


LEO Innovation Lab, Silkegade 8, DK-1113 Copenhagen, Denmark. E-mail: anders.daniel@leoilab.com
Accepted May 9, 2019; E-published May 10, 2019
Psoriasis is a chronic inflammatory skin disease that affects approximately 2% of people worldwide, with a reported prevalence as high as 11.4% in western countries (1–3). Living with psoriasis increases the risk of comorbidities, such as atrial fibrillation and stroke, and can also have a detrimental impact on mental health (4, 5). Although novel medical treatments for psoriasis have been widely investigated, there is little information on the influence of diet in people with psoriasis, and the value of specific anti-inflammatory nutrients, such as the omega-3 fatty acids eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA). Both EPA and DHA have been repeatedly demonstrated to reduce the risk of inflammatory-mediated diseases, such as diseases of the cardiovascular system (6, 7), partly through direct dampening of the inflammatory tone via effects on the eicosanoids family. We hypothesize that, in people with psoriasis, this effect could impact on how the disease influences patients’ quality of life (QoL).
The aims of this study were: (i) to explore the feasibility of conducting a fully digital qualitative survey using only e-mails and text messages as the means of communication; and (ii) to explore the effect of fish-oil supplementation (which is rich in omega-3 fatty acids) in people with psoriasis, using Skindex-16, a validated questionnaire for measurement of QoL in patients with skin diseases, as an outcome measure (8).
A cohort survey was conducted over a period of 12 weeks. ’Participants were recruited in Canada using a digital platform (https://studiesandme.com/, Denmark), and pre-screened with online questionnaires. Inclusion criteria were: diagnosis of psoriasis by a medical doctor and age > 18 years. Exclusion criteria were: body mass index (BMI) > 50 kg/m2, systemic drug use, use of blood-thinning medication, diabetes, pregnancy, iodine allergy, or people waiting for surgery.
All participants provided written consent to participate in the study. The study was evaluated by the Danish ethics committee (protocol 16025688) and evaluated as a service evaluation, not a clinical study.
Participants were classified as having mild (< 3%), moderate (3–10%) or severe (> 10%) psoriasis, based on self-estimated body surface area (BSA) (9). All participants agreed to take 3 capsules of fish-oil/day (PurePharma, Copenhagen, Denmark), equivalent to 2,700 mg fish-oil (1,250 mg EPA and 500 mg DHA), as recommended by the manufacturer’s instructions, for a period of 12 weeks. Participants were asked to complete the Skindex-16 questionnaire at baseline, after 4, 8 and 12 weeks. Participants were reminded to complete the questionnaire by e-mail and text message.
For baseline characteristics χ2 or one-way analysis of variance (ANOVA) test was performed, as appropriate. For the Skindex-16 a one-way ANOVA test with repeated measurements was used. When ANOVA was used, normality checks and Levene’s test were performed and the assumptions met. For all tests, p < 0.05 was considered statistically significant. With an expected drop-out of up to 25%, we recruited 65 subjects, to get 50 completing participants.
Four hundred and seventy people applied to participate in the survey. A total of 65 people were included. Of these, 58 (89%) completed the study (Table SI). Enrolled participants were categorized as having mild (15.5%), moderate (39.6%), or severe (44.8%) psoriasis, according to their self-estimated body coverage of affected skin.
