


1Department of Dermatology and Center for Chronic Pruritus, University Hospital Münster, Münster, 2Research & Development, Beiersdorf AG, Hamburg, 3Department of Anesthesiology and Intensive Care Medicine, Faculty of Medicine Mannheim, University of Heidelberg, Mannheim, Germany
Central sensitization induces pain augmentation in chronic pain states. An analogous mechanism is speculated for chronic pruritus. This study compared patients with chronic pruritus (n = 79) of different origins (atopic dermatitis, chronic pruritus on non-lesional skin, chronic prurigo) and healthy controls (HC, n = 54) with regard to itch intensity and qualities of sensory symptoms after selective peripheral nerve fibre activation by electrical stimulation at 5 Hz (surrogate for C-fibre function) and 2,000 Hz (surrogate for Aβ-fibre function) using a Neurometer®. Electrically-induced itch was more intense in patients with chronic pruritus than in HC, but patients with chronic pruritus did not report “itch” more often than HC at 5 Hz. Stimulation at 2,000 Hz induced more pricking and tingling, but less throbbing in patients with chronic pruritus compared with HC. Treatment with cooling compound reduced clinical and experimental itch, but did not alter the distribution of sensory symptoms. These data show hyperknesis in chronic pruritus of various origins, arguing for common central sensitization mechanisms.
Key words: neurometer; electrical stimulation; C-fibre; Aβ-fibre; chronic pruritus.
Accepted Jul 9, 2019; E-published Jul 10, 2019
Acta Derm Venereol 2019; XX: XX–XX.
Corr: Manuel P. Pereira, Department of Dermatology and Center for Chronic Pruritus, University Hospital Münster, Von-Esmarch-Str. 58, DE-48149 Münster, Germany. E-mail: manuelpedro.pereira@ukmuenster.de
Mechanisms underlying chronic pruritus are not yet completely understood. We compared patients with chronic pruritus of different origins (atopic dermatitis, chronic itch on non-lesional skin, chronic prurigo) to healthy controls in regard to itch intensity and sensory symptoms elicited by electrical stimulation. Both stimulation at 5 Hz (targeting C-fibers) and 2,000 Hz (targeting Aβ-fibers) induced a higher itch intensity in patients compared to healthy individuals, regardless of the origin of the pruritus. Additionally diverse sensory symptoms were recorded between patients and controls upon electrical stimulation. These findings argue for common central sensitization mechanisms in chronic itch patients of different origins.
Chronic pruritus is a condition of high complexity with a broad pathophysiological and clinical spectrum (1). In recent years advances in the understanding of underlying neurophysiological pathways have been made. In addition to the role of histamine-sensitive mechano-insensitive C-fibres in itch transmission, it could be demonstrated that heat and mechano-sensitive C-fibres activated by cowhage are also involved in itch signalling (2). In addition, these fibres transmit other sensory symptoms, such as pricking and burning (3). Of note, selective block of myelinated fibres diminishes cowhage-induced itch, arguing for a role of these fibres in non-histaminergic itch processing (4). Unmyelinated C-fibres are associated with the processing of itch and burning sensations, thinly myelinated Aδ fibres with cold and pricking sensations and thickly myelinated Aβ fibres with light touch and vibratory sensations (5). Interestingly, patients with chronic pruritus often report accompanying sensory symptoms, such as burning, stinging or tingling, in addition to the itch (6).
The Neurometer®, commonly used to assess polyneuropathy in diabetic patients (7, 8), is a tool to investigate peripheral fibre function and evoked sensory symptoms. Transcutaneous electrical stimulation at a frequency of 5, 250 and 2,000 Hz aims to assess the function of C, Aδ and Aβ fibres, respectively (9). Accordingly, in previous experiments electrical stimulation at 5 Hz induced itch and pain in healthy individuals (10).
