


1Department of Dermatology, Hospital de la Santa Creu i Sant Pau, Barcelona, Spain, 2Eli Lilly and Company, Vienna, Austria, 3Global Statistical Sciences, Lilly Deutschland GmbH, Bad Homburg, Germany, 4Eli Lilly and Company, Stockholm, Sweden, and 5Department of Dermatology and Allergy, Gentofte Hospital, University of Copenhagen, Denmark
Treatment goals defined by the absolute Psoriasis Area and Severity Index (PASI) scores offer certain advantages in the clinical setting. In order to investigate potential treatment targets, this study evaluated absolute PASI outcomes relative to other measures of response using data from two randomized clinical trials of patients with moderate-to-severe psoriasis treated with ixekizumab, etanercept, or placebo (n=2,567). Response was assessed throughout 12 weeks as the proportion of patients achieving absolute PASI band cut-offs who also reached established response criteria. Most PASI band ≤2 responders also achieved PASI 90 (70.1–100%), static Physician’s Global Assessment (0,1) (91.3–96.1%), Dermatology Life Quality Index (0,1) (63.0–67.7%), Patient Global Assessment of Disease Severity (0,1) (80.3–86.7%), and Itch Numeric Rating Scale improvement ≥4 (87.2–87.6%). Agreement sharply decreased for less stringent PASI criteria. These data indicate that PASI ≤2 represents significantly meaningful clinical and health-related quality of life improvements and may be a suitable treatment target for moderate-to-severe plaque psoriasis.
Key words: ixekizumab; psoriasis; disease management.
Accepted Jun 25, 2019; E-published Jun 26, 2019
Acta Derm Venereol
Corr: Martin Dossenbach, Eli Lilly and Company, Kölblgasse 8–10, AT-1030, Vienna, Austria. E-mail: dossenbach_martin@lilly.com
Psoriasis treatment goals defined in terms of the absolute Psoriasis Area and Severity Index (PASI) scores offer certain advantages in the clinical setting, but a consensus on a treatment goal based on absolute PASI has not yet been achieved. The current study was conducted in order to evaluate different absolute PASI treatment targets relative to other measures of the response to treatment based on the data derived from two large clinical studies of patients with moderate-to-severe plaque psoriasis. These data indicate that PASI ≤ 2 represents significantly meaningful clinical and health-related quality of life improvements and may be a suitable treatment target for moderate-to-severe plaque psoriasis.
Psoriasis is a chronic inflammatory disease of the skin, nails, and joints that affects at least 100 million people worldwide (1). Typical cutaneous signs of the disease are erythematous raised lesions covered by white or silvery scales. Itching, stinging, and pain are common symptoms. Psoriasis can be associated with several comorbidities, such as metabolic syndrome and cardiovascular disease, which add to its physical and psychological burden, negatively affecting the patient’s health-related quality of life (HRQoL) (1–3).
Optimal management of psoriasis requires well-defined treatment goals based on reproducible and objective assessment methods of the disease severity. The Psoriasis Area and Severity Index (PASI) is a widely used tool for evaluating the severity and extent of psoriasis, which takes into consideration the intensity of erythema, desquamation, and induration present as well as the percentage of body surface area involved for the head, trunk, and extremities (3, 4). An overall composite score from 0 to 72 is calculated, with higher scores indicating greater disease severity (3, 4). In clinical studies, a reduction from baseline in absolute PASI score of ≥75% (PASI 75) or ≥ 90% (PASI 90) is recommended as a primary endpoint to assess the treatment efficacy by the European Medicines Agency (5). Moreover, PASI 75 and PASI 90 responses have been found to be positively associated with patients’ HRQoL assessments, indicative of clinically meaningful improvements in the disease activity (2, 6). However, the use of relative PASI measures has some limitations. Notably, calculation of the relative PASI requires knowledge of the baseline disease status, which may not be known in routine clinical practice or other clinical settings where patients may switch from other treatments without a washout period (7). Further, patients, particularly those with moderate-to-severe disease, may reach PASI 75 or PASI 90 relative to their initial disease status but still have significant disease activity and HRQoL problems (2, 6). As the absolute PASI has the advantage of being indicative of the individual patient’s severity of disease at the time of analysis, independent of baseline PASI score, use of alternative treatment targets based on the absolute PASI scores have been proposed for assessment the effectiveness of new treatments (6). Previously, PASI ≤ 2, ≤ 3, and ≤ 5 have been suggested as potential therapeutic targets; however, the level of absolute PASI that could serve as an optimal treatment target for clinical studies and real-world use is currently unclear (2, 6−8).
To investigate this, we performed a post hoc analysis of the pooled efficacy data from patients in two phase 3 trials on ixekizumab, a high-affinity humanized monoclonal antibody that selectively targets interleukin-17A, for the treatment of moderate-to-severe plaque psoriasis in adults. In the UNCOVER-2 and UNCOVER-3 trials, ixekizumab demonstrated a favorable safety profile and clear clinical benefits, with superior efficacy to both placebo and the tumor necrosis factor-alpha inhibitor etanercept in terms of PASI 75, PASI 90, and PASI 100 responses following a 12-week induction phase (9). The current analysis is based on the data collected throughout 12 weeks of treatment (induction period) and aims to determine the degree of overlap in responders meeting various absolute PASI and relative PASI criteria to identify a level of absolute PASI that could serve as an alternative treatment goal. To further validate potential treatment targets, absolute PASI responders were also evaluated against responders defined by another commonly used clinical index of disease severity, the static Physician’s Global Assessment (sPGA), and multiple patient-reported outcomes in order to determine the absolute PASI targets representing meaningful improvement in disease activity and HRQoL.
This is a post hoc analysis of the pooled efficacy data from patients in two randomized, double-blind, placebo- and active-controlled phase 3 clinical trials, UNCOVER-2 and UNCOVER-3 (NCT01597245 and NCT01646177, respectively), comparing etanercept and ixekizumab efficacy and safety profiles in adult patients with moderate-to-severe plaque psoriasis. The eligibility criteria for the studies were similar and have been previously published (9). Briefly, the studies included patients ≥ 18 years of age with a confirmed diagnosis of chronic moderate-to-severe plaque psoriasis ≥ 6 months prior to the baseline with a minimum 10% body surface area involvement, an sPGA score ≥ 3 (0–5 scale, in order of increasing severity), and a PASI score ≥ 12 at screening and baseline visits. Key exclusion criteria included any active or recent infections at baseline; erythrodermic, generalized pustular, or guttate forms of psoriasis; and prior exposure to etanercept (9). All studies were conducted with the approval of each center’s institutional review board or independent ethics committee and in accordance with the guiding principles of the Declaration of Helsinki. All patients provided written informed consent prior to enrollment.
The original designs for the two studies have been published previously (9). The current analysis is based on the data collected during the 12-week induction periods of these studies, where the response to the two treatment regimens of ixekizumab, the active comparator etanercept, and placebo has been compared. Patients were randomly assigned 2:2:2:1 to receive subcutaneous 160 mg ixekizumab (starting dose) followed by 80 mg every 2 weeks (Q2W) or 4 weeks (Q4W), etanercept 50 mg twice weekly, or placebo.
Efficacy measures of interest in the current analysis included assessments of disease activity, including the proportion of patients achieving PASI 75, PASI 90, and absolute PASI criteria of ≤ 1, ≤ 2, ≤ 3, and ≤ 5 following 1, 2, 4, 8, and 12 weeks of treatment. To gain further insight into the distribution of responses at each time point, absolute PASI response data from the original studies were regrouped into 6 non-overlapping categories representing the proportion of patients reaching absolute PASI bands: PASI = 0; PASI > 0 to ≤ 1; PASI > 1 to ≤ 2; PASI > 2 to ≤ 3; PASI > 3 to ≤ 5; and PASI > 5. The proportion of patients per treatment group achieving each absolute PASI band criterion was assessed at each study endpoint in the induction phase.
Using data pooled across all treatments, the percentage overlap between each population of absolute PASI band response and the populations of PASI 75, PASI 90, and sPGA responders at week 12 was also determined. Treatment response for the sPGA was considered as achieving scores of 0 (clear) or 1 (minimal disease). Patient-reported outcomes reflective of HRQoL were also examined in this manner and included the proportion of patients showing improvement on the Dermatology Life Quality Index (DLQI), the Itch Numeric Rating Scale (NRS), and the Patient Global Assessment of Disease Severity (PatGA). The DLQI is a self-administered instrument that consists of 10 questions rating the impact of skin symptoms on various HRQoL domains over the previous 7 days, for a possible composite score of up to 30 (10). The current analyses used DLQI (0,1) as the response criterion, indicative of no effect of psoriasis or psoriasis treatment on the patient’s life (11). The Itch NRS is an instrument comprising of one question, with scores from no itch to worst itch imaginable (from 0 to 10) in the past 24 h (12). Treatment response was defined herein as a ≥4-point improvement from baseline on the Itch NRS. The PatGA is a single-item questionnaire in which the patient scores their symptoms on a 0–5 NRS (clear to severe), with a score of 0 or 1 set as the response criterion for this study.
To determine whether the baseline PASI affected the response to treatment, the proportion of patients reaching each absolute PASI band criterion at week 12 were assessed after categorizing patients into groups with baseline PASI < 20 or baseline PASI ≥ 20. Mean DLQI, PatGA, and Itch NRS at week 12 were also summarized overall and by baseline PASI category.
This was a post hoc analysis of pooled data collected from the intent-to-treat populations from two phase 3 clinical trials. The data cut-off date for this analysis was September 1, 2015. For categorical variables, missing data were imputed using non-responder imputation (NRI) for binary endpoints or last-observation carried forward (LOCF) for continuous outcomes. NRI assumes that every patient who discontinues is a non-responder; LOCF assumes that discontinued patients will have the same efficacy response for the remainder of the study. As the Q4W (every 4 weeks) ixekizumab regimen is not approved for use in the European Union, the Q4W data are only included in the integrated analyses of all treatments combined, and data for Q2W (every 2 weeks) (the approved dose) alone are otherwise shown in comparisons to placebo and etanercept treatment.
For comparisons between the proportions of patients meeting absolute PASI criteria by treatment group, a Cochran-Mantel-Haenszel test stratified by study was performed. Two-sided statistical tests were performed where p < 0.05 was considered statistically significant. Due to the exploratory nature of these analyses, no correction for multiplicity was performed. To compare the absolute PASI measures to other well-established indices of disease severity and HRQoL, the percentage of patients reaching each criterion of interest (PASI 75, PASI 90, sPGA [0,1], DLQI [0,1], PatGA [0,1], and Itch NRS improvement ≥ 4) who also reached each absolute PASI band cutoff was determined. For these analyses, all patients with data available at baseline and week 12 were pooled across treatment groups.
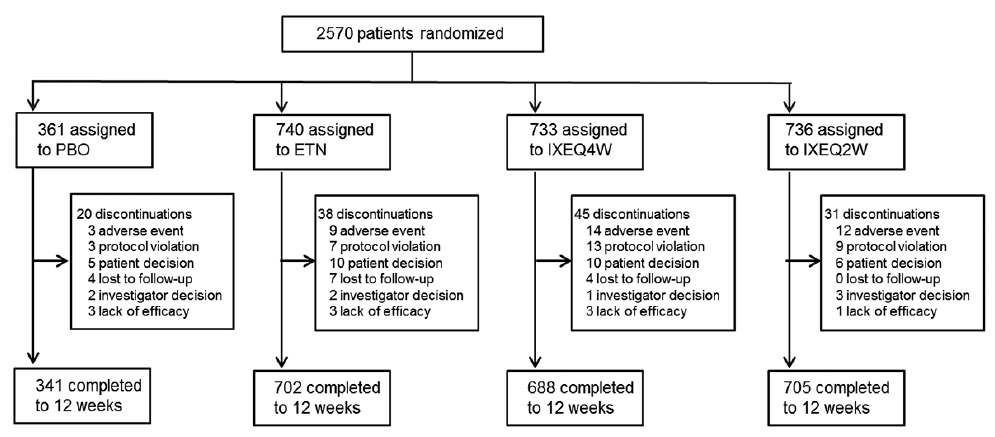
A total of 2,570 patients participated in the two studies. Patient disposition and clinical details for the individual studies have been previously reported in detail (9). An overview of patient disposition of the combined studies throughout the 12-week induction phase is provided in Fig. 1. For the current analyses, 3 subjects were excluded from the absolute PASI band analyses due to the missing baseline values on several measures.
Fig. 1. Patient disposition during the 12-week induction period of UNCOVER-2 and UNCOVER-3. Three additional patients who were randomized were excluded from the Psoriasis Area Severity Index (PASI) band analyses due to the missing baseline data. Ixekizumab 80 mg every 4 weeks (IXEQ4W) data are only included in the all-treatment-combined analyses. ETN: etanercept; IXEQ2W: ixekizumab 80 mg every 2 weeks; PBO: placebo. (Data from Ref. 9).
Table I shows selected summary demographics and baseline characteristics by treatment group for the combined studies. Across treatment groups, the patients had similar baseline characteristics, the majority comprising of white males with the mean psoriasis duration > 18 years and mean body surface area involvement of > 26% (Table I). Approximately 60% of patients had previously received at least one form of systemic therapy for psoriasis (Table I). The mean ± standard deviation (SD) baseline PASI score across all treatment groups was 20.29 ± 7.76 (range 12.0–63.0; median = 17.90).
Table I. Baseline demographics and clinical characteristics of patients with moderate-to-severe psoriasis: integrated analysis of UNCOVER-2 and UNCOVER-3
As previously reported in terms of the relative PASI response rates (9), the absolute PASI response rates for ixekizumab Q2W treatment were significantly higher across the 12-week induction period compared to the response rates for the placebo and etanercept treatment groups (Fig. 2). Notably, by week 2, a significantly greater proportion of patients in the ixekizumab treatment group reached PASI ≤ 1, and differences were sustained at all endpoints through 12 weeks (week 12 PASI ≤ 1 response rates: 54.6% ixekizumab vs. 13.4% etanercept vs. 0.8% placebo, p < 0.001; Fig. 2). Similar results were obtained for PASI ≤ 2, ≤ 3, and ≤ 5, with significant differences in response to ixekizumab compared to etanercept or placebo detected as early as week 1 for the absolute PASI ≤3 and ≤5 criteria (Fig. 2).
Fig. 2. Proportion of patients achieving absolute Psoriasis Area Severity Index (PASI) criteria from baseline through week 12 (non-responder imputation (NRI)) of UNCOVER-2 and UNCOVER-3. Percentages for each time point are color coded by treatment group. p-value from Cochran-Mantel-Haenszel test stratified by study. a) Placebo (PBO) at p < 0.001; b) vs Etanercept (ETN) at p < 0.001; c) vs PBO at p < 0.05; d) vs ETN at p < 0.05. For simplicity, zero values are not labeled.; IXE Q2W: ixekizumab 80 mg every 2 weeks.
Fig. 3 illustrates the differences in the distribution of responses to each treatment in terms of non-overlapping absolute PASI band categories. This breakdown of data indicates that, compared to patients who received etanercept or placebo, more patients treated with ixekizumab were distributed across the lower absolute PASI categories at all time points during the 12 weeks of treatment (Fig. 3). For example, at week 12, 80.8% of patients in the ixekizumab treatment group were categorized as ≤3 responders compared to 34.8% in the etanercept group and 3.7% in the placebo group, respectively.
Fig. 3. Comparison of relative response rates across treatment groups (non-responder imputation (NRI)) using absolute Psoriasis Area Severity Index (PASI) band criteria at 1, 2, 4, 8, and 12 weeks. The relative proportions of patients reaching each absolute PASI criterion are shown by treatment group and time point. ETN: etanercept; IXE Q2W: ixekizumab 80 mg every 2 weeks; PBO: placebo.
The proportion of responders across all treatments at week 12 for each absolute PASI band criterion was further examined relative to response on other disease severity indices (Table II). At week 12, of the patients classified as absolute PASI band > 0 to ≤ 1 responders, 100% of patients also met PASI 90 and 96.1% met sPGA (0,1), indicating excellent agreement between these response criteria. Similarly, the majority of patients with an absolute PASI > 1 to ≤ 2 response at week 12 also had a PASI 90 (70.1%) and sPGA (0,1) (91.3%) response, but the level of agreement sharply decreased thereafter for decreasingly stringent absolute PASI band criteria (Table II).
Regarding the patient-reported outcomes, across all treatments combined, a high proportion of patients (81.8%) classified as absolute PASI=0 (PASI 100) responders at 12 weeks reached DLQI (0,1), indicative of no impact of disease on patients’ lives (Table II). The percentage overlap with DLQI (0,1) responders fell to 67.7% and 63.0%, respectively, for absolute PASI >0 to ≤1 and >1 to ≤2 responders, and continued to gradually decrease with decreasing absolute PASI band ranges (Table II). In comparison, DLQI (0,1) was met by 67.2% of PASI 75 and 73.4% of PASI 90 responders (Table II). For the other HRQoL measures examined, the proportion of patients classified as absolute PASI = 0 responders at 12 weeks who also reached PatGA (0,1) and Itch NRS (≥ 4 improvement) was 96.0% and 94.7%, respectively (Table II). Of the patients with absolute PASI > 0 to ≤ 1 or > 1 to ≤ 2 responses, 86.7% and 80.3%, respectively, were also classified as PatGA (0,1) responders, and > 87% of patients in these absolute PASI categories also had a ≥4-point improvement on the Itch NRS (Table II). How-ever, the degree of overlap between > 2 to ≤ 3 or > 3 to ≤ 5 response and these response criteria was substantially lower at 56.3–67.2% for PatGA (0,1) and 75.0–79.2% for Itch NRS (≥ 4) (Table II).
Table II. Patients who reached relative Psoriasis Area and Severity Index (PASI), static Physician’s Global Assessment (sPGA), and patient-reported outcome criteria at week 12 (NRI) as a percentage of those patients achieving each absolute PASI band (all treatments combined)
Mean absolute DLQI, PatGA, and Itch NRS scores are summarized by absolute PASI band criteria in Table III, and the overall means are plotted relative to absolute band criteria in Fig. 4. Absolute DLQI, PatGA, and Itch NRS scores at week 12 correlated with the absolute PASI criteria, with the impact of skin symptoms on HRQoL rated as less severe by patients in the absolute PASI ≤ 2 categories compared to patients in the absolute PASI > 2 categories (Fig. 4).
Table III. Mean and mean change from baseline in DLQI, PatGA, and Itch NRS at Week 12 (LOCF) by PASI band response (all treatments combined)
Fig. 4. Mean Dermatology Life Quality Index (DLQI), Patient Global Assessment (PatGA), and Itch numeric rating scale (NRS) at week 12 (last observation carried forward (LOCF)) by Psoriasis Area Severity Index (PASI) band response (all treatments combined). DLQI has a possible composite score of 0–30 (least to most impact of skin symptoms on health-related quality of life (HRQoL)). PatGA is scored from 0–5 NRS (clear to severe). Itch NRS is scored from no itch to worst itch imaginable (from 0 to 10) in the previous 24 h. PASI > 5 category includes patients with missing data. Data are from the intention-to-treat population (DLQI, PatGA) or a subpopulation with baseline Itch ≥4 (Itch NRS). N: total number of patients in the analysis population; Nx: number of patients in each PASI band category.
Assessment of the 12-week response by baseline PASI < 20 versus baseline PASI ≥ 20 revealed no differences in the percentage of patients reaching each absolute PASI criterion between the two groups (Fig. 5). Furthermore, when the mean absolute DLQI, PatGA, and Itch NRS scores were assessed by these baseline PASI categories, no consistent differences were observed (Table III).
Fig. 5. Percentage of patients who reached each absolute Psoriasis Area Severity Index (PASI) band criterion at week 12 (non-responder imputation (NRI)) by baseline PASI (all treatments combined). Response has been categorized according to patients with baseline PASI score < 20 or ≥ 20.
Relative PASI response criteria are commonly used in clinical trials and for comparing newer and older treat-ments but have limitations when applied in the daily clinical practice. Treatment goals defined in terms of absolute PASI avoid some of these limitations, but a consensus on the absolute PASI target that is clinically meaningful has not been reached. The current study was conducted to inform this discussion and to evaluate different absolute PASI treatment targets relative to other measures of response based on data derived from two large clinical studies on patients with moderate-to-severe plaque psoriasis.
The ultimate treatment goal for psoriasis is clear or almost clear skin, with many clinicians now advocating robust treatment goals of ≥ 90% improvement over baseline PASI, given the increased efficacy of the newer treatments (2, 6). With respect to PASI 90, the current absolute PASI band analyses showed that both PASI > 0 to ≤ 1 and > 1 to ≤ 2 responder populations exhibited good overlap with the responder populations for PASI 90, as well as for sPGA (0,1). In contrast, the levels of overlap for PASI > 2 to ≤ 3 and > 3 to ≤ 5 responder populations with PASI 90 and sPGA (0,1) were markedly reduced, indicating worse agreement between these criteria. These data suggest that PASI ≤ 2 might serve as a potential alternative treatment goal for patients with plaque psoriasis. In support of this conclusion, compared to other absolute PASI levels, the PASI ≤ 2 response rates for ixekizumab, etanercept, and placebo treatment groups at 12 weeks in this pooled analysis most closely match the PASI 90 response rates previously published on the individual study populations (9).
Further, the current data suggest that absolute PASI values in this range (i.e., ≤ 2) reflect clinically meaningful improvements in the patients’ HRQoL. Not surprisingly, a high proportion of patients achieving absolute PASI = 0 at 12 weeks also reached DLQI (0,1), PatGA (0,1), and Itch NRS ≥ 4, suggesting that skin-related HRQoL improvements were strongly associated with achieving clear skin, which is consistent with previous reports (13−16). Patients showing less than total skin clearance at incrementally higher absolute PASI levels had correspondingly less overlap with the responders on these HRQoL measures, indicating a substantial reduction in patient satisfaction with increasing amounts of residual disease. This inverse relationship between PASI level and HRQoL benefit was also observed between absolute DLQI, PatGA, and Itch NRS scores and absolute PASI band response and is in broad agreement with previous studies, which used a variety of HRQoL measures (13, 17, 18). However, the baseline PASI level (baseline PASI < 20 versus PASI ≥ 20) did not substantially impact PASI response or HRQoL outcomes. These latter findings are in line with our previous report on UNCOVER-2 and UNCOVER-3 integrated populations, which found no differences in PASI response between baseline PASI < 20 and PASI ≥ 20 groups at 12 weeks and 156 weeks when patients were examined by treatment group, indicating a consistent response to treatment regardless of the baseline disease severity (19).
This study has a number of limitations. Notably, as this study used data from clinical trials on moderate-to-severe psoriasis, the study populations were largely homogeneous in terms of baseline demographics and clinical characteristics, including baseline PASI scores. With a mean baseline PASI of 20.29, the strong agreement observed between PASI ≤ 2 and PASI 90 response is to be expected, and examining the absolute PASI in a more heterogeneous patient group with a broader range of base-line PASI values would further improve the evaluation of the absolute PASI treatment targets. An additional limitation of using data from the UNCOVER clinical trials is that all patients met the inclusion criterion of baseline PASI ≥12, but it is not currently known if the findings are relevant to disease activity < 12. A recent prospective observational study using the BioCAPTURE registry, inclusive of patients from clinical practice with baseline PASI scores < 10, has begun to examine this issue; its findings suggest that defining treatment goals in terms of absolute PASI may also have utility in patients with mild disease according to the baseline PASI values (8).
Using data from clinical studies, the current study supports the use of absolute PASI to define treatment goals as it can be used regardless of knowledge of the baseline disease; thereby avoiding some of the limitations of the relative PASI measures. Specifically, the data suggest that for most patients, PASI ≤ 2 is an attainable goal for the treatment of moderate-to-severe plaque psoriasis, on par with PASI 90 in terms of its association with clinical and HRQoL improvements, and may be a clinically relevant choice if the absolute PASI is used instead of the relative PASI.
We thank the patients, their families, and the study personnel who participated in these clinical trials. Eli Lilly and Company (Indianapolis, Indiana, USA) sponsored this study and the production of this manuscript. Syneos Health provided medical writing (Kaye L. Stenvers) and editing (Teri Tucker, Antonia Baldo, Rod Everhart) support.
The study was sponsored by Eli Lilly and Company, Indianapolis, IN.
Conflicts of interest: LP has received consultancy/speaker’s honoraria from and/or participated in clinical trials sponsored by Abbvie, Almirall, Amgen, Baxalta, Biogen, Boehringer Ingelheim, Celgene, Gebro, Janssen, Leo-Pharma, Eli Lilly and Company, Merck-Serono, MSD, Mylan, Novartis, Pfizer, Regeneron, Roche, Sandoz, Samsung-Bioepis, Sanofi, and UCB. CZ has received honoraria for lectures from Eli Lilly and Company, Leo Pharma, Novartis, and Pfizer; has consulted for and participated in advisory boards for AbbVie, Almirall, Amgen, Eli Lilly and Company, Janssen-Cilag, Novartis, and Takeda; and has been a clinical study investigator for AbbVie, Amgen, Boehringer Ingelheim, Celgene, Eli Lilly and Company, Leo Pharma, MSD, Novartis, and Takeda. MD and AL are present or past employees and may be shareholders of Eli Lilly and Company. LB is a consultant for Eli Lilly and Company.


 Click to show fullsize
Click to show fullsize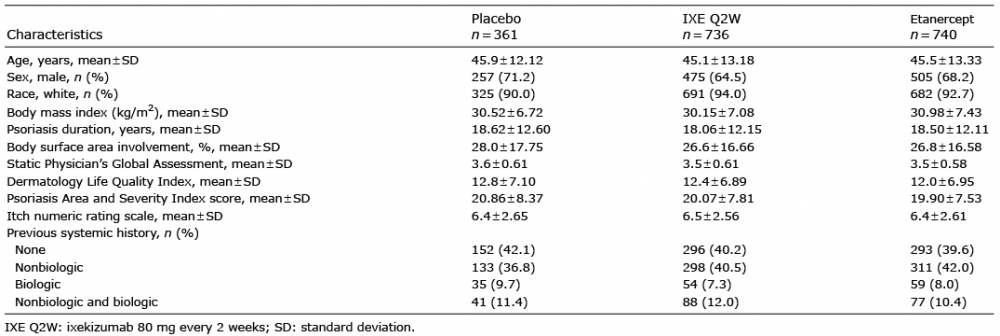 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize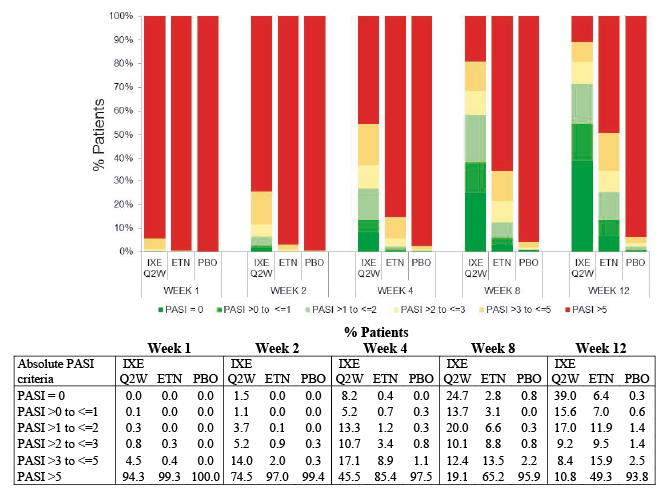 Click to show fullsize
Click to show fullsize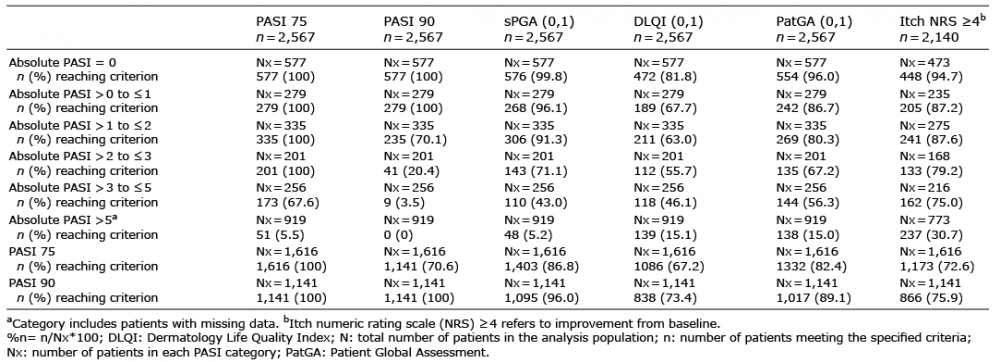 Click to show fullsize
Click to show fullsize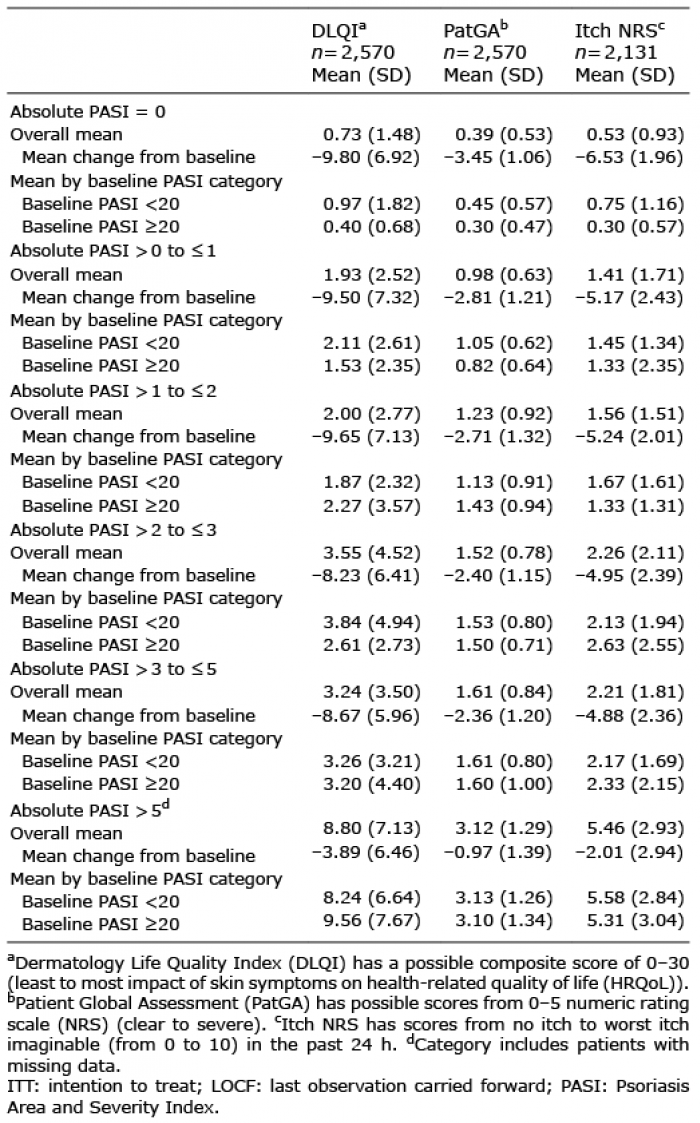 Click to show fullsize
Click to show fullsize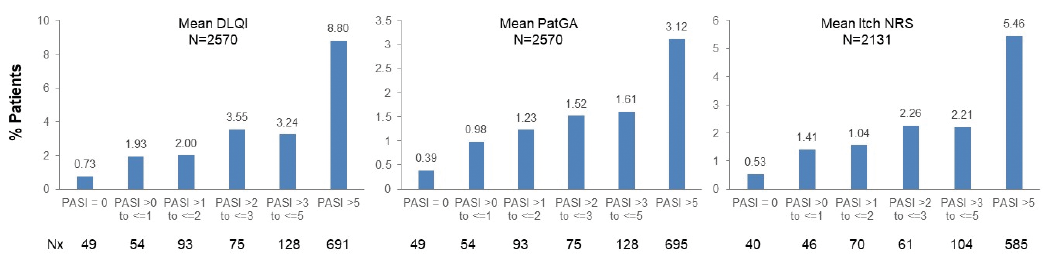 Click to show fullsize
Click to show fullsize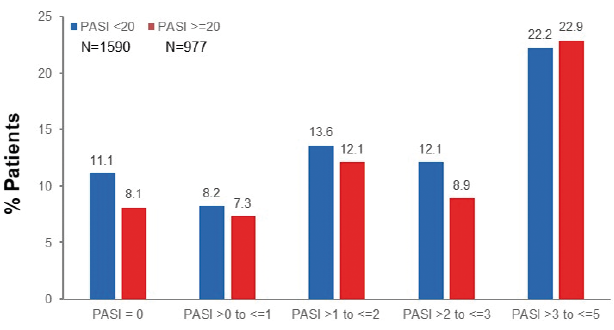 Click to show fullsize
Click to show fullsize