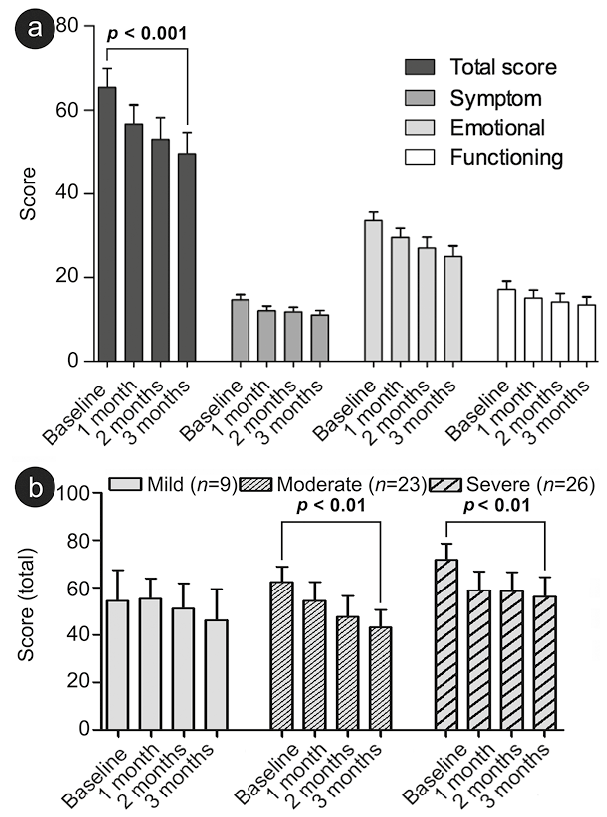
Across all participants, from baseline and throughout the 12 weeks, there were no changes in any of the 3 subdomains (symptom, emotional, and functioning) of the Skindex-16 questionnaire, although there appeared to be a trend toward a decrease in the emotional domain. The total Skindex-16 score, however, was significantly reduced (p < 0.001) from baseline to the first month, and from the first month to the end of the study (12 weeks, Fig. 1a). This reduction was similar for both sexes. When grouped into mild, moderate, and severe patients, based on the self-reported extent of psoriasis, the reduction in Skindex-16 total score over time was significant for patients categorized as moderate or severe (both p < 0.01), but not for those categorized as mild (Fig. 1b).
Fig. 1. (a) Skindex-16 scores for the 58 completing participants during the course of the study, showing a reduction in the total score from baseline to the end of the study. (b) Skindex-16 in self-reported body surface area (BSA) during the course of the study, showing that total Skindex-16 score for participants classified as moderate or severe improved from baseline to the end of the study.
This study shows that it is possible to conduct a fully digital survey of the effect of a physical treatment modality, such as a dietary supplement, without meeting the participants face-to-face or having them attend a specific location. Moreover, approximately 9 out of 10 people in the survey completed the study. This is the same retention as observed by Chambers et al. (10) when demonstrating that patient-centred online management was as effective as in-office management. Arguably, this supports the potential for using digital tools within medicine in the future, both in studies and in actual patient-management.
This survey did not show any impact of a daily dose of 1,250 mg EPA and 500 mg DHA, taken in the form of fish-oil capsules, on self-reported symptoms of psoriasis. Other comparable studies have shown confliciting results. One study (11) reports of an improvement, and another (12) of no impact of omega-3 fatty acids on subjective or clinical psoriasis symptoms.
Nonetheless, the current study showed that participants with moderate to severe disease reported that impact on QoL diminished over the 12-w period, as assessed with Skindex-16 total score. The relatively low baseline value and low number of participants may explain why this was not the case for mild patients (Fig. 1b).
The reduction in the total Skindex-16 score appears to be driven primarily by changes in the emotional domain. This finding may be related to participants feeling that they do something actively, take charge, or are being a part of a survey. As such, the reduction in total Skindex-16 may not be an effect of the fish-oil as a treatment modality per se. Because this study was not controlled it is not possible to isolate the effect of fish-oil on Skindex-16 from that of other factors. Being part of a study have previously been speculated to explain placebo effects on disease symptoms in psoriasis patients (13, 14).
This study was conducted fully remotely, requiring the participants to estimate their own BSA (disease extent), and thus might differ from what a trained dermatologist would find. Furthermore, the disease severity was not clinically evaluated; hence, measurement of effects was performed using a patient-reported outcome on QoL. The effect of the fish-oil treatment modality was not compared with that of a control group; however, it was compared with baseline.
The survey showed that, although omega-3 taken as a fish-oil supplement did not improve measures of psoriasis symptoms, the participants reported an improvement in QoL of life assessed with Skindex-16.
The product was supplied to the participants without cost, sponsored by PurePharma (shipment cost covered by LEOiLab). All of the authors are employed by LEOiLab, an independently established unit of LEO Pharma A/S.


 Click to show fullsize
Click to show fullsize