It is well known that central sensitization plays a major role in chronic pain syndromes, contributing to augmenting and maintaining the pain state (11, 12). Analogous to chronic pain syndromes, it is hypothesized that, regardless of the aetiology, central sensitization mechanisms play a role when itch becomes chronic, i.e. when it lasts for 6 weeks or longer (13). In fact, in a previous study on atopic dermatitis patients nociceptive input induced itch rather than inhibiting it, suggesting central sensitization for itch (14). One feature of central sensitization in itch syndromes is the enhanced response to pruritic stimuli, known as hyperknesis. The present study investigated whether stimulation with the Neurometer® at 5 Hz and 2,000 Hz induces more C and Aβ fibre evoked itch in patients with generalized chronic pruritus compared with healthy controls, assuming that hyperknesis and alloknesis would correlate to the level of ongoing pruritus in the patients. We included patients with chronic pruritus on inflamed skin, on non-lesional (normal appearing) skin and with chronic scratch lesions, as well as healthy controls. In addition, we analysed whether a topical antipruritic therapy with an emollient containing a TRPM8-activating cooling compound has an influence on the above-mentioned neurophysiological parameters.
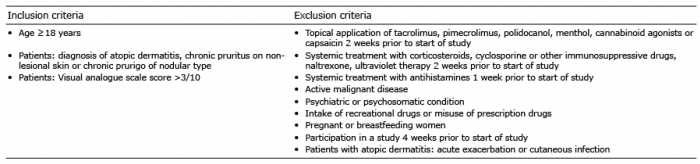
Patients with chronic generalized pruritus presenting at the Center for Chronic Pruritus, University Hospital Münster with atopic dermatitis (AD), chronic pruritus on non-lesional skin (CP) and chronic prurigo of nodular type (PN) were recruited along with healthy controls (HC). Inclusion and exclusion criteria are shown in Table I. The study was approved by the local ethics committee (Medical Faculty of the University Hospital Münster, 2010-179-f-S) and was registered at the German Registry for Clinical Trials (DRKS00005970). Study participants signed an informed consent prior to any study procedures, which were performed according to the Declaration of Helsinki 1975, revised 1983.
Table I. Inclusion and exclusion criteria
This study consisted of two experimental visits, separated by 14 days for patients and one experimental visit for HC.
On day 1 patients’ medical history and skin status were assessed by a dermatologist. The itch intensity (mean, worst; past 24 h) was measured on a numerical rating scale (NRS, 0–10). Subsequently, electrical stimulation using the Neurometer®, both at a frequency of 5 Hz and 2,000 Hz, was performed at the medial aspect of the volar forearm. The stimulations were executed at lesional itchy skin in AD patients, in non-lesional itchy skin in CP patients and in perilesional itchy skin in PN patients.
After the experimental testing of day 1, patients received an emollient with the TRPM8-agonist cooling compound, consisting of a combination of (1R, 2S, 5R)-N-(2-(2-pyridinyl)ethyl)-2-ispropyl-5-methylcyclohexancarboxamide and menthoxypropanediol (15), and were instructed to use the emollient twice daily in the assessment area. On day 14, patients, but not HC, repeated all experimental procedures and assessments as in day 1.
For the electrical stimulation, gel used for ultrasound examinations was applied to the medial aspect of the volar forearm and gold electrodes of 1 cm diameter were attached to the skin. Electrical stimulations were delivered, starting at an intensity of 0 μA, with subsequent increments of 2 μA. Five sets of electrical stimulations at 5 Hz were applied (each stimulation lasting 2 s with an interval of 0.5 s between stimulations). Study participants were instructed to press a button as soon as they perceived the stimulation (current perception threshold; CPT) and were asked to rate the quality of the sensory symptom (pricking, itch, stinging, throbbing, pounding) after each stimulation, as well as the intensity of the perceived pruritus (but not of the other sensations) on the NRS and the urge to scratch. Other sensations (tingling, burning) were also reported by study participants and included in the analyses. In addition, patients were asked to compare the electrically-induced pruritus with baseline pruritus originating from their pruritic condition. Subsequently, electrical stimulation at 2,000 Hz followed in similar fashion, but with intensity increments of 10 μA. Data for the first set of electrical stimulations were disregarded, so that 4 sets of electrical stimulation at 5 Hz and 2,000 Hz were analysed. The mean value of the electrical current required to induce a sensation was calculated as the CPT. CPT values are shown in Neurometer-specific units (NSU), 100 NSU are equivalent to 1 mA. The experimental testing of day 1 was repeated on day 14.
Statistical analysis was performed with SPSS 24.0 (IBM, Armonk, NY, USA). To assess for data normality the Kolmogorov-Smirnov test and Q-Q residual plots were used. Since data was not normally distributed, comparisons between 2 groups were performed (comparisons between study population subgroups) with the Mann–Whitney U test and the Kruskal–Wallis test was used to compare more than 2 groups (patient subgroups). For comparisons across the same individuals (sensory symptoms evoked by electrical stimulation of different frequencies or comparisons between experimental days) the Wilcoxon-test was used. In addition, we performed non-parametric correlation analyses between change in clinical parameters (itch intensity, evoked symptoms) and change in neurophysiological parameters (CPT, evoked itch intensity) across experimental days, correcting for missing data and data sets in which a value of 0 was registered in both experimental days. The level of significance of the statistical tests was set to 0.05. Data are presented as median (interquartile range).
Seventy-nine patients (AD: n = 19, CP: n = 45, PN: n = 15) and 54 HC were included. Demographic data is presented in Table II. A difference in age between patients and HC (p = 0.002) and across patient groups between AD and CP (p = 0.01) was recorded, but not between AD and PN (p = 0.15) or CP and PN (p = 0.35). There were no differences in sex distribution between patients and HC and across patient groups (p > 0.1). At the follow-up visit (V2), 5 patients did not show up (AD: n = 1, CP: n = 3, PN: n = 1) and 2 dropped-out due to side-effects from the therapy (CP: n = 1, PN: n = 1).
Table II. Demographic data
Prior to any experimental procedures, patients reported a median itch intensity of 5.0 [3.0; 6.0], n = 78). No differences were recorded across patient groups (p = 0.87, Table
III). Regarding the worst itch intensity of the past 24 h, we recorded a median score of 9.0 [8.0; 10.0], n = 78) for the overall patient population. CP showed a higher itch intensity compared with PN (p = 0.04), while there were no differences in worst itch intensity between AD patients and the other patient groups (p > 0.1, Table III).
Table III. Itch intensity before and after treatment. Mean and worst itch intensity in the past 24 h were assessed using the numerical rating scale (NRS) before (day 1) and after (day 14) treatment with an emollient with cooling compound applied twice daily
At 5 Hz, evoked itch (patients: 6/78 (7.7%), HC: 7/54 (13.0%)), burning (patients: 7/78 (9.0%), HC: 0/53 (0.0%)), pricking (patients: 41/78 (52.6%), HC: 38/54 (70.4%)), stinging (patients: 18/78 (23.1%), HC: 22/53 (41.5%)), throbbing (patients: 12/78 (15.4%), HC: 5/53 (9.4%)), pounding (patients: 4/78 (5.1%), HC: 4/53 (7.5%)) and tingling (patients: 21/78 (26.9%), HC: 0/53 (0.0%)) was recorded in at least one of the 4 stimulations. Compared with HC, patients reported more tingling (patients: 0 [0;1], HC: 0 [0;0]; p < 0.001) and burning (patients: 0 [0;0], HC: 0 [0;0]; p = 0.026) and less stinging (patients: 0 [0;0], HC: 0 [0;2]; p = 0.03) at a stimulation of 5 Hz. PN reported more pounding than CP patients (p = 0.03), otherwise no differences were observed across patient groups (Fig. 1a).
At 2,000 Hz, evoked itch (patients: 2/73 (2.7%), HC: 1/54 (1.9%)), burning (patients: 3/73 (4.1%), HC: 0/54 (0.0%)), pricking (patients: 22/73 (30.1%), HC: 7/54 (13.0%)), stinging (patients: 8/73 (11.0%), HC: 5/54 (9.3%)), throbbing (patients: 19/73 (26.0%), HC: 31/54 (57.4%)), pounding (patients: 17/73 (23.3%), HC: 16/54 (29.6%)) and tingling (patients: 29/73 (39.7%), HC: 0/54 (0.0%)) was recorded in at least one of the 4 stimulations. Compared with HC, patients reported more pricking (patients: 0 [0;1], HC: 0 [0;0]; p = 0.03) and tingling (patients: 0 [0;3], HC: 0 [0;0]; p < 0.001) and less throbbing (patients: 0 [0;1], HC: 3 [0;4]; p < 0.001) at a stimulation of 2,000 Hz. AD reported more throbbing than CP patients (p = 0.046), otherwise no differences were observed across patient groups (Fig. 1a).
