


1Dr Phillip Frost Department of Dermatology, Miami Itch center, University of Miami, Miami, 2Department of Immunology, Eli Lilly and Company, Indianapolis, 3Division of Pharmaceutical Sciences, University of Cincinnati, Cincinnati, OH, and 4Harvard Medical School and Beth Israel Deaconess Hospital, Boston, MA 02215, USA. *E-mail: CLEARS@bidmc.harvard.edu
Accepted Jul 9, 2019; E-published Jul 10
Psoriasis is a chronic disease that is associated with significant disease burden and negative impact on the quality of life of patients. The efficacy and safety of ixekizumab, a high-affinity monoclonal antibody that selectively targets interleukin 17A (1), are well established (2, 3) and patients treated with ixekizumab achieve more rapid improvements, both in health-related quality of life (HRQoL) and itch, compared with patients treated with etanercept (ETN) and placebo (PBO) (4). During the initial 16 weeks of multiple biologic treatment, a strong correlation was reported between reduction in Psoriasis Area and Severity Index (PASI) score and Dermatology Life Quality Index (DLQI) score (5). However, HRQoL may not always correspond to severity of skin disease. Pruritus, an invisible, but tangible, symptom of psoriasis, was identified as an important mediator of the association between improvements in disease severity and HRQoL in ixekizumab-treated patients (6). The present post hoc analysis was therefore conducted to assess the independent, relative effects of early improvements in pruritus (itch) and PASI score on changes in DLQI score using multi-mediator analysis.
In the present analysis, integrated data from UNCOVER-2 and -3 studies (2, 3) on patients with moderate-to-severe psoriasis who received ixekizumab 80 mg once every 2 weeks (IXE Q2W; n = 736) or every 4 weeks (IXE Q4W; n = 733) after the 160-mg starting dose, PBO (n = 361), or ETN 50 mg (n = 740) biweekly through Week 12 were included.
The efficacy end points analyzed at Weeks 4 and 12 were the mean changes in DLQI total score and its domain scores, percentage of patients achieving PASI 75, 90, 100, percentage of patients with a ≥ 4 point reduction from baseline in itch Numeric Rating Scale (NRS: 0 = no itch; 10 = worst imaginable itch in the past 24 h), percentage of patients with a ≥ 5-point reduction in DLQI score, and the percentage of patients reporting itch NRS (0), and itch NRS ≤ 3, and DLQI 0/1 (total score of 0 or 1, indicating psoriasis has no impact on patient’s quality of life) over time with IXE vs. ETN and PBO. Patient reported outcomes were collected using the DLQI and itch NRS at baseline and Weeks 2, 4, and 12 (7, 8).
A mediation analysis with multiple mediators (9) using change in DLQI score from baseline to Week 4 or 12 as the dependent variable and treatment as the independent variable evaluated the effects of change in itch NRS and PASI scores. The total treatment effect on DLQI score improvement over PBO that can be accounted for by changes in itch and PASI score is the ‘indirect’ or mediation effect, while the total treatment effect that cannot be accounted for by the ‘indirect’ effect is called ‘direct’ effect. As a sensitivity analysis, the mediator analyses were also performed for DLQI symptoms and feelings domain as well as DLQI total score without symptoms and feelings domain independently. Cochran-Mantel-Haenszel for categorical variables and mixed effects models for continuous variables were used for treatment comparison. Missing data were imputed using non-responder imputation (NRI) for categorical variables and last observation carried forward (LOCF) for continuous variables.
Overall, integrated data from 2,570 patients (PBO = 361; ETN = 740; and IXE Q4W = 733 and IXE Q2W = 736) were included in this analysis. Details of patient disposition for the induction phases of UNCOVER-2 and UNCOVER-3 have been published previously (2, 3). The patient demographics and baseline characteristics were similar in the treatment groups (Table SI). Treatment with IXE demonstrated significantly greater improvement for all comparisons, except the work and school domains of DLQI for IXE Q4W vs. ETN at Week 12, in PASI 75, 90, 100, DLQI (0,1), no itch (NRS = 0), itch (NRS ≤ 3) and mean changes in itch and DLQI total and domain scores compared to PBO and ETN at Weeks 4 and 12 (Table SII). Pearson correlation analyses showed a significant (p < 0.001 for all comparisons) correlation between PASI score and DLQI score improvements at Weeks 4 (r = 0.38) and 12 (r = 0.43) or correlation between itch NRS and DLQI score improvements at Weeks 4 (r = 0.55) and 12 (r = 0.60).
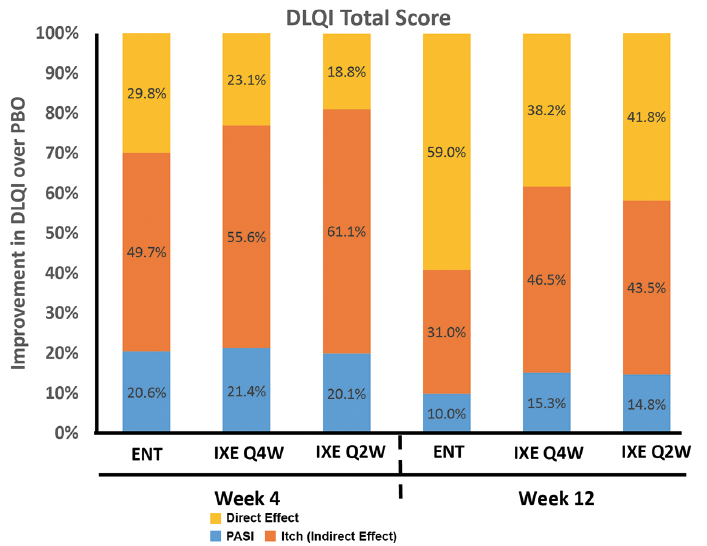
Mediator analysis showed that the major portion of DLQI score improvement at Weeks 4 and 12 with IXE over PBO was attributable to mediating (indirect) effects of itch and PASI scores (Fig. 1). The relative contribution by itch improvement at Week 4 toward DLQI score improvement at Weeks 4 and 12 was 2–3 times higher than that for PASI score. Similar relative contributions to DLQI score improvement by itch and PASI score improvements were observed for the ETN treatment over PBO, even though the overall treatment effect of ETN on DLQI score improvement was significantly less compared to IXE Q2W or Q4W (Fig. 1). Sensitivity analyses of relative contribution to DLQI symptoms and feelings score by itch and PASI score improved showed that itch improvement at Week 4 was more than 3 times higher, compared to PASI in IXE treatment groups. Similar trend was observed in DLQI total score without symptoms and feelings domain between IXE treatment groups and ETN vs. PBO (Figs S1 and S2).
Fig. 1. Relative contribution of itch and Psoriasis Area and Severity Index (PASI) scores on Dermatology Life Quality Index (DLQI) score improvement at Weeks 4 and 12 for Intention-to-treat population. ETN: etanercept; IXE Q2W: ixekizumab 80 mg once every 2 weeks; IXE Q4W: ixekizumab 80 mg once every 4 weeks; PBO: placebo. All data are compared with PBO.
Itch was the most important mediator of improvement in HRQoL compared with PASI, consistent with previous analyses in smaller groups of patients with moderate-to-severe psoriasis (6).
The relationship between DLQI score improvement and improvements in itch and PASI scores has not been well understood. Using the two main disease symptoms, PASI and itch, as the mediators, the mediation analysis showed that both early improvement in itch and PASI scores played a role in improving patient’s quality-of-life at Weeks 4 and 12, with improvement in itch playing a more dominant role than PASI score. Similar results were shown previously in patients with moderate-to-severe psoriasis (6, 10, 11) using a single mediator (6) or more complex models with several factors including PASI, itch, pain, scaling (11). There were limitations in this mediation analysis. First, the mediation analysis serves as a different association analysis in order to quantify the contributions of different mediators to the DLQI improvement. It should not be interpreted in the context of causal relationship between PASI and itch improvements and patient’s quality-of-life improvement. Second, there was still a proportion of total treatment effects on DLQI improvement over PBO that could not be explained by the mediators, which was more evident with ETN treatment. The smaller overall effect of ETN may have increased the variations in modeling the mediation effects; the relative lower contributions of PASI and itch from ETN treatment compared to IXE treatments may also explain the differences. Other factors not considered in the mediation analysis may also contribute to the improvement in patients’ quality of life, which may contribute to the unaccounted-for ‘direct effect’ of the mediation analysis. Further studies to evaluate other mediators could provide more insight in understanding and improving patients’ quality of life for patients with psoriasis.
Results of the present analysis demonstrated superiority of IXE treatment in improving itch and DLQI scores compared to ETN and PBO and showed that the early improvements in itch and PASI scores have considerable impact on DLQI score in patients with moderate-to-severe psoriasis.


 Click to show fullsize
Click to show fullsize