


1Department of Dermatology, Taipei Medical University Hospital, No. 252, Wuxing St, Xinyi District, Taipei City, 110, 2Department of Emergency Medicine, National Taiwan University Hospital Hsin-Chu Branch, Hsinchu, and 3Department of Dermatology, School of Medicine, College of Medicine, Taipei Medical University, Taipei, Taiwan. *E-mail: living-white@yahoo.com.tw
Accepted Jun 18, 2019; E-published Jun 24, 2019
Lichen planus (LP), a chronic inflammatory skin disease, is a dermatopathological prototype of lichenoid interface dermatitis. The glans penis is the predisposed site of genital LP (1). In male patients, genital LP is a common non-infectious cause of balanitis. Male genital LP often presents with erosions with pruritus and soreness (2), and potential complications, such as scarring and phimosis, may occur (3). Management of genital LP is challenging due to a chronic relapsing course, and circumcision is suggested for patients who are refractory to conservative treatment (2, 4). The benefits of circumcision for the other 2 most common causes of balanitis, namely lichen sclerosus and Zoon’s balanitis (4), are well established, whereas evidence relating to the effects of circumcision on penile LP is limited. This study analysed the association of circumcision status with genital LP through a systematic review and meta-analysis.
Using “circumcision” and “lichen planus” as keywords, a systematic search was carried out for eligible studies published before 10 February 2019, in PubMed, Embase, Web of Science, and Cochrane Library. The number of patients with genital LP was compared for circumcised and uncircumcised men. Quality of included studies was assessed using Joanna Briggs Institute critical appraisal checklist for case series (5). A random effects model was used for pooled analysis, and data were represented with a risk ratio (RR) and a 95% confidence interval (CI). Heterogeneity across studies was assessed using the χ2 statistic and the I2 statistic, and the risk of publication bias was further assessed using Egger’s test. For all results, a 2-sided p-value < 0.05 was considered statistically significant. All statistical analyses were performed using Comprehensive Meta-Analysis version 3.0 (Biostat, Englewood, NJ, USA).
Three studies (6–8), published between 2012 and 2017, were finally included for meta-analysis after sequential exclusion of 82 preliminary studies. A total of 32 patients and 60 patients with penile LP in 334 circumcised men and 1,130 uncircumcised men were identified, respectively. Table I presents the basic characteristics of these studies, and Table SI shows the evaluations of study quality of each study. It was observed that patients who underwent circumcision had a higher risk of vulnerability to LP than did those who were not circumcised (RR 1.851, 95% CI 1.233–2.780, p = 0.003, Fig. 1). Low heterogeneity across studies was detected (I2 = 0.000%), and no significant publication bias was found using Egger’s test (p = 0.76479).
Table I. Basic characteristics of included studies in meta-analysis
Fig. 1. Forest plot for comparison of the risk of penile lichen planus between circumcised and uncircumcised patients. 95% CI: confidence interval.
Unexpectedly, this meta-analysis indicated a higher risk of male genital LP in circumcised men. Some possible explanations were proposed. First, genital LP is easier to diagnose in circumcised men (8). However, more than half of patients with genital LP were uncircumcised in all studies included in the current meta-analysis. You et al. reported that LP accounts for 12.8% of genital dermatoses over the glans penis in circumcised Korean men (9), which was similar to the mean percentage (10.1%) of genital LP in the circumcised group for all 3 studies in the current meta-analysis. Secondly, LP is a common dermatosis exhibiting the Koebner phenomenon. The exposed glans of the postcircumcision penis may be more vulnerable to friction or trauma (4). Thirdly, the benefits of circumcision for genital LP featured only in case reports (10), but no randomized controlled trials exist. Circumcision is considered hazardous when used to treat penile LP because of the risk of the Koebner phenomenon (10). For patients with genital LP intract-able to conservative therapies, the risks and benefits of circumcision should be weighed thoroughly and discussed with patients.
Limitations of this study are related to the design and information of included original reports. Such limitations include selection bias of case series, no known disease course between LP and circumcision, insufficient data for disease severity associating with the status of circumcision, lack of data regarding circumcision status for some cases, and the limited number of cases concerning different ethnicities.
In conclusion, this meta-analysis suggests that genital LP is more common in circumcised groups and other factors, such as ethnicity, may be taken into consideration.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize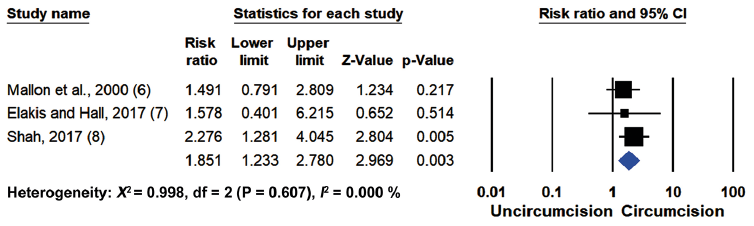 Click to show fullsize
Click to show fullsize