Fig. 1. Sensory symptoms evoked by electrical stimulation. (A) The percentage of patients and healthy controls reporting sensory symptoms (pricking, itch, stinging, throbbing, pounding, tingling or burning) at least 1/4 times after electrical stimulation at a frequency of 5 Hz and 2,000 Hz is shown. Comparing the median of the frequency of sensory symptoms evoked by stimulation at 5 Hz, patients reported more tingling (p < 0.001) and burning (p = 0.03) and less stinging (p = 0.03) than healthy controls. Stimulation at 2,000 Hz evoked more pricking (p = 0.03) and tingling (p < 0.001) and less throbbing (p < 0.001) in patients compared with controls. Solid black: stimulation at 5 Hz in patients; linear black: stimulation at 5 Hz in healthy controls; solid grey: stimulation at 2,000 Hz in patients; linear grey: stimulation at 2,000 Hz in healthy controls. (B) The percentage of patients reporting sensory symptoms (pricking, itch, stinging, throbbing, pounding, tingling or burning) at least 1/4 times after electrical stimulation at a frequency of 5 Hz and 2,000 Hz is shown for experimental day 1 and 14. There were no differences in the median of the frequency of sensory symptoms evoked by stimulation at 5 Hz and 2,000 Hz when comparing measurements in day 1 to day 14. Solid black: stimulation at 5 Hz on day 1; linear black: stimulation at 5 Hz on day 14; solid grey: stimulation at 2,000 Hz on day 1; linear grey: stimulation at 2,000 Hz on day 14.
Patients experienced more intense itch on the NRS evoked by electrical stimulation at a frequency of 5 Hz compared with HC (patients: 2.0 [1.0; 3.3], n = 67; HC: 1.0 [1.0; 2.0], n = 53; p = 0.002), while no differences in itch perception were recorded across patient groups (p = 0.67, Table IV). A minority of the patients (8/76) and HC (4/52) felt an urge to scratch due to the experimental itch and only 3/60 patients (all in the CP group) rated the experimental itch higher than the clinical itch.
Electrical stimulation at 2,000 Hz induced a higher itch intensity on the NRS in patients compared with HC (patients: 2.3 [1.0;3.5], n = 67; HC: 1.0 [1.0; 2.0], n = 51; p = 0.002), while there were no differences in evoked itch intensity across patient groups (p = 0.23, Table IV). Only 9/75 patients and 0/53 HC reported an urge to scratch due to the experimental itch and 4/60 patients (all in the CP group) considered the experimental itch more intense than the clinical itch.
Table IV. Current perception threshold and experimental itch intensity
Electrical stimulation at a frequency of 5 Hz induced more pricking (5 Hz: 1 [0;4], 2,000 Hz: 0 [0;1]; p < 0.001) and stinging (5 Hz: 0 [0;0], 2,000 Hz: 0 [0;0]; p = 0.008) and less throbbing (5 Hz: 0 [0;0], 2,000 Hz: 0 [0;1]; p = 0.008), pounding (5 Hz: 0 [0;0], 2,000 Hz: 0 [0;1]; p = 0.008) and tingling (5 Hz: 0 [0;1], 2,000 Hz: 0 [0;3]; p = 0.002) compared with stimulation at 2,000 Hz in the patient group (n = 73). In HC (n = 53), more pricking (5 Hz: 3 [0;4], 2,000 Hz: 0 [0;0]; p = 0.001) and stinging (5 Hz: 0 [0;2], 2,000 Hz: 0 [0;0]; p < 0.001) and less throbbing (5 Hz: 0 [0;0], 2,000 Hz: 3 [0;4]; p < 0.001) and pounding (5 Hz: 0 [0 ;0], 2,000 Hz: 0 [0;3.5]; p < 0.001) were recorded after stimulation at 5 Hz compared with 2,000 Hz.
At 5 Hz stimulation frequency, the CPT was of 12.8 [8.5;23.4] NSU in patients (n = 78) and 14.6 [8.6;22.9] NSU in healthy controls (n = 54). There were no differences in CPT between patients and HC (p = 0.52) or across patient groups (p = 0.15, Table IV).
As for stimulation at a frequency of 2,000 Hz, a CPT of 105.0 [80.0; 131.9] NSU, n = 78 was recorded for patients and 106.3 [83.1; 141.9] NSU, n = 54 for HC. CPT did not differ between patients and HC (p = 0.69) or across patient groups (p = 0.73, Table IV).
