


1Department of Dermatopathology, Institute of Dermatology, Chinese Academy of Medical Sciences and Peking Union Medical College, Nanjing 210042, China, and 2Departments of Dermatology & Pathology, SUNY at Buffalo, School of Medicine and Biomedical Sciences, Buffalo Medical Group PC. *E-mail: yiqunjiang@qq.com
Accepted May 22, 2019; E-published May 23, 2019
Blau syndrome (BS) is a rare monogenic disease caused by mutation of the NOD2/CARD15 gene (1–3) and is clinically characterized by the triad of skin, joint, and eye disorders (4). We report a case of Blau syndrome with c.1000C>T (R334W) mutation in NOD2 gene in a 7-year-old Chinese girl. She also presented with a congenital ostium secundum atrial septal defect which has not been previously reported.
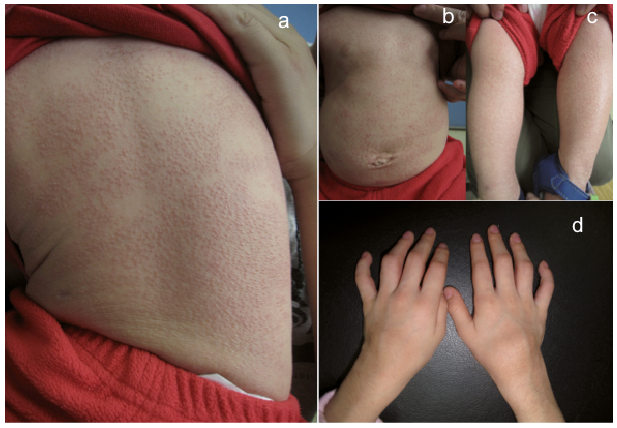
A Chinese girl initially presented to our clinic with generalized lichenoid papules over the face, trunk and limbs with moderate itching when she was 10 months old (Fig. 1a–c). Biopsy was taken 6 months later and revealed non-caseating granulomas admixed with scant lymphocytic infiltrate. Tuberculin skin test was negative. Computed tomography (CT) suggested bilateral axillary lymph node enlargement and a large pericardium, however, lung and hilar lymph nodes were negative. An elevation of sACE was detected with 178 U/l (reference range < 139 U/l). Echocardiography examination showed congenital ostium secundum atrial septal defect. She was diagnosed with sarcoidosis and treated with oral methylprednisolone at a dose of 4 mg (equivalent to prednisone of 0.5 mg/kg/day). The lesions improved significantly in 3 weeks, and the methylprednisolone was tapered to 1 mg as maintenance. The lesions recurred after the oral corticosteroid was discontinued. At the age of 4, she developed subcutaneous nodules starting on her feet, hands, and gradually involving the joints of ankles, wrists and elbows, as well as the back of hands and feet. During follow-up at 7 years of age, the girl presented with ocular manifestation of impaired vision (OD0.02+, OS0.6+). The ophthalmological examination revealed granulomatous anterior uveitis in the patient’s eyes bilaterally and old retinal vasculitis of the right. She has been treated with oral methylprednisolone at a dose of 40 mg/day and methotrexate 8.75 mg/week. No pulmonary symptoms were noted. No familial history of similar disease was present.
Fig. 1. Clinical examination showed numerous 1–2 mm, lichenoid papules over the trunk (a, b), limbs (c) and subcutaneous mass over the affected joint (d).
Dermatological examination showed numerous 1–2 mm, lichenoid erythematous papules covering the face, trunk and extremities. Subcutaneous nodules were found over the affected joints of wrists and ankles (Fig. 1d). MRI and ultrasonography showed abnormal signal in bilateral ankles, dorsum and sole of feet with unaffected bones. Multiple biopsies were performed and showed non-caseating granulomas admixed with scant lymphocytic infiltrate (Fig. 2). Gene sequencing revealed that the patient had a heterozygous c.1000C>T (p.R334W) mutation in NOD2. Altogether, the clinical and histological findings were consistent with Blau syndrome, which was further confirmed by the mutational analysis of the NOD2 gene.
Fig. 2. Histopathology revealed non-caseating granulomas admixed with scant lymphocytic infiltrate in the dermis. (a, HE, x25; b, HE, x100).
Blau syndrome is a rare, autosomal dominant, and granulomatous autoinflammatory disease, first described by Blau in 1985 (5). The most common initial features are granulomatous dermatitis with exanthema and joint involvement with granulomatous arthritis/periarthritis, while eye symptoms with granulomatous uveitis often start later, between 7 and 12 years of age (6). Other organs may be involved sporadically. Miceli-Richard et al. identified the responsible gene, the caspase recruitment gene, NOD2, which mapped to chromosomal region 16q12.1-13 in 2001 (7). To date, 18 different NOD2 mutations associated with Blau syndrome have been identified, among which were 3 main missense mutations (R334Q, R334W and L469F) in the nucleotide-binding domain (NBD) of CARD15/NOD2 (8). Our patient harvested a R334W mutation of NOD2 (9) and we believe our patient present as sporadic form of Blau syndrome, also termed early-onset childhood sarcoidosis.
We reported a sporadic form of Blau syndroms in a Chinese girl with missense mutation R334W in the NOD2 gene. In addition to the classical presentation of skin, joint, and eye involvement, our patient was born with congenital ostium secundum atrial septal defect, which was not previous reported. Blau syndrome is a rare and relatively newly described entity, and its clinical spectrum continues to expand. Our case provides some information, which would be helpful to further characterize this disease.
This work was supported by CAMS Innovation Fund for Medical Sciences (CIFMS-2017-I2M-1-017).
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize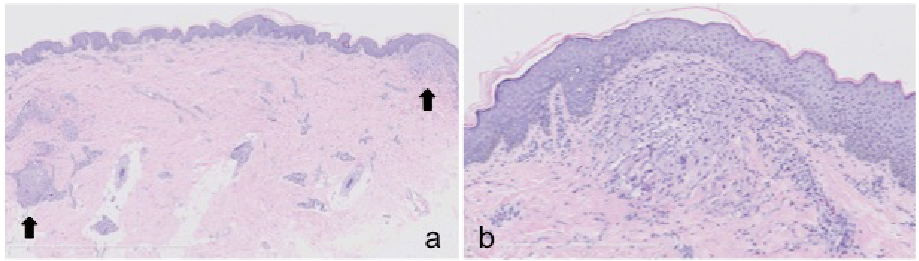 Click to show fullsize
Click to show fullsize