


Department of Dermatology, Kurume University School of Medicine, 67 Asahimachi, Kurume, Fukuoka 830-0011, Japan. E-mail: ohata@med.kurume-u.ac.jp
Accepted Apr 30, 2019; E-published May 2, 2019
Granuloma faciale (GF) is a rare dermatosis that presents as a single or several brownish red plaques, nodules, macules and papules on the face. The aetiology of GF is unclear, and GF is occasionally refractory to treatment. Topical tacrolimus and glucocorticosteroids are the mainstay of treatment for GF. Moreover, intralesional and systemic corticosteroids, topical pimecrolimus, topical and systemic dapsone, systemic hydroxychloroquine, clofazimine, tumour necrosis factor-α inhibitors, lasers, cryosurgery, and surgery have been reported as other treatment options (1). Colchicine has, surprisingly, been reported as a treatment option in several articles, despite the lack of even an anecdotal report (2–5). We report here a case of GF in which colchicine was effective against an aggravated lesion following cessation of dapsone, which was also effective, but was stopped because of liver injury.
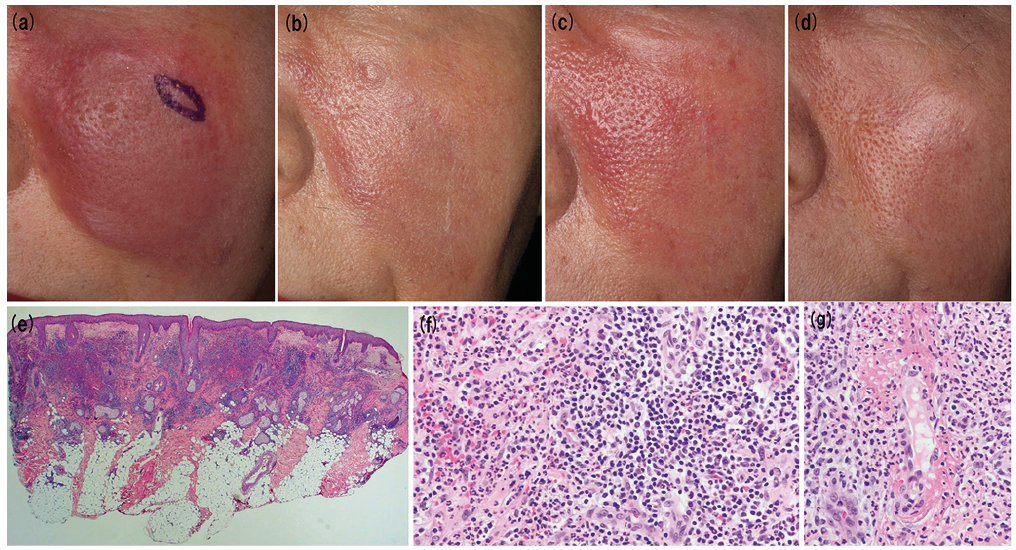
A 63-year-old woman presented with a painful, red plaque on the left cheek, which had gradually enlarged over a year. The patient was treated with minocycline, prednisolone, 35 mg/day, and/or topical corticosteroids before visiting our hospital; however, none of them was effective. The patient had a positive test result for the hepatitis C virus (HCV) antibody, whereas liver enzyme levels were within the normal range. A hepatologist did not treat the patient because serum HCV RNA was undetectable. Physical examination revealed a relatively well-demarcated dark-red plaque on the left cheek (Fig. 1a). A biopsy from the lesion revealed a dense, diffuse inflammatory cell infiltrate throughout the dermis with a narrow, uninvolved grenz zone (Fig. 1e). The infiltrate consisted of lymphocytes, neutrophils, eosinophils, and plasma cells, together with extravasated erythrocytes (Fig. 1f). The blood vessels were dilated in the upper dermis. In the mid dermis, leukocytoclastic vasculitis (LCV) with nuclear debris and eosinophilic fibrinoid material within and around the vessel were seen (Fig. 1g). Fibrosis was also observed. Based on these findings, the patient was diagnosed with GF, and dapsone, 50 mg/day, was initiated. Although, one month of this treatment alleviated the pain, the clinical manifestation of the lesion did not change. Consequently, the dose of dapsone was increased to 100 mg/day, and this cleared the lesion after one month (Fig. 1b). However, liver injury, with aspartate aminotransferase levels at 277 U/l (normal range 13–30 U/l) and alanine aminotransferase levels at 675 U/l (normal range 7–30 U/l), occurred when the lesion improved. Thus, dapsone was discontinued because of suspicion that it was causing liver injury. The patient was referred to a hepatologist, who excluded other liver diseases, infections, and drugs other than dapsone as a cause of liver injury. Liver enzyme levels returned to normal range one month after cessation of dapsone without any medication for liver injury. Three months after cessation of dapsone, the lesion recurred (Fig. 1c). Dapsone, 50 mg/day, was restarted as per the patient’s strong wish. However, liver injury occurred again, and liver injury due to dapsone was confirmed. Liver enzyme levels returned to normal range in 2 weeks after cessation of dapsone. Finally, the patient was treated with colchicine, 0.5 mg/day, which improved the lesion slightly in one week, but the response was insufficient. Increasing the colchicine dosage to 1 mg/day cleared the lesion in 2 weeks (Fig. 1d), and the lesion did not recur for 16 months with 1 mg/day colchicine.
Fig. 1. (a) Clinical manifestation at first visit. (b) Improved lesion with dapsone. (c) Recurrence of granuloma faciale after the cessation of dapsone. (d) Improved lesion with colchicine. (e) Scanning view of a biopsy specimen revealed a dense, diffuse inflammatory cell infiltrate throughout the dermis with a narrow, uninvolved grenz zone (haematoxylin and eosin (H&E) ×40). (f) The infiltrate consists of lymphocytes, neutrophils, eosinophils, and plasma cells, together with extravasated erythrocytes (H&E ×40). (g) Leukocytoclastic vasculitis with nuclear debris and eosinophilic fibrinoid material within and around the vessel in the mid dermis (H&E ×40).
GF shows a neutrophilic vascular reaction, which is indistinguishable from the histopathological change observed in erythema elevatum diutinum (EED) (1). Because of the histopathological similarities between GF and EED, similar systemic treatment options have been used for both. Dapsone is one such drug frequently used in the treatment of GF and EED. Colchicine has also been found to be successful in the treatment of patients with EED (6–8). However, to the best of our knowledge, there are no reports of GF treated with colchicine in the English-language literature.
Colchicine, an alkaloid derived from Colchicum autumnale, inhibits polymorphonuclear leukocyte chemotaxis, blocks lysosome formation, and stabilizes lysosomal membranes (9). A previous case series disclosed that low doses of colchicine (0.5–1 mg/day) were effective in the treatment of LCV (9, 10). Dapsone exerts its anti-inflammatory activity by inhibiting neutrophil chemotaxis and function. Thus, colchicine and dapsone have similar efficacy in diseases in which neutrophils play an important role, such as EED. Because GF is considered a variant of LCV, as is EED, the efficacy of colchicine on GF can be expected. In fact, that is why we used colchicine after the cessation of dapsone. The absence of previous reports of GF treated with colchicine may be due to the rarity of GF and the predominant use of dapsone, rather than colchicine. However, since adverse events are not uncommon with dapsone, another systemic treatment option may be helpful.
In the present case, although dapsone was effective, liver injury hindered its continuous use. This single case report validates the efficacy of colchicine for the treatment of GF.


 Click to show fullsize
Click to show fullsize