneous T-cell lymphoma. In addition, we investigated the relationship between chemokine receptor expression and survival prognosis. Differential patterns of CXCR3, CCR3, CCR4 and CCR10 expression were useful for the diagnosis of cutaneous T cell lymphoma. Moreover, expression of CCR3 or CCR4 suggested a poor prognosis in cutaneous T-cell lymphoma.
Tumor cells in cutaneous T cell lymphoma (CTCL) express limited numbers of chemokine receptors. CXCR3, a receptor for CXCL9, CXCL10 and CXCL11, is mainly expressed on Th1 cells and natural killer cells (1). CXCR3 has been reported to be expressed by epidermotropic T cells in mycosis fungoides (MF) (2). CCR3, which binds to CCL5, CCL7, CCL11, CCL13 and CCL26, is mainly expressed on eosinophils and subpopulations of Th2 cells (3), and CCR3 expression by atypical lymphoid cells has been related to anaplastic large cell lymphoma (ALCL) (4). CCR4 is a receptor for CCL17 and CCL22. CCL17 is expressed by dendritic cells and endothelial cells in lesional skin of patients with MF and Sézary syndrome (SS) (5), suggesting important roles of the CCL17-CCR4 interaction in the disease progression of MF/SS. CCL27 and CCL28, ligands for CCR10, are associated with the homing of memory T lymphocytes to the skin (6). Keratinocytes express CCL27, which is accompanied by CCR10-positive tumor cell infiltration in lesional skin of patients with MF (7). In this study, we analyzed the patterns of CXCR3, CCR3, CCR4 and CCR10 expression in MF, SS, CD30+ lymphoproliferative disorders (LPDs) such as lymphomatoid papulosis (LyP) and ALCL and atopic dermatitis (AD). In addition, we investigated the relationship between chemokine receptor expression and survival prognosis in MF/SS.
One hundred and twenty-one biopsy specimens were collected in our department from January 2008 to August 2018. Skin samples from cases of MF (n = 76), SS (n = 12), LyP (n = 10), ALCL (n = 5) and AD (n = 18) were used for immunohistochemistry. The samples enrolled in a previous report were also analyzed in this research (8). The medical ethical committee of the University of Tokyo approved all described studies, and the study was conducted according to the principles of the Declaration of Helsinki.
Fresh-frozen skin samples were used for immunohistochemistry. We used the following antibodies as primary antibodies: a mouse monoclonal antibody directed against CXCR3 (1C6, BD Biosciences Pharmingen, Heidelberg, Germany), a rabbit antibody against CCR3 (MBL International, Woburn, MA, USA), a mouse monoclonal antibody directed against CCR4 (1G1, BD Biosciences Pharmingen) and a goat antibody against CCR10 (Capralogics, Hardwick, MA, USA). The following antibodies were used as secondary ones: a biotinylated horse anti-mouse IgG antibody (Vector Laboratories, Burlingame, CA, USA) for CXCR3 and CCR4, a biotinylated goat anti-rabbit IgG antibody (Vector Laboratories) for CCR3 and a biotinylated rabbit anti-goat IgG antibody (Vector Laboratories) for CCR10. We classified the immunostaining intensity into 3 categories: negative (–), weakly positive (+) and strongly positive (++). Samples in which more than half of the infiltrating cells were positive for a chemokine receptor were considered strongly positive for that receptor. Four doctors evaluated the staining blinded to the clinical diagnosis.
Statistical analysis was performed using the χ2 test. p-values < 0.05 were considered statistically significant. Survival analysis was performed using the Kaplan-Meier method.
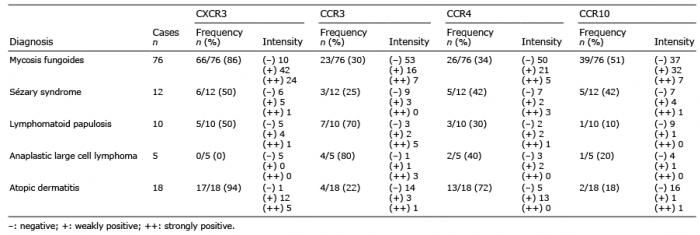
A summary of chemokine receptor expression is shown in Table I and Fig. 1. CXCR3 expression was detected in 86% of MF cases and 94% of AD cases but in no ALCL cases (Table I). The frequency of CXCR3 expression was significantly different between ALCL cases and both MF (p < 0.01) and AD (p < 0.01) cases. In MF and AD cases, the majority of infiltrating lymphocytes were positive for CXCR3; by contrast, in ALCL cases, no tumor cells were positive for CXCR3 (Fig. 1A). In MF cases, epidermal lymphocytes that formed a Pautrier’s microabscess were positive for CXCR3 (Fig. 1A). CCR3 expression was positive in more than 70% of LyP and ALCL cases but in less than 30% of MF, SS and AD cases (Table I). The frequency of CCR3 expression was significantly different between CD30+ LPD cases and MF (p < 0.01), SS (p < 0.05), and AD (p < 0.01) cases. The immunostaining intensity indicating the CCR3 expression level was highest in LyP cases, followed by ALCL cases (Fig. 1B). The frequency of CCR4-positive cases was nearly equal in MF, SS, LyP and ALCL cases, ranging from 30–42%, significantly lower than that in AD cases (72%, p < 0.05; Table I). Regarding immunostaining intensity, 4 MF cases and 3 SS cases were strongly positive for CCR4; however, CCR4 expression was weak in all CCR4-positive AD cases. The immunostaining intensity of CCR10 expression was higher in MF/SS cases than in LyP, ALCL or AD cases (Fig. 1D and Table I). CCR10 expression was detected in 50% of MF/SS cases, a significantly higher percentage than that of CD30+ LPD (13%, p < 0.05) and AD (11%, p < 0.01) cases. Thus, CXCR3 expression was associated with MF, while CCR3 expression was related to CD30+ LPDs such as LyP and ALCL. In addition, MF/SS was more frequently accompanied by CCR10 expression.
Table I. Summary of CXCR3, CCR3, CCR4 and CCR10 expression in mycosis fungoides (MF), Sézary syndrome (SS), lymphomatoid papulosis (LyP), anaplastic large cell lymphoma (ALCL) and atopic dermatitis (AD)
Fig. 1. Immunohistochemical staining for (A) CXCR3, (B) CCR3, (C) CCR4 and (D) CCR10. (A) Infiltrating cells expressed CXCR3 in MF, SS, LyP and AD. (B) Infiltrating cells expressed CCR3 in LyP and ALCL. Strong CCR3 expression was seen in MF cases with poor prognosis. (C) Infiltrating cells expressed CCR4 in AD. (D) CCR10-positive cells infiltrated in MF and SS. Bars = 50 µm.
Next, we classified the MF/SS cases into the following 3 groups according to chemokine receptor expression: negative (–), weakly positive (+) and strongly positive (++). Then, we analyzed the survival prognosis among the 3 groups (Fig. 2). As assessed by a log-rank test, patients strongly positive for CCR3 expression had a significantly lower survival rate than CCR3-negative patients (hazard ratio (HR) 8.084, 95% confidence interval (CI) 0.7483–87.35, p < 0.0001) or patients weakly positive for CCR3 expression (HR 12.75, 95% CI 1.232–132, p < 0.0001; Fig. 2). Similarly, MF/SS patients strongly positive for CCR4 expression exhibited a significantly lower survival rate than CCR4-negative patients (HR 3.397, 95% CI 0.7526–15.34, p = 0.0191) or patients weakly positive for CCR4 expression (HR 4.014, 95% CI =0.8762–18.39, p = 0.0379; Fig. 2).
Fig. 2. Kaplan-Meier survival curve of MF/SS patients according to CXCR3, CCR3, CCR4 and CCR10 expression. Negative (–), weakly positive (+) and strongly positive (++) groups.
The frequencies of CCR3-negative, weakly positive and strongly positive staining were 70%, 22% and 8%, respectively, in patients with MF in the early patch and plaque stage and 66%, 23% and 11%, respectively, in patients with advanced-stage MF/SS; these frequencies were not significantly different. For CCR4, the frequencies of negative, weakly positive and strongly positive staining were 68%, 29% and 3% in patients with early-stage MF, respectively, and 62%, 15% and 23%, respectively, in patients with advanced MF/SS, indicating that strong CCR4 expression was observed in advanced MF/SS rather than in early MF. Moreover, we investigated the correlation between CTCL disease markers and CCR3/CCR4 expression. The serum levels of soluble interleukin-2 receptor, lactate dehydrogenase, IgE and CCL17, which are disease markers of CTCL (9–11), were not significantly different among the groups with negative, weakly positive and strongly positive CCR3/CCR4 expression (data not shown). Taken together, these results indicate that higher expression of CCR3 and CCR4 is associated with a poorer prognosis in MF/SS.
Previously, we investigated the expression patterns of CXCR3, CCR3 and CCR10 in CTCL and cutaneous inflammatory diseases by using 43 skin samples (8). In this study, we increased the number of samples to 121 and reanalyzed the expression patterns of chemokine receptors and further assessed survival prognosis.
