


1Department of Dermatology, Venereology, and Allergology, 5Institute of Pathology and 6Department of Hematology and Oncology, University Medical Center Mannheim, Ruprecht-Karls University of Heidelberg, Theodor-Kutzer-Ufer 1-3, DE–68167 Mannheim, 2Division of Immunogenetics, German Cancer Research Center, 3Section of Clinical and Molecular Dermatology, 4European Center for Angioscience, Medical Faculty Mannheim, Heidelberg University, Mannheim, Germany. *E-mail: jan.nicolay@umm.de
Accepted Jun 28, 2019; E-published Jul 8, 2019
Leukaemia cutis (LC) describes an infiltration of the skin by myeloid or lymphoid blasts, which occurs with variable frequencies in different subtypes of acute/chronic leukaemias and lymphomas (1, 2). Clinical manifestation of LC is highly variable, although erythematous papules and nodules seem to occur most frequently (3, 4). In contrast, ulcerations are a very unusual presentation of LC (1, 5). We present here a rare, and instructive, case of primary extramedullary clinical manifestation of acute myeloid leukaemia (AML) that was unique due to bilateral occurrence of inguinal ulcerations.
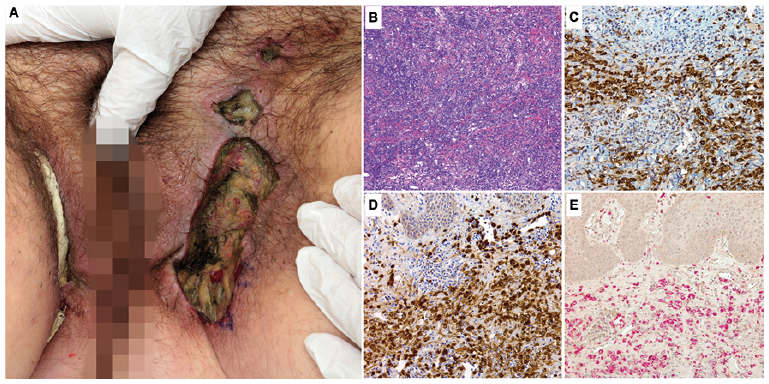
A 54-year-old woman presented to our clinic with extremely painful, malodorous, bilateral inguinal skin ulcerations, progressing for 10 weeks without an obvious trigger or trauma (Fig. 1A). No other skin lesions were detected. Apart from malignant melanoma, stage IA according to the American Joint Committee on Cancer, which was excised 8 years earlier, her medical history was unremarkable. The patient also reported massive fatigue, and weight loss of 4 kg within 2 weeks.
Physical examination revealed extensive, bilateral ulcerations in the inguinal region covered with yellowish-green necrotic tissue presenting with a foul odour (Fig. 1A). Broad-spectrum antibiotic therapy with piperacillin/tazobactam was started immediately. Subsequent microbiological analysis of the ulcer tissue identified the presence of Proteus mirabilis, Morganella morganii and Bacteroides fragilis and all were sensitive to the initiated antibiotic treatment.
Multiple biopsies were taken from the ulcer beds. Haematoxylin/eosin histology revealed mixed inflammatory infiltrates with myelomonocytic blasts (Fig. 1B), as identified by immunohistochemical reactivity for myeloperoxidase (MPO) (Fig. 1C), lysozyme (Fig. 1D), naphthol-AS-d-chloroacetate esterase (Fig. 1E) and CD15. CD3, CD4, CD20, CD34, CD117 and terminal deoxynucleotidyl transferase were negative.
Fig. 1. Clinical picture, histomor-phology and immunohistochemistry of inguinal skin ulcerations as the first presen-tation of acute myeloid leukaemia (AML) before treatment. (A) Initial clinical presentation. (B) Blast infiltration (haematoxylin and eosin (H&E) stain, original magnification: ×100). (C) Myeloperoxidase (MPO) stain (original magnification: ×200). (D) Lysozyme stain (original magnification: ×200). (E) Naphthol-AS-d-chloroacetate esterase (NACE) stain (original magnification: ×200).
Blood analysis revealed severe anaemia (haemoglobin 5.8 g/dl) and thrombocytopaenia (21 × 109/l), the leukocyte count was 6.37 × 109/l with 82% CD33/CD13/cyMPO+ blasts. Consequently, the patient was diagnosed with AML (World Health Organization (WHO) classification: myeloid sarcoma, FAB-classification: M4) (6). The bilateral inguinal skin ulcerations were the first detected manifestation of AML. Blood involvement was confirmed on the day of inpatient admission. A diagnosis of LC was therefore made. The patient was transferred to the Department of Hematology and Oncology, where subsequent bone marrow analyses confirmed blast infiltration (80–90%) with a monocytic differentiation. Next-generation sequencing of a myeloid gene panel revealed somatic mutations in IDH2, KMT2A and STAG2. The karyotype was normal.