Treatment with the emollient-containing cooling compound induced an improvement in itch intensity assessed at the visit in the overall patient population (day 1: NRS 5 [3;6], day 14: 2.5 [1.0; 4.0]; p < 0.001), as well as in all patient subgroups (p < 0.05, Table III). The worst itch intensity of the past 24 h was decreased after treatment in the overall patient population (day 1: NRS 9 [8;10], day 14: 7.3 [5.0; 9.0]; p < 0.001), and in AD (p = 0.007) and CP (p < 0.001), but not in PN patients (p = 0.11, Table III). At day 14, 11/72 patients expressed an urge to scratch upon electrical stimulation at 5 Hz, while 3/61 (2 CP, 1 PN) considered the experimental itch more intense than the clinical itch. As for the electrical stimulation at 2,000 Hz, 6/68 patients (2 AD, 3 CP, 1 PN) reported an urge to scratch and one patient (PN) evaluated the experimental itch as more intense than the clinical itch.
No differences between day 1 and day 14 were registered when comparing the distribution of sensory symptoms evoked by electrical stimulation both at 5 Hz and 2,000 Hz in the overall patient population and across patient subgroups (p > 0.05; Fig. 1b). CPT evoked by electrical stimulation at a frequency of 5 Hz and 2,000 Hz did not differ in the overall patient population (5 Hz: p = 0.64; 2,000 Hz: p = 0.90) or in any patient group (5 Hz and 2,000 Hz: p > 0.1, Table IV) when comparing assessments performed at day 1 and day 14. In addition, no differences between experimental days were recorded for NRS-scores after electrical stimulation at 5 Hz and 2,000 Hz in the overall patient population (5 Hz: p = 0.79; 2,000 Hz: p = 0.35) or in any patient group (5 Hz and 2,000 Hz: p > 0.1, Table IV).
The change in clinical itch intensity from day 1 to day 14 correlated positively with the change in evoked itch intensity after stimulation with 2,000 Hz (r = 0.50) and negatively with the evoked pain (r = –0.37) in patients with chronic pruritus on non-lesional skin (CP, Fig. 2). Such correlations were not observed for the remaining patients. As for the sensory symptoms evoked by stimulation at 5 Hz, change in evoked itch intensity correlated robustly with stinging (r = 0.77) and negatively with pounding (r = –0.74) and tingling (r = –0.75) in CP patients. In the remaining patients we also observed a positive correlation between the change in evoked itch with stinging (r = 0.85) and a negative correlation with tingling (r = –0.71).
Fig. 2. Correlation between change in clinical itch intensity and evoked itch and CPT. The change in average itch of the past 24 h from day 1 to 14 correlated positively with the change in evoked itch intensity after stimulation with 2,000 Hz (r = 0.50; black dots) and negatively with the current perception threshold (CPT) at 2,000 Hz (r = –0.37; white squares) in patients with chronic pruritus on non-lesional skin. Such a correlation could not be found for the remaining patients. NRS: numerical rating scale; NSU: neurometer specific unit.
In response to peripheral stimuli, the central nervous system is capable of delivering enhanced responses in regard to their intensity, spatial distribution and duration, a phenomenon called central sensitization (11, 12). The role of central sensitization in chronic pain states is well documented. It manifests clinically through hyperalgesia, increased temporal and spatial summation, allodynia, and secondary hyperalgesia, contributing to the transition from acute to chronic pain, and to the maintenance of chronic pain states (11, 12). Central sensitization has been documented in various chronic pain conditions, including fibromyalgia, complex regional pain syndrome, neuropathic pain and post-surgical pain (11). Analogous to pain, central sensitization may play an important role in chronic pruritus conditions (13). Affected patients often report hyperknesis, i.e. enhanced itch sensations to a pruritic stimulus, alloknesis, i.e. itch induced by a stimulus that usually does not provoke itch, as well as spontaneous itch without a triggering stimulus (16), arguing for involvement of central mechanisms. In addition, localized pruritic syndromes may spread beyond the initially localized area, reflecting larger spinal receptive fields that facilitate spatial summation (17).
The current study included patients with generalized chronic pruritus, since central sensitization is more likely to occur in patients in whom itch has spread to the whole body. We hypothesized that electrical stimulation at 5 Hz and 2,000 Hz would target mainly C and Aβ fibre associated sensory symptoms, respectively, in patients with chronic pruritus of various origins compared with healthy controls. As the electrical stimulation of the axons is not affected by possible peripheral sensitization of sensory endings, the result should mainly reflect central sensitization. Peripheral sensitization of the sensory ending will increase sensitivity to natural stimulation that requires the transduction process. In contrast, the axonal depolarization and subsequent induction of action potentials does not involve transduction at the sensory endings. Thus, our electrical stimulation of axons will skip the transduction process residing in the sensory nerve endings and consequently, the evoked action potentials will be independent of potential sensitization of the peripheral sensory endings. However, we cannot exclude that peripheral sensitization might also have included axonal proteins including voltage sensitive sodium channels, as shown, for example, following dermal injection of nerve growth factor in humans (18). In this case our electrical skin stimulation could be modified by peripheral “axonal sensitization”.
As expected, electrically-induced itch after stimulation at both 5 Hz and 2,000 Hz was more intense in patients compared with controls, showing hyperknesis. However, only a minority of patients felt an urge to scratch (5 Hz: 8/76 patients, 4/52 controls; 2,000 Hz: 9/75 patients, 0/53 controls). Interestingly, there were no differences in evoked itch intensity across patient groups, suggesting that central sensitization in patients with generalized pruritus are primarily independent of the underlying aetiology. Accordingly, CPT did not differ between patient groups both after electrical stimulation at 5 Hz and 2,000 Hz. Differences were detected between patients and controls regarding the C-fibre-associated sensory symptom burning after stimulation at 5 Hz, but not regarding itching, another C-fibre-associated sensation. These findings may result from an overall scarce induction of itch (and burning) with this experimental setup. For stimulation at 2,000 Hz, we observed more pricking and tingling, but less throbbing in patients compared with controls, suggesting a possible central involvement. The applied frequency of 2,000 Hz is far beyond the following frequency of both Aβ and Aδ-fibres, and therefore the reported sensory symptoms, especially the pricking sensation, are most probably linked to Aδ-fibres.
When the stimulation frequency is reduced to 5 Hz, activation of C-fibres is anticipated. However, for selective C-fibre stimulation in human skin, higher current density with small bipolar electrodes is required (19). Patients reported more throbbing, pounding and tingling after stimulation at 2,000 Hz compared with stimulation at 5 Hz. However, stimulations at 5 and 2,000 Hz did not differ in their ability to cause itch and burning, 2 sensory symptoms transmitted by C-fibres confirming the limited specificity of the surface electrodes. Looking at the absolute values, however, a higher percentage of patients reported itch (7.7% (5 Hz) vs. 2.7% (2,000 Hz)) and burning (9.0% (5 Hz) vs. 4.1% (2,000 Hz)), while more controls reported itch (13.0% (5 Hz) vs. 1.9% (2,000 Hz)) after electrical stimulation at 5 Hz compared with 2,000 Hz, supporting that these sensations are associated with C-fibre activation.
The role of Aβ-fibres in itch transmission is still disputed. In fact, recent experiments on a psoriasis mouse model suggest that a reduction in Aβ-fibres might contribute to a disinhibition of mechanical itch (20). In the current study only a minority of patients (2.7%) and controls (1.9%) reported itch after electrical stimulation at 2,000 Hz. A concomitant activation of other nerve fibres cannot be ruled out with the experimental setup used, and may have contributed to the sensation of itch in these patients. Interestingly, myelinated fibres seem to play a role in the transmission of scratch-induced pleasurability. Following compression nerve block of Aβ and possible Aδ-fibres myelinated fibres, the pleasurable sensation of scratching was reduced in healthy subjects, who were stimulated with cowhage (21). While our study focused on the transmission of sensory symptoms upon selective nerve fibre activation, future studies should investigate the role of specific myelinated fibres in scratch-induced pleasurability in patients with chronic pruritus.
Treatment with an emollient with cooling compound showed an antipruritic effect in all patient groups. The itch intensity evoked by electrical stimulation, as well as CPT, did not differ when comparing scores before and after treatment when analysed independently of spontaneous itch levels. However, when analysing changes in clinical itch severity, electrical stimulation induced weaker itch in those patients who showed a reduction in their clinical itch. Thus, reduction in clinical itch severity between experimental days correlated with the reduction in evoked itch intensity after stimulation with 2,000 Hz, and negatively with the perception threshold in patients. On the one hand, these results reflect the close relationship between ongoing pruritic activity for the maintenance of central sensitization. Even in patients without obvious cutaneous inflammation, restoration of the barrier by treatment with emollient appears to reduce such pruritic input. Pruritic input from non-lesional skin might appear to be of minor pathophysiological importance; however, barrier impairment and xerosis is closely linked to systemic diseases leading to CP, such as renal failure (22), hepatobiliary conditions (23) or advance internal malignancies (24). Moreover, it is important to note that we have learned from patients with chronic pain that, even if the pathophysiology is restricted to the central nervous system, such as post-stroke pain, modulation of the peripheral input can still block ongoing pain (25). Thus, topical anti-pruritic treatment appears promising even if the main pathophysiological process is systemic.
Patients and controls in this study were not matched for age and sex. However, this limitation does not affect the interpretation of the results, since only a few study participants reported itch evoked by electrical stimulation, and thus hyperknesis in patients with chronic pruritus as a reflection of central sensitization could not consistently be shown with this experimental setup.
Central sensitization may play a role in chronic pruritic conditions by enhancing itch perception and other sensations. In our study sensory symptoms arising from selective peripheral fibre activation by electrical stimulation were only partially enhanced in patients with generalized chronic pruritus compared with controls. Alternative experimental setups may be needed to consistently show the effects of central sensitization after peripheral stimulation of different nerve fibres in chronic pruritus. Future experimental studies should further investigate central sensitization in patients with chronic pruritus.
This paper presents partial data from JK’s “doctor medicinae dentum” degree thesis.
This article was supported by Beiersdorf and a grant from the German Research Foundation to KA, MS and SST (DFG; FOR2690). The funding sources played no role in the definition of the study design, in the collection, analysis and interpretation of data, in the writing of the report, or in the decision to submit the article for publication.
Conflicts of interest: GN is an employee at Beiersdorf AG. SST has served on the advisory board of Beiersdorf AG and received equipment employed in this study from Beiersdorf AG.


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize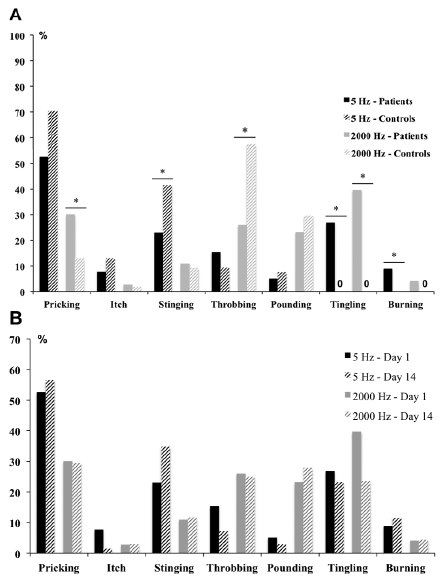 Click to show fullsize
Click to show fullsize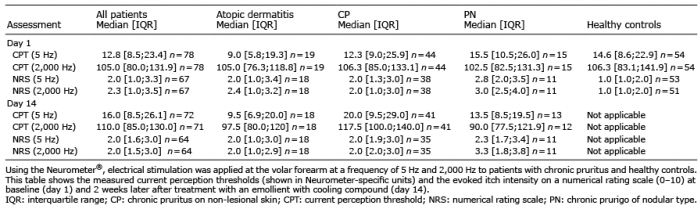 Click to show fullsize
Click to show fullsize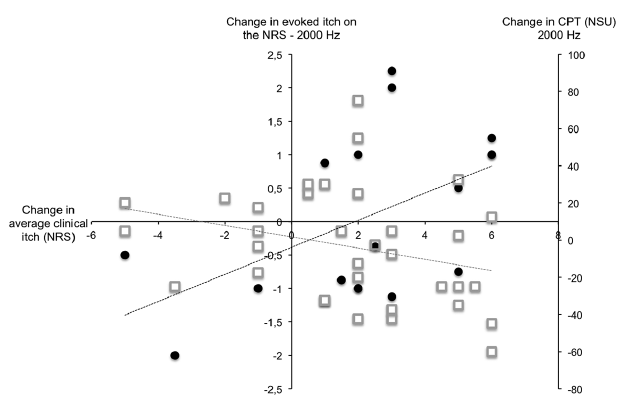 Click to show fullsize
Click to show fullsize