


St Vincent’s University Hospital, Dublin, Ireland
Microdialysis is a minimally invasive technique to study metabolic, biochemical, and pharmacological events in tissue. Factors that influence microdialysate collection include molecular weight cutoff of the membrane, perfusion rate, perfusate viscosity, duration of collection, depth of the catheter, length of the tubing and adsorption of hydrophobic molecules to the membrane. To standardize these factors, a robust sampling protocol needs to be established. Microdialysis is applied in healthy and inflamed skin. It enables the in vivo sampling of endogenous and exogenous substances in skin’s extracellular fluid. In atopic dermatitis, levels of neuropeptides, eicosanoids and histamine pre- and post-treatment treatment have been conducted. Microdialysis in atopic skin has assessed the pharmodynamics of a number of topical drugs. In psoriatic skin, the ‘cytokine fingerprint’ has been evaluated through microdialysis and bioassays. This unique fingerprint has also been analyzed after certain pharmacological treatments for psoriasis.
Key words: cutaneous microdialysis; inflammation; atopic dermatitis; psoriasis; cytokines
Accepted May 22, 2019; E-published May 23, 2019
Acta Derm Venereol
Corr: Dr Helen Rea, St Vincent’s University Hospital, Dublin 4, Ireland. E-mail: helen.rea@ucdconnect.ie
This review summarises the role of microdialysis of the skin. It is a useful tool to evaluate the skin’s biological processes in both healthy and inflamed skin. It can also enable a better understanding of the mechanism of action of certain drugs in inflamed skin. The microdialysis technique still needs to be standardised so that its practice can be used in a reproducible fashion in clinical studies. It would be interesting to carry out microdialysis in subjects with the skin condition, hidradenitis suppurativa as this research has not yet been conducted.
Microdialysis is a minimally invasive technique for the chronological study of metabolic, biochemical, and pharmacological events in living tissue (1). Microdialysis was introduced approximately 40 years ago as a method for monitoring neurotransmitters in the brain of rodents (2, 3). The first published application in humans was a study on interstitial glucose in 1987 (4). During the last two decades, microdialysis has become a well-established method for continuously sampling substances within the extracellular fluid compartment of various tissues outside the central nervous system, including subcutaneous adipose tissue, dermis, muscle and other organs (5, 6).
The usefulness of microdialysis lies in its measurement of change. This change can be provoked by spontaneous events (e.g. the metabolic deterioration in a patient in intensive care (7)) or by the topical or systemic administration of a provoking agent (e.g. oral ingestion of antimicrobial or anti-neoplastic agents and subsequent measurement of their concentrations.). It can also monitor the change evoked by administration of an active agent administered by the microdialysis catheter itself, through reverse microdialysis, which shows changes in the concentration pattern of metabolites and drugs in situ (8).
Microdialysis has many useful applications. It plays a role in neuroscience and predominantly in animal studies, enabling the measurement of neurotransmitters, small neuromodulators, amino acids and energy metabolites (9). Exogenous drugs which can be analysed by microdialysis include anti-depressants and anti-psychotics and other drugs that act on the central nervous system. Glucose concentrations in patients with diabetes (5, 10) can take place through intravascular and subcutaneous microdialysis catheter placement. Cardiac troponin has been measured in the myocardium of cardiac surgery patients (11). In the skin, the bioavailability of both topical drugs (particularly non-steroidal anti inflammatory drugs (12, 13) and systemic drugs, as well as the measurement of metabolic changes can be assessed.
Despite extensive use of microdialysis in the studies of inflammation of the skin, comparative studies with histology, plasma levels and other models are sparse. Sjogren & Anderson compared cytokine findings in the skin by microdialysis and biopsies and found moderate to excellent agreement (14). Further methodology studies may be needed to improve the translational value of microdialysis. Groth et al. (15) deduced that microdialysis technique is probably primarily useful for the study of hydrophilic substances and substances with low molecular weight and low protein binding. Since this study, Clough (16) has conducted further studies on microdialysis of large molecules. She noted that the protein dialysate level of macromolecules was significantly higher in the first 5 min of collection compared to those collected after this. This is related to a large concentration gradient between the perfusate and interstitial space, and a very fast diffusion rate as a result. In addition, the application of cutaneous microdialysis for the study of lipophilic substances needs further methodological development. Many lipophilic substances adhere to the polymeric microdialysis membrane and tubing, thus yielding lower relative recoveries of dialysate. However, Sun & Stenken (17) enhanced the microdialysis recovery of the lipophilic eicosanoids significantly through the addition of cyclodextrins or organic substances such as arachidonic acid to the perfusate.
Microdialysis equipment includes a membrane, a ca-theter, a pump, a guide needle, a sampling device and a perfusion fluid (usually normal saline) with a physiological buffer. The microdialysis technique is minimally invasive and requires the insertion of a small microdialysis catheter into the tissue of interest. The microdialysis catheter consists of a semi-permeable membrane that is continuously perfused with the physiological solution. This physiological solution is called a ‘perfusate’, and then becomes a ‘dialysate’ once it has filtered through the membrane. Pumps that are capable of low (0.1–8 µl/min) (1) but consistent speeds are required. This allows for the passive diffusion of substances. The size of the substances diffused depends on the permeability of the catheter. Depending on the size that you wish to analyse, catheters are used that allow diffusion of substances with cut offs between between 3,000 to 120,000 Daltons (9). The direction of the analysate flow is determined by the respective concentration gradient and allows the usage of microdialysis probes as sampling (retrodialysis) as well as tools for the delivery of investigated molecules or medication. The solution leaving the probe (dialysate) is collected at certain time intervals for analysis. ‘Retrodialysis’ (18) occurs when diffusible compounds are added to the perfusate, and can diffuse from the catheter into the tissue of interest, exerting their effects.
The design of microdialysis probes is divided into two basic categories: linear and concentric. The linear style probe is a membrane embedded within a length of small diameter tubing. It is usually used for tissue implants such as those in the subcutis (19), dermis (20), adipose tissue or muscle (21). Concentric probes have a membrane located at the distal end of a supporting cannula. They are most often used for accessing the extracellular fluid of the brain (22, 23). This avoids unnecessary invasiveness at this site as this probe has only one insertion point, and no exit point.
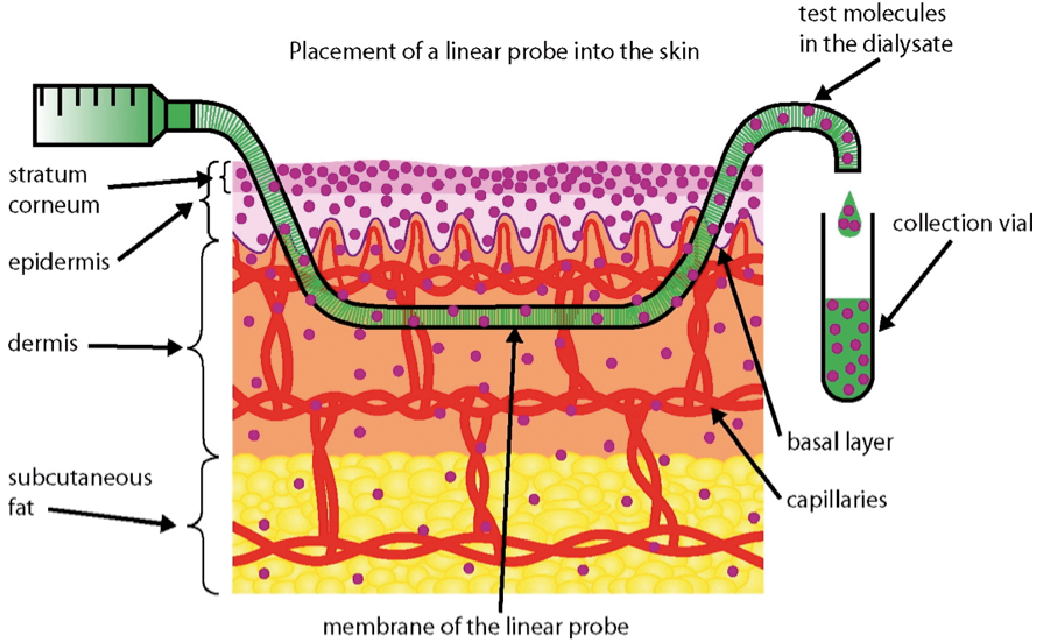
The microdialysis probe tip is inserted along the skin approximately 1 cm from the point of insertion using a guide needle. The bevel should reach the depth of the dermo–epidermal junction. The membrane is then perfused with the physiological solution at a fixed perfusion rate, usually between 2 and 5 µl/min. Effects of the probe insertion can lead to direct trauma to cells, a foreign body inflammatory reaction, including the release of interleukins and TNF alpha, and circulatory effects over a wider area by axon reflex. Anderson et al. (24) used laser Doppler perfusion imaging to investigate skin blood perfusion with skin microdialysis. They concluded that increases in skin blood perfusion tend to subside around 15 min after probe insertion and by 60 min values are near resting levels. Thus, collection of the dialysate must take place at least 15 min after probe placement, however optimal collection is after 60 min (Fig. 1).
Sample analysis is a critical step in microdialysis and various methods exist. These include enzyme-linked immunosorbent assays, radioimmunoassays and high performance liquid chromatography. Other approaches include microsphere-based protein micro-assays, electron spin resonance, immunoaffinity capillary electrophoresis, capillary electrochromatography or mass spectrometry-based proteomics (25, 26).
Fig. 1. The apparatus arrangement of a microdialysis membrane in the skin. From Ref. 13 after permission from the publisher.
Certain environmental factors can influence dialysate collection so these must be managed to ensure steady state elution. The relative recovery for different molecules can differ according to their temperature, which is directly proportional to their diffusion coefficient (27). In vivo microdialysis should be carried out at a constant body temperature of 37°C. Blood flow also influences the steady state concentration (28). Clough et al. (28) found that the magnitude of relative recovery in vivo is directly related to blood flow. This was exemplified when the relative recovery of the small diffusible molecule, sodium fluorescein was reduced by 50% through the application of a local vasodilator, glyceryl trinitrate patch. The pH values (29) of the medium surrounding the catheter influences the relative recovery of certain cytokines. In vitro, the RR of IL-10 and TNF alpha varied significantly for pH 5 and 8 respectively, compared to pH 7 (p < 0.05). However, in vivo the pH of interstitial fluid is normally 7 and this is not normally a variable.
Mechanical factors that affect collection and analysis include the molecular weight cut off of the membrane, the perfusion rate (30) (as previously discussed), perfusate fluid viscosity, the duration of collection, the depth of the catheter probe in the skin, the length of the tubing and adsorption of hydrophobic molecules to the polymeric materials in the probe and on the membrane.
The higher the molecular weight membrane cut-off of the microdialysis probe, the higher the fluid loss. Unfortunately, many of the mediators of pathological conditions of the skin are higher molecular weight peptides and proteins (5). These membranes lead to greater bulk fluid flow either in to the probe (ultrafiltration) or out of the probe (probe buffer loss.) It has been documented that significant probe fluid loss (up to 50% of expected volume) is a consequence of microdialysis in protein-containing solutions (31).
Lowering the molecular weight cut-off of the membrane can yield more dialysate volume but this limits the collection of metabolically active substances. There are two possible alternatives to overcome this problem. The first is to alter the fluid viscosity in the perfusate by adding a protein such as bovine serum albumin (BSA) to minimise the fluid loss from the microdialysis probe (32). The size of BSA prevents its diffusion across the semipermeable membrane of the microdialysis probe by placing an osmotic pressure that can offset the hydrostatic pressure forcing fluid out of the probe. The second possible solution to this problem would introduce the use a ‘push-pull’ pumping system (33). The push-pull pumping system is set up so that the ingoing pressure to the ca-theter is directly balanced against the outgoing pressure.
Poiseuille’s law applies to microdialysis collection. This states that the velocity of the steady flow of a fluid through a narrow tube (such as a catheter) varies directly as the pressure (hydrostatic pressure in the extracellular fluid space) and the fourth power of the radius of the tube and inversely as the length of the tube and the coefficient of fluid viscosity (Fig. 2).
To standardize these factors, a robust sampling technique is still to be established. A slower perfusion rate equates to less fluid loss so standardization is recommended at rate of 3–5 µl/min. The depth of the catheter probe in the skin can be standardised using a Doppler ultrasound (Dermascan A Sonotron; AB Sweden) (24). Of note, there was no statistical difference found between continuous and intermittent versus continuous only microdialysis (34) thus continuous microdialysis is the standard of practice.
Fig. 2. Poiseuille’s aw applies to Cutaneous Microdialysate Collection. This states that the velocity of the steady flow of a fluid through a narrow tube (such as a catheter) varies directly as the pressure (hydrostatic pressure in the extracellular fluid space) and the fourth power of the radius of the tube and inversely as the length of the tube and the coefficient of fluid viscosity.
The following techniques are employed to calculate the tissue uptake or delivery of substances. When the probe is used in sampling mode, the microdialysate concentration is usually a fraction of the unbound concentration in the tissue. This is known as the relative recovery. To calculate the relative recovery from the tissue in this mode, the following equation is used;
RR gain= C dialysate/C tissue, (Equation 1)
where RR (gain) is the relative recovery of the tissue uptake, C dialysate is the concentration of the dialysate and C tissue is the concentration of the tissue of interest.
Of note, an in vivo study of long term microdialysis comparing the relative recovery in linear versus concentric catheters, there was a statistically significantly lower RR in the case of linear catheters (73.3% versus 84.9%) (35).
A number of microdialysis calibration methods can be used depending on the goal of the experiment. Calibration methods in the literature are retrodialysis (36), ultraslow flow rate (37), no net flux (4) and dynamic no net flux methods (37). A good calibrator should have similar diffusion, transport and metabolism properties to the solute of interest.
The most common calibration mode is retrodialysis, which is used for drug delivery. In order to calculate the drug in the probe diffusing in to the surrounding tissue, the following equation is used;
RR loss=(C perfusate – C dialysate/C perfusate), (Equation 2)
where, RR (loss) is relative recovery (lost from the tissue), C perfusate is the concentration of the perfusate and C dialysate is the concentration of the dialysate.
Microdialysis can be used in healthy skin to monitor endogenous metabolites and their response to homeostatic perturbations such as ultraviolet radiation light, cold or pain. In addition, it is being increasingly employed to monitor exogenous substances such as free, unbound drug tissue concentrations.
Microdialysis has been extensively used in healthy skin and allows for the in vivo sampling of both endogenous and exogenous substances in the extracellular fluid, which represents up to 20% of the tissue volume. The endogenous substances include neuropeptides (such as substance P and calcitonin gene-related peptide (38, 39), insulin (5), cytokines (40), TNF alpha (41), leukotrienes (20), eicosanoids (42), nitric oxide (43), histamine (44) and growth factors.
Falcone et al. (45) recently explored 10 minimally invasive methods of sampling interleukin 1 alpha and interleukin-1 receptor antagonist, with a view to further analyse the molecular profiles of skin inflammation. The obstacles encountered in the use of microdialysis were a long collection time, adsorption on to the polymeric materials used to construct the membranes and the outlet probe and the low analyte concentration in the extracellular fluid. The effect of the skin trauma after the insertion of the microdialysis catheter on the profile of mediators was also mentioned. Despite these limitations, she concluded that the levels of the mediators measured in the fluid extracted by microdialysis, skin suction blistering and microporation were the most representative of the overall levels mediators in the skin.
Among the other techniques for in vivo sampling of biomarkers include tape stripping, skin suction blistering, adsorption by sebutape, skin chamber technique, microporation, swabbing, scraping, transdermal analysis patch, skin surface wash sampling and skin biopsies. All methods except for microdialysis measure the total tissue concentration and require a correction factor to correct for tissue binding. Of note, microdialysis is the only technique currently available that is capable of selectively sampling the unbound pharmacologically active concentrations of the analyte in the tissue (46). This is an advantage as it reduces the scope for error.
Microdialysis has been applied in normal healthy skin to investigate cytokine and neuropeptide release in inflammation following exposure to thermal stimuli (40, 47). In their study from 2016, Quist et al. (47) showed 3 peaks with the release of T helper cells were detected in an early phase (4–12 h), intermediate phase (16–24 h) and late phases (32–40 h) post-exposure. The early-phase increase in cytokine levels was more TH1 dominated, and the late phase was more TH2 dominated, whereas in the intermediate phase, a mixed TH1/ TH2 response was detectable. In an earlier ultraviolet B (UVB) light study (40) microdialysis was performed 24 h before and after the UVB challenge. This study was stopped after 24 h, and lacked a negative control. Therefore, it could not be fully concluded that the observed increases in cytokines levels may have been a result UVB exposure as opposed to the repair processes experienced after tissue trauma post-catheter insertion.
Levels of calcitriol (vitamin D3) after UVB synthesis in healthy human skin (48) has also been assessed using microdialysis. The link between ultraviolet B irradiation and synthesis of calcitriol in the skin may be of immense importance for regulation of biological processes such as skin growth, differentiation, apoptosis and immunological reactions. This study demonstrates that photolysis of 7-dihydrocholesterol (7-DHC) induced by irradiation of human skin with UVB at 300 nm results in epidermal synthesis of calcitriol (vitamin D3). Cutaneous microdialysis was utilised as a valuable tool to mirror vitamin D3 metabolism in human skin.
The effects of drugs in healthy human skin have also been analysed through the use of microdialysis. The very first publication of this use was a study of ethanol absorption into the skin by Anderson et al. (49). The study demonstrated that ethanol does penetrate the skin and that maximum dermal levels varied from 15 to 800 µg/ml between subjects. However, ethanol was only sampled for 50 min which was subsequently concluded to be sub-optimal. Drugs that have been monitored using microdialysis in human skin include those on 8-methoxypsoralen (50), propranolol (51), methyl nicotinate (52), lidocaine (53), prilocaine (54), ethanol (49, 55), isopropranol (55), salicylic acid (56), nicotine (57), estradiol (58), diclofenac (13), metronidazole (59), tacrolimus (60), polyunsaturated fatty acids (60) and botulinum neurotoxin type A (BoNTA) (61).
A bioequivalence study where lidocaine delivery from two different vehicles was compared by dermal microdialysis sampling and pharmacodynamics assessment of the pain-relieving effect of the formulations was done previously (54). Thus, microdialysis has the potential to differentiate the magnitude of drug concentrations produced by different formulations. Silva et al. (61) provided the first evidence supporting the inhibitory effect of BoNTA on glutamate release in human skin. Two microdialysis catheters were inserted 1cm from the saline and BoNTA injections and diasylate was collected for 3 h. Glutamate concentrations were determined from this. An additional finding in this study using microdialysis was that BoNTA reduced capsaicin and mild heat-evoked pain intensity and skin blood flow. Through the effective use of microdialysis it was deduced that the blockade of glutamate release may be responsible for some of the analgesic action of BoNTA.
Further knowledge in to the pathophysiology of atopic dermatitis (AD) would be of immense value to this burdensome disease. Many studies have shown that as AD severity increases, quality of life decreases (62, 63). In children, the International Study on Life with Atopic Eczema (ISOLATE) found major impacts of AD on self esteem; 27% of those had been teased or bullied because of AD and 36% said AD affected their self confidence (64).
Cutaneous microdialysis has been used in patients with AD to study the pathophysiology of AD, for example by measuring the concentrations of eicosanoids (60) and neuropeptides (65) in AD skin and comparing them with the concentrations found in healthy skin. In a similar fashion to its applications in healthy skin, it has also been used to analyse the effects and penetration of topical drugs (66, 67) on atopic skin as well as a tool to deliver drugs (68).
A recent study demonstrated through dermal microdialysis that levels of pro-inflammatory eicosanoids (prostaglandins and isoprostanes) are increased in lesional AD skin compared with nonlesional AD skin (62). In addition, treatment with the topical immune modulator tacrolimus suppresses the interstitial release of eisosanoids, thus reducing inflammation and subsequent skin erythema. Topical treatment with w-6-fatty acids was also found to reduce the level of isoprostanes, but not prostaglandin PGE2.
Microdialysis can be used to measure levels of neuro-peptides in the skin. One study compared the levels in nerve growth factor (NGF) in atopic skin and healthy skin (65). It was previously reported that increased plasma levels of NGF and substance P in AD patients correlated with disease severity and plasma NGF and thereby was suggested as a marker of disease severity. This microdialysis study did not support this concept as it found that levels of NGF vary throughout the day and overall serum NGF levels were found to be lower in comparison to healthy subjects.
Microdialysis is also utilised as a tool for delivering drugs. Neisius et al. (68) applied prostaglandin E2 via microdialysis capillaries and analysed protein extravasation. The study did not reveal any significant difference (p < 0.05) in the time course of protein concentration between AD skin and controls. Thus, PGE2 was found to be a potent vasodilator and weak pruritic in both normal skin and atopic skin, yielding no evidence for a special use of PGE2 in AD.
Rudwied et al. (69) also used microdialysis capillaries to apply the mast cell degranulating substance compound 48/80 or histamine and also to deliver H1 blockade (cetirizine). Protein extravasation induced by the substance 48/80 and histamine was significantly reduced in AD patients. In addition, pruritus in AD patients was unchanged after H1 blockade, suggesting that mast cell mediators other than histamine are involved in itch in these patients.
Few techniques are available for the assessment of in vivo topical drug penetration in human skin. Dermal microdialysis is regarded as the technique of choice for the study of topical drug pharmacodynamics in AD skin. The penetration of topical metronidazole (59) and topical salicylic acid (56) have been assessed. Dermal microdialysis demonstrated a 2.4-fold increased penetration of the metronidazole topical formulation in active AD skin compared with uninvolved skin. Benfeldt et al. (56) demonstrated that the penetration of salicylic acid is initially much increased in AD skin compared with healthy skin but is reduced in skin with chronic AD. The reason for this is that the barrier capacity of the corneum stratum, (as measured by trans-epidermal water loss) in AD decreases with each topical treatment of salicylic acid. Thus, more skin barrier perturbation resulted in less drug penetration.
Variability in patient response to any given drug is still poorly understood. Even when a treatment response is seen, the degree of response is variable among patients (70). Cutaneous microdialysis could facilitate in filling gaps in knowledge in psoriasis. This would be of immense importance given the marked impact this disease has on a patient’s physical and psychological quality of life. Clinical depression (13.8% vs 4.3%), anxiety (22.7% vs 11.1%) and suicidal ideation (17.3% vs 8.3%) are significantly higher in this cohort of patients compared with controls (71). Indeed, some psoriasis scoring tools incorporate psychosocial disability in to their assessment, emphasizing the psychological impact of this condition (72). The Salford Psoriasis Index is derived from combining a score of current severity of psoriasis based on the clinical assessment from the PASI, a score indicating psychosocial disability and a score based on historical information. This score recognises that some patients have a large degree of psychological disability from psoriasis despite a low PASI score.
Microdialysis has been used to measure endogenous substances in psoriatic skin. Sjögren et al. (73) carried out microdialysis on lesional and non-lesional psoriatic skin over 24 h in 3 subjects. These were compared to a reference group of 10 healthy controls. The median concentrations of 5 pro-inflammatory cytokines were collected hourly over 24 h and compared to controls. All microdialysis samples were investigated for cytokine content with a bead-based multiplex immunoassay from luminex. This study suggests that analysis of a ‘cytokine fingerprint’ for a range of cytokines or other mediators over 24 h is a possible basis for consideration in inflammatory dermatoses. The findings of note include a statistically significant elevation in the cytokine granulocyte-macrophage colony-stimulating factor in both lesional and non lesional skin of psoriatic patients at 3–8 h compared with controls (p < 0.05). In addition, Interleukin (IL)-8 was found to be significantly elevated (p < 0.05) in the lesional psoriatic group compared with the controls at 0–2 h.
Another study assessed the cytokines profile of 3 patients receiving treatment with fumaric acid esters for 12 weeks (74). All patients showed significant clinical improvement and this correlated with a decrease in concentrations of the pro-inflammatory cytokines IL-6, IL-18, IL-23, but not IL-2 and adiponectin in lesional skin.
Besides cytokines, the insulin antagonizing adipokine resistin was found to be substantially elevated in psoriatic plaques in this study, indicating a metabolic state of insulin resistance (74). The presence of mediators inhibiting insulin receptor signalling in lesional psoriatic skin may directly contribute to the altered epidermal homeostasis characteristic for this disease. It is well established that insulin plays a major role in homeostasis of the skin (75).
IL-1β levels were monitored successfully using microdialysis (76). This cytokine is present in high concentrations in tissue fluid from patients with psoriasis and is reduced with successful anti-psoriatic therapy. It is already established that insulin is a pre-requisite for proper formation of the epidermal structure by participating in keratinocyte formation. IL-1β interferes with this mechanism and contributes to the pathogenesis of psoriasis with dual effects. Firstly, it blocks insulin-mediated differentiation by means of insulin resistance via p38MAPK (mitogen activated protein kinase). Secondly, IL-1β activates protein kinase B which induces proliferation and induces proliferation of keratinocytes. This study demonstrated the extent to which ILβ contributes to psoriasis via microdialysis and subsequent fluorescent bead immunoassay and was confirmed by immunohistochemistry of keratinocytes.
Microdialysis has been utilised for the investigation of granulocytes and histamine concentrations in psoriasis and to follow these parameters during therapy with high dose ranitidine (77). Compared to control skin in healthy volunteers, this study showed that mast cells are higher in number (p < 0.05), skin and plasma histamine concentrations are increased and histamine release to mast cell secretagogues (codeine and substance P) were raised by 10- and 2-fold, respectively at baseline. After treatment with a H2 antihistamine, ranitidine, these responses returned to normal. These results suggest a decrease in histamine release during remission in psoriatic patients. An earlier microdialysis study (78) echos these findings. Both the perfusion and interstitial concentrations of histamine as well as the net release of histamine after the topical application of capsaicin were significantly increased in both lesional and peri lesional skin.
Levels of iron and ascorbic acid in psoriatic skin have also been assessed using microdialysis (79). It has been shown that levels of free iron in these patients is significantly higher and the level of ascorbic acid significantly lower compared to healthy controls. It is hypothesised that the ascorbic acid is lower as a result of the inflammatory process in which free iron is released from storage proteins and then produces reactive oxygen species (ROS), which are then scavenged by anti-oxidants such as ascorbic acid.
Microdialysis is a useful technique for measuring drug levels in the psoriatic skin. Methotrexate levels have been assessed (80) and it was found that drug levels and the bioavailability of methotrexate was higher in lesional compared to nonlesional skin. Methotrexate levels reach a higher concentration at an earlier time point with a higher overall bioavailability but reside for shorter time in the psoriatic plaque than in the nonlesional skin. However, the pharmacokinetic profiles of patients receiving methotrexate are highly individual and not primarily dependent on dose or route of administration. The study demonstrated that subcutaneous administration was not superior to oral administration regarding bioavailability and drug levels or area under the curve, as other current studies suggest.


 Click to show fullsize
Click to show fullsize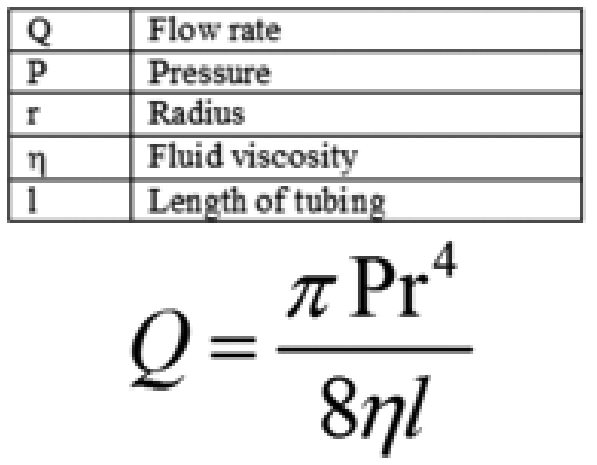 Click to show fullsize
Click to show fullsize