A double AML induction therapy with daunorubicin/cytarabine was initiated. Antibiotic therapy was adjusted several times because of sustained fever. During inpatient care, re-analyses of the bone marrow and ulcerations were performed. Post-induction histological examination of the re-biopsied ulcerations and the bone marrow revealed significant reduction of blasts, with a decrease to less than 5% blasts in both respective compartments (Fig. 2A, B). Clinically, cutaneous involvement improved steadily (Fig. 2C). The patient was discharged 2 months after diagnosis of AML. Importantly, the cutaneous involvement healed completely with no surgical intervention (Fig. 2D).
Fig. 2. Course of the clinical presentation, histomorphology and immunohistochemistry of inguinal skin ulcerations (A, B, C) 6 weeks and (D) 28 weeks post-chemotherapy initiation. (A) Haematoxylin and eosin (H&E) stain (original magnification: ×200), (B) naphthol-AS-d-chloroacetate esterase (NACE) stain (original magnification: ×200).
In case of infiltrating myeloid precursors, LC has also been designated as cutaneous myeloid sarcoma (1, 7). Myeloid sarcoma is defined as an extramedullary tumour mass consisting of myeloid blasts (8). In most cases, the enzyme MPO is highly expressed and contributes to a green colour of the tumour mass, which gave the tumour its alternative name chloroma (9). The most frequently detected sites of manifestation include lymph nodes, skin, soft tissues, testes, bone, peritoneum and the gastrointestinal tract (9).
In patients with FAB type M4 and M5 AML, LC occurs in ≥10% of all cases, whereas it is less common in other subtypes and chronic myelogenous leukaemia (10). Importantly, LC has to be differentiated from non-specific, non-leukaemic skin lesions associated with leukaemia, which occur most commonly as a consequence of impaired bone marrow function and/or drug-reactions (1). Non-specific skin lesions involve petechiae, leukocytoclastic vasculitis, opportunistic infections and neutrophilic dermatoses, which are found in over 40% of patients (1). In general, LC is associated with a poor prognosis (1, 5, 7). Besides simultaneous diagnosis of systemic and cutaneous involvement of leukemia, both subsequent development of LC and occurrence of LC prior to systemic involvement have been described (1). So far, only a few cases of ulcerations as a variant of LC have been published (5, 11, 12), which results in a high risk of incorrect or delayed diagnosis. Leukaemic infiltrates can also occur in pre-existing skin lesions, such as pyoderma gangraenosum (13) and traumatically induced leg ulcerations (14).
Although LC typically develops at the extremities, back, chest and head (1), ulcerations that occur due to blast infiltration predominantly seem to affect the genital region (5, 11, 12). However, the inguinal region is a very uncommon site of manifestation (1, 5).
Under chemotherapy, regression and healing of ulcerations induced by infiltrating blasts have been reported (11, 15). Thus, the extensive inguinal skin ulcerations of our patient healed completely during systemic AML therapy without any further intervention. The patient presented here emphasizes the importance of considering haematopoietic neoplasms in the differential diagnosis of primary skin ulcers, in particular those without obvious trigger factors.
The patient gave full permission for the publication, reproduction or other use of data (including photographs) presented in this manuscript. Written patient consent is available on request.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize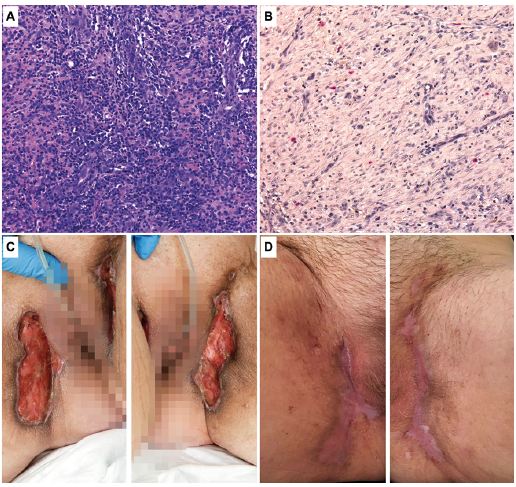 Click to show fullsize
Click to show fullsize