


1Department of Dermatology, Faculty of Medicine, The University of Tokyo, 7-3-1 Hongo, Bunkyo-ku, Tokyo 113-8655, and 2Department of Dermatology, International University of Health and Welfare, Chiba, Japan. E-mail: asahikari1979@gmail.com
Accepted Jun 25, 2019; E-published Jun 26, 2019
Activins, members of the transforming growth factor β superfamily, were originally discovered as reproductive hormones, which stimulate FSH release, and were identified in many tissues. Activins are homo- or heterodimers composed of βA and βB subunits. Among 3 isoforms of activins: activin A (βA/βA), activin B (βB/βB), and activin AB (βA/βB); activin A is the most abundant and best-characterized variant. Activin A has various functions, such as regulating cell differentiation, proliferation, and apoptosis. It has been shown that activin A plays important roles in the development and progression of solid tumors including breast carcinoma (1), ovarian carcinoma (2), and colorectal carcinoma (3). In addition, a recent study has revealed that activin overexpression is an early event in murine and human skin tumorigenesis via attracting tumor-associated macrophages (4). Tumor-associated macrophages are thought to have important roles in progression of not only skin solid tumors but also cutaneous T-cell lymphoma, based on the reports which describe that the depletion of tumor-associated macrophages delays tumor formation of cutaneous T-cell lymphoma cells in skin (5) and that cutaneous T-cell lymphoma patients with an increased number of tumor-associated macrophages had worse prognosis (6). To elucidate activin A involvement in the progression of mycosis fungoides (MF) and Sézary syndrome (SS), we measured serum activin A levels in patients with MF/SS.
Serum samples were obtained from 23 patients with MF (stage IA 6, stage IB 2, stage IIB 12, stage IVA1 1, stage IVA2 2; mean ± standard deviation (SD) age: 59.0 ± 15.1 years; 15 males and 8 females), 6 patients with SS (stage IIIB 2, IVA1 1, stage IVA2 3; mean ± SD age: 71.5 ± 15.9 years; 5 males and 1 female), and 14 normal control subjects (mean ± SD age: 50.8 ± 19.9 years; 9 males and 5 females). All patients with MF/SS were given diagnoses according to International Society of Cutaneous Lymphoma (ISCL)/ European Organization for Research and Treatment of Cancer (EORTC) criteria (7). As for patients with MF/SS, clinical stage IIB or more were defined as advanced stage and clinical stages I and IIA were defined as an early stage. The healthy controls had no history of allergy, atopic dermatitis, psoriasis, or malignancies. The medical ethical committee of the University of Tokyo approved all described studies. Written informed consent was obtained to use the blood samples. Serum activin A levels were quantified by human enzyme-linked immunosorbent assay (ELISA) kits (R&D Systems, Inc., Minneapolis, MN, USA). Significance of difference between two groups was analyzed with Mann-Whitney test and significance of difference among 3 groups was analyzed with Kruskal-Wallis test. Correlation coefficients were determined by using the Spearman’s rank correlation test. Significance of difference in Kaplan-Meier curves was analyzed with Log-rank test. p-values of < 0.05 were considered statistically significant.
Serum activin A levels in patients with MF/SS were significantly elevated compared to those of normal controls (p = 0.012; Fig. 1a). Divided by stages, activin A levels in the sera in patients with advanced stages of MF/SS were significantly elevated compared to those of normal controls (p = 0.004; Fig. 1b), although serum activin A levels in patients with early stages of MF/SS were comparable to those of normal control (Fig. 1b). In sera of patients with MF/SS, serum activin A levels positively correlated with serum soluble IL-2 receptor and lactate dehydrogenase levels (p = 0.005; Fig. 1c, p = 0.014; Fig. 1d), both of which reflect disease severity of MS/SS (8).
Fig. 1. (a) Serum activin A levels in sera of all mycosis fungoides (MF)/Sézary syndrome (SS) (n = 29) patients and those of normal controls (n = 14). p = 0.012 by Mann-Whitney test. (b) Serum activin A levels in sera of stage I or IIA of MF/SS (early stage of MF/SS; n = 8) patients, those of stage IIB or more of patients with MF/SS (advanced stage of MF/SS; n = 21), and those of normal controls (n = 14). p = 0.004 by Kruskal-Wallis test. The measured values from individual patients were plotted by dots. Error bars represent standard error of the mean. (c) Correlation between serum activin A levels and serum soluble interleukin (IL)-2 receptor levels in MF/SS (n = 28). p = 0.005 by Spearman’s rank correlation test. (d) Correlation between serum activin A levels and serum lactate dehydrogenase levels in MF/SS (n = 29). p = 0.014 by Spearman’s rank correlation test.
Next, we performed survival analysis of patients with MF/SS. Kaplan-Meier curves with a cut-off point of 503.3 pg/ml, which was the mean + standard deviation level of normal control, are presented in Fig. 2. As shown in Fig. 2, patients with high serum activin A levels (more than 503.3 pg/ml) had a significantly lower survival rate than those with low serum activin A levels (503.3 pg/ml and less) assessed by Log-rank test (hazard ratio = 4.971, 95% confidence interval = 1.173 to 21.06, p = 0.030).
Fig. 2. Kaplan-Meier survival curve for patients with mycosis fungoides (MF)/Sézary syndrome (SS) with high serum activin A levels (> 503.3 pg/ml, n = 15) and those with low serum activin A levels (≤ 503.3 pg/ml, n = 14). p = 0.030 by Log-rank test.
In this study, we found that serum activin A levels were increased in advanced MF/SS and correlated with disease severity markers such as soluble IL-2 receptor and lactate dehydrogenase levels in the sera. In addition, high serum activin A levels were associated with a poor prognosis. These results imply the possible contribution of activin A to the development of MF/SS. Consistently, the previous report on lung adenocarcinoma shows that upregulated serum activin A levels correlated with more advanced disease stages and associated with a poor overall survival (9). In addition to the lung adenocarcinoma, there are some studies demonstrating that activin A is associated with progression of several solid tumors (1–3). By contrast, its biological and clinical significances in hematological malignancies remain controversial. Activin A was reported to cause apoptosis of myeloma cells and chronic myeloid leukemia cells (10, 11). On the other hand, similar to our results, high expression of βA subunit, which composes activin A, is an adverse prognostic factor for acute myeloid leukemia (12). Considering that activin A can affect tumor progression in an indirect manner, such as inhibiting anti-tumor immunity or attracting macrophages that helps tumor development (4, 13), our results and the previous report suggest that activin A may be associated with progression of some other hematological malignancies in addition to MF/SS. Limitations of this study are the retrospective nature and the small number of patients. In conclusion, we revealed that serum activin A levels were correlated with disease severity and associated with a poor prognosis in MF/SS.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize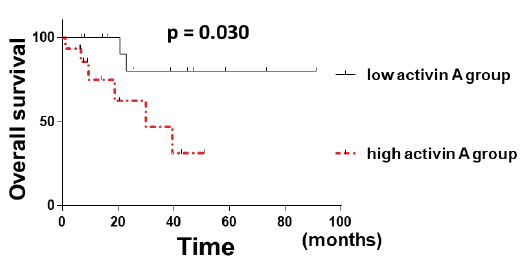 Click to show fullsize
Click to show fullsize