


1Department of Dermatology, Venereology, and Allergology, HELIOS St Elisabeth Hospital Oberhausen, University Witten-Herdecke, DE-46045 Oberhausen, 2Institute of Pathology, Mülheim an der Ruhr, Mülheim, and 3Institute of Virology, National Reference Center for Papilloma- and Polyomaviruses, University of Cologne, Faculty of Medicine and University Hospital of Cologne, Germany. E-mail: a.kreuter@derma.de
Accepted Jul 9, 2019; E-published Jul 10, 2019
Human papillomaviruses (HPV) are amongst the most common sexually transmitted infections. Phylogenetically, HPVs are classified into 5 different genera, called alpha, beta, gamma, mu and nu (1). Approximately 40 HPV-types of the genus alpha predominantly infect the anogenital region and, depending on their oncogenic potential, are divided into low- and high-risk HPV types (1, 2). Alpha-HPV infections can cause a broad spectrum of diseases, ranging from benign genital warts to (pre-)invasive cancer. In contrast to HPV-induced anogenital disease, the association of alpha-HPV infection with squamous cell carcinoma (SCC) of the non-genital skin is a very rare event. Certain digital (particularly periungual) SCCs and SCCs in situ are associated with alpha-HPV infections, especially with HPV16 (3–5). Anogenital–digital spread of high-risk HPV has been suggested to play a role in the pathogenesis of these lesions (6). To date, the association of HPV with SCC or SCC in situ located on the feet has only been reported rarely. We describe here 2 patients with HPV16-induced SCC and SCC in situ of the toes, with significant delay between first clinical appearance and correct diagnosis in both cases.
Patient 1. A 78-year-old Caucasian woman presented with a slowly enlarging verrucous plaque located in the 4th interdigital space of the right foot (Fig. 1A). She reported that she had first noticed the asymptomatic lesion 18 years previously. She had undergone several treatments with topical antifungal and antibacterial creams, without clinical improvement. The patient had no history of trauma, previous HPV-related disease, no exposition to tar, and no previous arsenic or radiation therapy. Besides arterial hypertension and hypothyroidism, her medical history was unremarkable. Inspection of the entire skin, including the anogenital region, revealed no further abnormalities. HIV testing was negative and lymphocyte subpopulations were within the normal range. The patient was a non-smoker. A lesional punch biopsy revealed typical histological features of SCC in situ with focal areas of invasive SCC (Fig. 1B). Maximal depth of penetration of the SCC was 1.2 mm. Immunohistochemical staining for p16INK4a, an indirect marker of high-risk HPV E7-oncogene expression, showed strong nuclear and cytoplasmatic p16INK4a-expression (Fig. 1C). HPV-DNA detection and typing from lesional tissue biopsies were performed with an alpha-HPV group-specific PCR and bead-based multiplex hybridization (7, 8). HPV-DNA load was determined with real-time PCR using type-specific primers and probes (8). The assays revealed infection with HPV16 and a high viral load of 1,893 HPV16 DNA copies per beta-globin gene copy. Surgical excision of the lesion, with a margin of 5 mm, was performed, followed by coverage with a split-thickness skin graft.
Patient 2. A 31-year-old Caucasian woman presented with complete destruction of the nail apparatus of the right hallux is presented in Appendix S1.
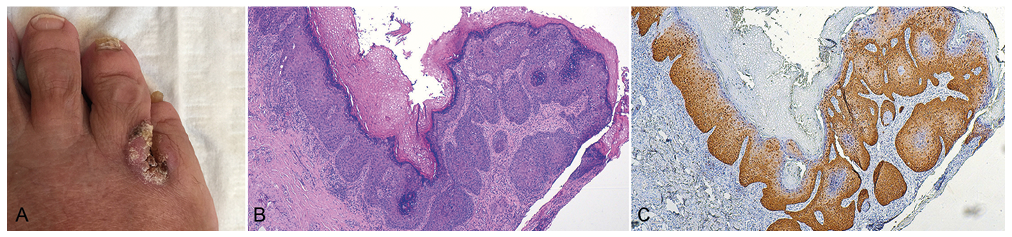
Fig. 1. Patient 1. (A) Clinical findings at first presentation in our department. A verrucous hyperkeratotic plaque with brownish adherent crusts is located in the interdigital space of the right foot, enlarging to the dorsal part of both toes. (B) Histopathological findings of a lesional biopsy. Atypical keratinocytes are present in the entire epidermis, with focal areas of microinvasion into the dermis and moderate accompanying inflammatory infiltrates. These findings are consistent with microinvasive squamous cell carcinoma. The maximal depth of penetration is 1.2 mm (original magnification 100×). (C) Immunohistochemical staining with p16INK4a. Strong nuclear and cytoplasmic p16INK4a-expression is present in the entire epithelium (called p16INK4a-block-staining) and in areas of invasive squamous cell carcinoma. p16INK4a is an indirect marker of high-risk human papillomavirus E7 oncogene expression (original magnification 100×).
