


1Department of Dermatology, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, 2Preventive Medicine, School of Public Health, Southern Medical University, Guangzhou, China, and 3Department of Dermatology, Hospital Ramon y Cajal, Madrid, Spain. E-mail: mdonglai@sohu.com
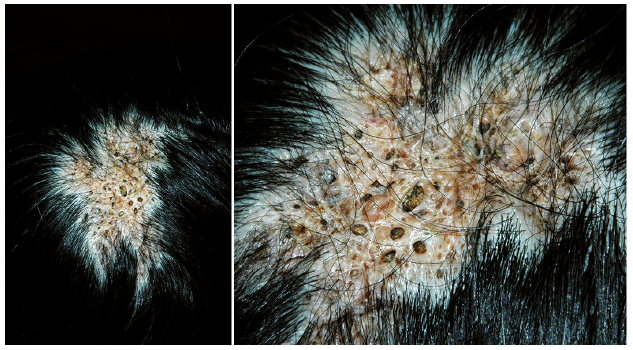
A 13-year-old girl presented with an unusual asymptomatic birthmark on her scalp. The birthmark increased in size gradually in proportion to the patient’s growth. Her physical and mental development was normal and there were no other associated neurological, skeletal or congenital anomalies. There was no family history of this disorder and no consanguinity. Physical examination revealed a 5 × 8 cm alopecic patch on the vertex of her scalp. The lesion consisted of aggregated comedo-like pits and scars (Fig. 1). Skin biopsy was taken for histopathological examination.
What is your diagnosis? See next page for answer.
Fig. 1. A circumscribed alopecic plaque on the vertex of the scalp. The lesion consisted of aggregated comedo-like pits, papules, nodules and scars.
Acta Derm Venereol 2019; XX: XX–XX.
Diagnosis: Naevus comedonicus of the scalp
Skin biopsy revealed a hyperkeratotic epidermis with cup-shaped follicular plugging (Fig. 2). Arrector pili muscles and sebaceous glands were absent. A diagnosis of naevus comedonicus (NC) was made based on the clinical and histological findings. The patient was referred to plastic surgery for treatment. The lesion was excised successfully with no complications.
Fig. 2. A hyperkeratotic epidermis with cup-shaped follicular plugging (haematoxylin & eosin, original magnification ×40).
NC is a rare subtype of epidermal naevus first described by Kofmann in 1895 (1). It has been considered a hamartoma of the pilosebaceous unit, resulting in developmental defect in production of mature hairs, matrix cells, or sebaceous glands. Only soft keratin can be formed, which results in dilated follicular orifices (2). Somatic mutation of the fibroblast growth factor receptor 2 gene (FGFR-2) is thought to be an important factor in the pathogenesis of NC (3). NC can be associated with central nervous system, ocular and skeletal abnormalities in the context of naevus comedonicus syndrome (4).
Clinically, the lesions of NC may present shortly after birth or may develop during early childhood (most commonly before the age of 10 years) (5). Growth of the lesions appears to be proportional to age, but may be accelerated during puberty due to the increase in eccrine and sebaceous secretions (4). NC is characterized by multiple asymptomatic dilated follicular openings with dark keratinous plugs resembling comedo-like lesions in a linear, unilateral distribution along Blaschko’s lines or presenting as a circumscribed plaque. Occasionally, it may associate with bacterial infections, drainage, cyst formation, and scarring, which is an inflammatory subtype of NC (6). The lesions are most commonly located on the face, neck, trunk and upper extremities. Involvement of the palms, soles and genitals has also been reported. However, involvement of the scalp is extremely rare (2, 6–8). Histology typically reveals grouped immature follicles with dilated keratin-filled invagination of the epidermis, devoid of hair shafts or well-formed sebaceous glands (7). Immunohistochemical findings showed an increased expression of proliferating cell nuclear antigen (PCNA), intercellular adhesion molecule-1(ICAM-1), HLA-DR and CD68 (9). Clinical differential diagnosis includes acne conglobata, naevus sebaceous, epidermal naevi, Favre-Racouchot syndrome and familial dyskeratotic comedones.
NC are thought to be have a benign course, but association with squamous cell carcinoma has been reported recently; thus surgical treatment or close monitoring of these patients is recommended (10). Other treatment options include systemic retinoids, topical therapy (retinoic acid, salicylic acid, 12% ammonium lactate) and ablative laser treatment (ultrapulse carbon-dioxide lasers, erbium-YAG lasers, 1450-nm diode laser), which have been used with various success (5, 8).


 Click to show fullsize
Click to show fullsize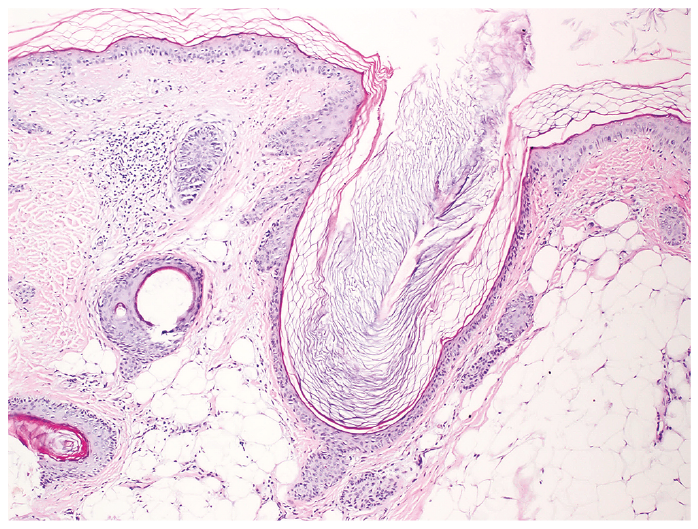 Click to show fullsize
Click to show fullsize