CXCR3 was expressed in 86% of MF cases. CXCL9 and CXCL10, ligands for CXCR3, were expressed in the epidermis of MF lesions, suggesting that CXCR3-CXCL9/CXCL10 interactions are associated with marked epidermotropism (2, 12). However, most tumor cells in MF and SS samples were negative for CCR3 expression, consistent with previous reports (13, 14). In contrast, CCR3 was expressed in 73% of CD30+ LPD cases, suggesting that CCR3 may be a key marker for CD30+ LPDs. Large transformed tumor cells often express CD30 in advanced MF/SS. Interestingly, in some cases of MF with large cell transformation, CD30+ large tumor cells express CCR3. Previous reports showed that CCR10 is expressed on tumor cells in MF and SS (7, 15, 16). Consistent with this finding, our study identified CCR10 expression in 50% of MF/SS cases but in only 13% of CD30+ LPD and AD cases. Furthermore, serum levels of CCL27, a ligand for CCR10, were reported to be higher in MF patients than in normal controls (7). Collectively, these results suggest that CCR10-CCL27 interactions play a role in the development of MF/SS.
We found a significant correlation between the survival rate and the expression of CCR3 or CCR4 in MF/SS. We previously reported that IL-4 expression was much stronger when more CCR3+ lymphocytes infiltrated into lesional skin of MF/SS (17), suggesting that interactions between CCR3+ lymphocytes and tumor cells are important for establishing a Th2-dominant microenvironment for tumor survival. An association between CCR4 expression and an unfavorable outcome was reported in patients with peripheral T-cell lymphoma, unspecified (18). Similarly, in our study, higher CCR4 expression was associated with a poorer prognosis in patients with MF/SS, suggesting that CCR4 expression in the CTCL microenvironment plays important roles in tumor progression. At diagnosis, CCR3 was strongly expressed in 8% of early MF cases and 11% of advanced MF/SS cases, while CCR4 was strongly expressed in 3% of early MF cases and 23% of advanced MF/SS cases. Although the expression level of CCR3 did not correlate with the stage of MF, patients who were strongly positive for CCR3 showed a poorer prognosis. One possible explanation for this is that active interactions between CCR3 and its ligand eotaxins could be closely related to rapid progression of CTCL, which needs further studies. Interestingly, one of the early MF patients, who was strongly positive for CCR4 died within one year after diagnosis due to disease progression. As strong CCR3 and CCR4 expression could be a risk factor for a poor prognosis in MF/SS, patients who are strongly positive for CCR3 or CCR4 expression should be followed carefully. We also investigated the correlation between CCR3 expression and CCR4 expression but found no significant correlation (data not shown).
In summary, CXCR3 expression was more frequently associated with MF, whereas CCR3 expression was more often linked to CD30+ LPDs. Furthermore, expression of CCR3 or CCR4 could be a useful indicator of a poorer prognosis in MF/SS.
We thank Tamami Kaga for technical assistance. This study was supported by grants from the Ministry of Education, Culture, Sports and Technology in Japan.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize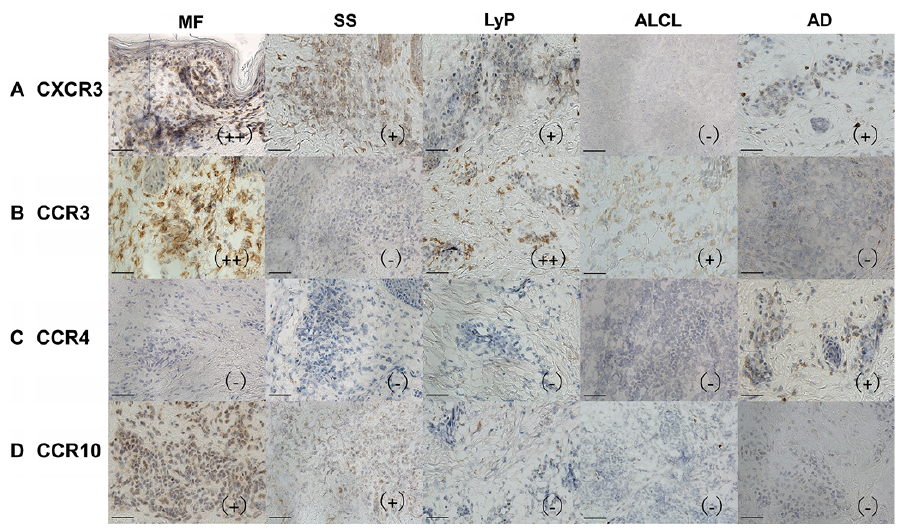 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize