


1Department of Dermatology, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, No. 1 Shuaifuyuan, Dongcheng District, Beijing, and 2Preventive Medicine, School of Public Health, Southern Medical University, Guangzhou, China. E-mail: mdonglai@sohu.com
A 66-year-old man presented with a 1-year history of asymptomatic hyperpigmented plaque on his apex nasi. The lesion initially appeared as erythematous macules, and several open, black comedones gradually developed. The patient was a farmer and had worked outdoors for more than 40 years without sun protection, which resulted in substantial sun exposure. He also had smoked >10 cigarettes daily for more than 40 years. On physical examination, a 1.5×2-cm hyperpigmented plaque was located on the apex nasi; it showed symmetrical distribution of multiple open, black comedones (Fig. 1A). Wrinkles and furrows were present on the patient’s forehead. The remainder of his physical examination was unremarkable. Laboratory tests were negative, including complete blood count, antinuclear antibodies, and dsDNA antibodies. A lesional punch biopsy showed epidermal atrophy, solar elastosis, and multiple dilated follicular infundibula filled with laminated keratinous material (Fig. 1B). Focal elastosis and degeneration of elastic fibres were observed in the dermis (Fig. 1C).
What is your diagnosis? See next page for answer.
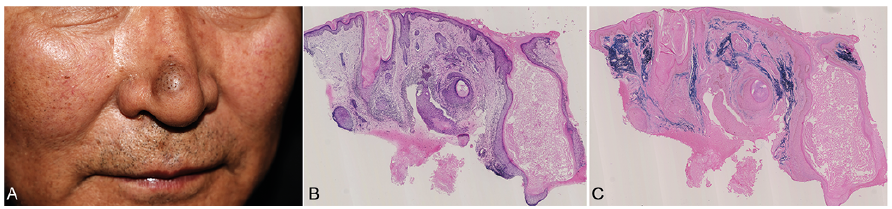
Fig. 1. (A) Clinical image. A hyperpigmented plaque with multiple open, black comedones on the apex nasi. (B) Histopathological image. A lesional punch biopsy showed epidermal atrophy, solar elastosis, and multiple dilated follicular infundibula filled with laminated keratinous material (haematoxylin-eosin staining ×40). (C) Special stain image. Focal elastosis and degeneration of elastic fibres were observed in the dermis (elastic fibre staining ×40).
Acta Derm Venereol
Diagnosis: Actinic comedonal plaque
Favré-Racouchot syndrome (FRS) is a complication caused by chronic actinic damage to the skin, characterized by atrophic skin, multiple open comedones, cysts, and nodules; marked solar elastosis of adjacent skin is also observed (1). FRS occurs in up to 6% of patients between the ages of 40 and 60 years (2). Men seem to be affected more frequently than women.
Actinic comedonal plaque is a rare and ectopic form of FRS. It was first named in 1980 by Eastern & Martin in a series of 5 elderly fair-skinned patients who exhibited lesions of confluent plaques, nodules, and comedone-like structures (3). In contrast to typical FRS, which shows distribution on temporal and periorbital areas, particularly surrounding the lateral canthi, lesions of actinic comedonal plaque can be found in the forearms, thorax, neck, ear helices, and chest, as well as in sun-protected areas (1, 4). Histological changes in actinic comedonal plaque typically comprise an atrophic epidermis, follicular plugging, solar elastosis and possible basophilic degeneration of collagen bundles. Dilated follicles and large cystic structures may be noted in the dermis. Most published case reports describe elderly fair-skinned individuals; in contrast, the patient in this case was a Fitzpatrick skin type III–IV farmer who otherwise met the diagnostic criteria for actinic comedonal plaque.
Although the exact mechanism of the condition is un-known, sun exposure, smoking, and therapeutic radiation are considered to be important causative factors. Ultraviolet radiation is known to cause sebaceous gland hyperplasia, thereby inducing elastic fibre degeneration (1). Loss of supporting properties of the dermis induces distension of the infundibular canal within sebaceous follicles, thus causing the onset of comedones (1, 5). Similar changes can be detected after radiotherapy (6).
The lesion should be distinguished clinically and histopa-thologically from comedonal naevus. However, a comedonal naevus is typically present at birth or appears during childhood, while the lesion in our patient developed after 65 years of age. Other clinical differential diagnoses include colloid milium, seborrhoeic keratosis, and amyloidosis, which can be ruled out on the basis of typical histopathological manifestations. Finally, detailed examinations should be performed to detect signs of premalignant and malignant skin lesions.
Photoprotection is suggested in patients with actinic comedonal plaque or FRS; furthermore, long-term use of retinoic acid can help to improve the lesions. Other therapeutic options include cryotherapy, CO2 laser treatment, comedone extraction, dermabrasion and curettage, plasma exeresis, and surgical excision (4, 7). The patient was prescribed topical tretinoin cream once per day and was advised to reduce sun exposure and use sunscreen. At the 1-month follow-up visit, the lesion did not show considerable change.


 Click to show fullsize
Click to show fullsize