Almost all cervical cancers, the vast majority of anal cancers, and approximately half of all vulvar and penile carcinomas, are induced by high-risk alpha-HPV-types. Specific alpha-HPV-types, especially HPV16, are involved in the pathogenesis of periungual SCCs (3, 4). It has been hypothesized that the periungual skin is particularly susceptible to HPV acquisition due to the propensity of the nail unit to abrasion and microtrauma (4). In the largest study so far on HPV-induced digital SCCs and SCCs in situ, including a case series of 23 patients and 51 reported cases from the literature, the majority of lesions (89%) was induced by HPV16 (3). Of the evaluated cases, 10% had antecedent genital dysplasia or carcinoma containing the same HPV type as the digital SCCs, suggesting that anogenital–digital spread is involved in the pathogenesis of these digital lesions.
Previously, a causal role of alpha-HPV-infection in SCCs and SCCs in situ located on the feet was considered unlikely, and other predisposing factors (e.g. genetic aetiology, radiation, exposure to chemicals, trauma, chronic tissue irritation or inflammation) were discussed to be of pathogenetic relevance (9). However, a recent literature review of 36 subungual SCC cases of the toes found an association with HPV in 19.5% of these cases (10). Several of these lesions contained high-risk HPV-types other than HPV16 (e.g. HPV58, HPV56 or HPV45) (11–14). In some cases, the respective HPV-types were found to be integrated into the chromosomal DNA of the tumour cells, as demonstrated by in-situ hybridization, indicating that HPV plays a pathogenetic role in these lesions (12, 13, 15). The high lesional HPV16 DNA loads and the strong p16INK4a-expression found in our 2 patients also argue for a pathogenic role of HPV16 in these cases. The exact mechanism of HPV transmission in HPV-positive SCCs of the feet is unclear. Although HPV-related anogenital lesions were absent in both of our patients, a genital-digital route by auto- or hetero-inoculation from the anogenital area may play a role, as proposed previously for finger lesions (6). In contrast to most other HPV-induced anogenital cancers, immunosuppression does not seem to play an important role in SCCs located on the feet (10).
To the best of our knowledge, only one similar case of interdigital SCC has been reported in the literature. A 46-year-old Japanese woman with a history of concurrent invasive vulvar and cervical carcinomas had polydactylous SCCs in situ located in the 4th interdigital space of the left foot, left thumb, right index finger and both middle fingers. HPV analyses revealed an infection with the high-risk type HPV58 (12).
No standardized therapeutic approach exists for SCC and SCC in situ of the feet, given the rarity of these tumours. The treatment of choice is surgical excision (preferably with a safety margin of 5 mm) and depends on the extent of the lesion. Excision of the complete nail apparatus is advisable for peri- and subungual SCCs, as partial surgical excision of the nail apparatus may result in higher recurrence rates (16). Sentinel lymph node biopsy should be considered in high-risk tumours. Amputation or interphalangeal disarticulation should be restricted to locally advanced, inoperable cases and tumours with bone involvement.
In conclusion, SCCs or SCCs in situ located on the feet are rare keratinocyte tumours. Similarly to digital SCCs, a significant proportion of peri- and subungual tumours of the toes is induced by high-risk HPV. Wide local excision with adequate margin is the treatment of choice. Diagnostic delay is common, as lesions are often confused with benign skin conditions, such as fungal and bacterial infections.
The authors are indebted to Monika Junk, Nabila Ristow, Anke Bartröver, Selina Naujoks and Stefanie Fittkau for their excellent technical assistance.
HPV analyses were funded by the German National Reference Center for Papilloma- and Polyomaviruses (German Federal Ministry of Health, grant 1369-401).
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize