


1Department of Dermatology, Sheba Medical Center, Sackler School of Medicine, Tel Aviv University, Tel Aviv, 2Department of Dermatology, Hadassah-Hebrew University Medical Center, Kiryat Hadassah, and 3Department of Radiology, Shaare Zedek Medical Center, Jerusalem, Israel
#These authors contributed equally to this paper.
Vascular anomalies (VAs) may be associated with significant morbidity and mortality. The aim of this study was to evaluate the efficacy and safety of sirolimus (rapamycin) in the treatment of children and young adults with complicated VAs. A retrospective chart was created that included 19 patients treated with sirolimus for complicated VAs. Concurrently, a search of the PubMed database for VA cases treated with sirolimus was conducted. Descriptive analysis was performed and the efficiency rate of sirolimus was calculated. This retrospective study included 19 patients, 17 of whom were treated with oral sirolimus and 2 with topical sirolimus. Clinical improvement occurred in 15 patients (79%). One patient experienced near-complete resolution. Only 2 patients showed poor response and discontinued treatment. The literature review analysed 150 cases of VA treated with sirolimus. Sirolimus was efficient in 85% of cases, including 5 cases of complete resolution. Sirolimus appears to be an effective and safe treatment for children and young adults with complicated VAs.
Key words: sirolimus; rapamycin; vascular anomalies; vascular malformation.
Accepted Jul 12, 2019; E-published Jul 12, 2019
Acta Derm Venereol 2019; XX: XX–XX.
Corr: Shoshana Greenberger, Department of Dermatology, Sheba Medical Center, Tel Hashomer, Ramat Gan, Israel. E-mail: Shoshana.greenberger@sheba.health.gov.il
In recent years, sirolimus, an mTOR inhibitor, has become a new therapeutic option for patients with vascular anomalies that do not respond to other treatments. We report here a retrospective series of 19 young adults, children and neonates with complex vascular anomalies treated with sirolimus. Overall, clinical improvement was demonstrated in 15 patients (79%). In addition, an up-to-date literature review was performed and 150 cases of vascular anomalies treated with sirolimus were analysed. The results suggest that sirolimus is an effective and safe treatment. Further study is needed into the early use of sirolimus in cases of low-flow lesions, and overgrowth syndromes with low-flow components.
Vascular anomalies (VAs) are a heterogeneous group of disorders originating from blood and/or lymphatic vessels that are further classified as either vascular malformations (VMs) or vascular tumours (VTs) (1). VTs are thought to result from endothelial proliferation. They include infantile and congenital haemangiomas, tufted angiomas and kaposiform haemangioendotheliomas (KHE) (2). In contrast, VMs are anomalies resulting from abnormal embryonic morphogenesis of blood and/or lymphatic vessels and have a normal endothelial cell turnover. They are described by the abnormal vessel type(s). VMs are generally present at birth; they enlarge through expansion that is proportionate to the child’s growth, as well as in response to infection, hormonal changes or trauma (3–5).
Although the majority of VAs are benign and cause minor symptomatology, some may be associated with complications. Growth and/or expansion of VAs can cause clinical problems, such as disfigurement, chronic pain, recurrent infections, coagulopathies, organ dysfunc-tion and death. Individuals often experience progressive clinical symptoms with a worsening quality of life (6).
Treatment of VAs is largely based on symptoms, and no therapy is suggested as a first possibility. Historically, VMs have been primarily treated by procedural interventions to achieve local control, such as excision, embolization, sclerotherapy, debulking and pulsed dye laser. In contrast, treatments of VTs have been based mostly on medical therapy; infantile haemangiomas are mostly treated with propranolol when indicated, whereas other VTs might be treated with steroids, vincristine, interferon, chemotherapeutic agents or radiotherapy or surgery (7, 8). Nevertheless, some of these complicated VAs are refractory to the above-mentioned treatment modalities. In these cases, rapamycin (mTOR) inhibitors are found to be more promising (9–16).
mTOR is a serine/threonine kinase regulated by phosphoinositide 3 kinase (PI3K) and protein kinase B (Akt). The PI3K/AKT/mTOR pathway acts as a master switch on numerous cellular processes, including cellular catabolism and anabolism, cell motility, angiogenesis and cell growth (17). Enhanced mTOR signalling increases expression of the vascular endothelial growth factor (VEGF), a key regulator of angiogenesis and lymph-angiogenesis (18). Disorders that lead to inappropriate activation of the PI3K/AKT/mTOR pathway result in tissue overgrowth in association with VAs (6). mTOR inhibitors, such as sirolimus, directly inhibit mTOR, therefore blocking downstream protein synthesis and subsequent cell proliferation and angiogenesis (17).
Sirolimus is effective for treatment of VAs in syndromes with an upregulated mTOR activity, specifically for hamartomas in patients with PTEN mutations (19–21), VTs in patients with tuberous sclerosis (22) and in patients with lymphangioleiomyomatosis (LAM) (23, 24). Given its effectiveness in these conditions, sirolimus was initially tried as a VA treatment in a patient with refractory KHE with Kasabach-Merritt phenomenon (KMP) (25). This patient had a rapid and dramatic response to sirolimus treatment. Since this initial success, the use of sirolimus has expanded rapidly (8). While initially explored for KHE and lymphatic malformation (LM) (26–28), sirolimus is now being used broadly throughout the VA spectrum and is showing promising results in both systemic administration (10, 29–31) and topical administration (32–34).
Sirolimus opens the era of targeted molecular therapy for complicated VAs (35, 36). The discovery of mutations that upregulate the PI3K/Akt/mTOR pathway and result in VAs, such as PTEN (37), PIK3CA (38, 39), TIE2 (40), RASA1 (41) and NRAS (42), provides the molecular rationale for mTOR inhibition in many of the VA disorders and sets the stage for targeting genes and pathways involved in VAs to be developed (6).
In recent years, several case reports (11, 15, 43–48) and retrospective case series (12, 14, 29, 49–52) have been published on the use of sirolimus for the treatment of VAs, with positive results. Following these publications, sirolimus was further evaluated in a phase II study of 60 patients with complicated VAs, with clinical improvement in most patients and with tolerated adverse effects (6). However, an up-to-date literature review that addresses these publications, characterizes clinical features and assesses the efficacy and safety of sirolimus for different VAs, is lacking.
Therefore, the objective of this study is to evaluate the efficacy and safety of sirolimus in the treatment of children and young adults with complicated VAs. We present here a series of young adults, children and neonates with complex VAs treated with sirolimus in 3 medical centres in Israel, and a literature review.
A retrospective review was performed on 19 cases of complicated VAs treated with sirolimus between March 2013 and December 2017. Fifteen patients were treated at the Sheba Medical Centre, 3 were treated at the Hadassah Medical Centre, and one was treated at the Shaare Zedek Medical Centre. Oral sirolimus was administered to 17 patients, while topical sirolimus was administered to 2 patients. The systemic treatment regimen initially consisted of oral 0.6 mg/m2 sirolimus twice daily, which was then titrated to reach a target level of 5–12 ng/ml. The topical treatment regimen consisted of a twice daily application of 0.2% sirolimus gel. A positive response to treatment was defined as a clinical/radiological stabilization or a decrease in lesion size, overgrowth, malformation weeping and/or bleeding, decreased number of thrombosis events, resolution of transfusion requirements, decreased number of cellulitis episodes, improvement in quality of life and/or functional impairment and a reduction in pain, as reported by the patients. A partial response was defined as an improvement in the symptoms and a reduction in the lesion, but a persistence of the anomaly. A complete response was defined as a resolution of symptoms and lesion. Laboratory parameters that were monitored included, but were not limited to, complete blood count (CBC), liver function tests, serum creatinine and lipid profile. Appropriate imaging studies were obtained throughout the study, when indicated. The case series, with review of the medical record, was approved by each Institutional Review Board.
Concurrently, a review of the literature was performed using the MEDLINE database via PubMed for publications on sirolimus treatment for VAs, without date or language limitations. The following key words were used in various combinations: ”rapamycin”, ”sirolimus”, ”mTOR inhibitor”, ”vascular”, ”malformations”, ”tumours”. The inclusion criteria were: English language and the relevance of the title or abstract to the field of research, including VTs and VMs treated with systemic sirolimus in humans. Exclusion criteria were: studies describing single patient case reports, malignant tumours, sirolimus administered in the form of neoadjuvant/adjuvant therapy and topical treatment. For each selected report, the following variables were considered: year and country of publication, journal, study design, number of cases described, sex and age of the patients, symptoms, type of the VA, treatment (including dosage and target serum level, efficacy, toxicity) and follow-up. Subsequently, a descriptive analysis was performed. Since efficacy criteria were heterogeneous, sirolimus treatment was considered to be efficient if the authors reported it as such. The efficiency rate (calculated as the percentage of patients who had a positive response to Sirolimus treatment out of the total number of patients receiving Sirolimus treatment) of sirolimus was then calculated. Two reviewers first selected the studies and then extracted and classified the data. Another independent reviewer checked the selection and the data classification.
Patient characteristics
Nineteen patients with different VAs were included in this report. Eighteen had malformations: congenital, lipomatous, overgrowth, vascular malformations, epidermal naevi and spinal/skeletal anomalies and/or scoliosis (CLOVES) syndrome n = 2, Klippel-Trenaunay syndrome (KTS) n = 5, Parkes-Weber syndrome (PWS) n = 1, combined lymphatic-venous malformation (LVM) n = 2, lymphatic malformation (LM) n = 4, blue rubber naevus syndrome (BRBNS) n = 1, arteriovenous malformation (AVM)/PTEN n = 1, generalized lymphatic anomaly (GLA) (n = 2), and 1 patient had VT (unknown n = 1). Male predominance (2.17:1) existed, and the mean age at the time of treatment initiation was 6.2 years (range 0.5–322 months). Thirteen patients (68%) were pre-treated prior to sirolimus, all with at least 1 surgical or interventional procedure performed. Although some of the patients had shown a partial response to prior interventions and medical therapy, all patients continued to experience debilitating or life-threatening complications, including chronic pain (79%), overgrowth (42%), coagulopathies (37%), recurrent cellulitis (16%), secretions (26%) and organ dysfunction (37%).
Response
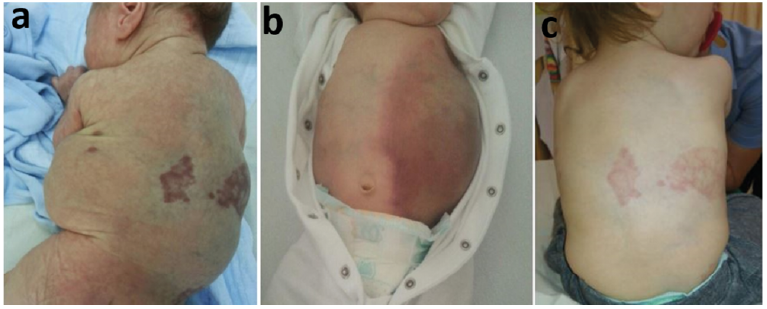
Clinical improvement was demonstrated in 15 patients (79%) and included an improvement in pain level, size of VAs, secretion, as well as decreased cellulitis and thrombosis events. One patient (Patient 1) with CLOVES had a nearly complete resolution of cystic lesions and overgrowth, as shown in Fig. 1. Only 2 patients (Patient 7 with KTS and Patient 8 with PWS) had shown a poor response to overgrowth and discontinued treatment. Two patients with GLA (Patients 17 and 18) had a partial response expressed in respiratory stabilization for several months, before further deterioration due to their underlying disease. Patient 18 eventually died from respiratory failure while on sirolimus treatment. The mean initial response time was 1.5 months (range 10–90 days), except for Patient 14, for whom data were not available, and for Patients 7 and 8, who showed no response. The mean follow-up time was 19.42 months (range 1.5–60 months). Fourteen patients (74%) discontinued treatment with sirolimus during follow-up. In 10 of these patients (71%), exacerbation was demonstrated after discontinuing sirolimus treatment, whereas improvement was evident following the renewal of it. In total, 15 patients are now on continuous sirolimus treatment and 1 patient (Patient 10) is on pulse therapy, as needed. Details of the sirolimus treatment courses are shown in Table I.
Fig. 1. Patient 1. (a) The boy presented at birth with extensive lymphatic-venous vascular malformations (VMs) in both lateral chest walls and limb overgrowth and was diagnosed with Congenital, Lipomatous, Overgrowth, Vascular malformations, Epidermal naevi and Spinal/skeletal anomalies and/or scoliosis (CLOVES) syndrome. (b) At the age of 7 weeks, a life-threatening episode had occurred with enlargement and bleeding into the VM, requiring red blood cell transfusions and sclerotherapy. Sirolimus was introduced at the age of 2 months. (c) After 22 months of sirolimus treatment he had a nearly complete resolution of cystic lesions and overgrowth.
Table I. Result of sirolimus treatment in 19 patients with complicated vascular anomalies
Toxicity
Adverse effects observed in this study were consistent with expected sirolimus toxicities. Sirolimus toxicities were graded according to the Common Terminology Criteria for Adverse Events. Observed effects included Grade I hypercholesterolemia (n = 3), Grade I–III hypertriglyceridaemia (n = 2), Grade I elevation of liver enzymes (n = 4), Grade I mouth sores (n = 1), Grade I thrombocytopaenia (n = 2) and Grade I abdominal pain and nausea (n = 1). In addition, adverse effects that are possibly attributable to sirolimus treatment included thrombocytosis (n = 2), Grade III hyperkalaemia (n = 1), perianal abscess (n = 1) and buttocks abscess (n = 1). Six patients experienced bacterial infection during treatment, including cellulitis (n = 4), pneumonia (n = 1) and methicillin-resistant Staphylococcus aureus (MRSA) bacteraemia (n = 1). One patient developed an opportunistic cytomegalovirus (CMV) infection (n = 1). Only 2 patients interrupted sirolimus therapy due to adverse events possibly attributable to sirolimus treatment; one experienced hyperkalaemia and the other an elevation of liver enzymes. Both of them resumed sirolimus therapy shortly after stopping. Four other patients had brief interruption of sirolimus treatment due to intercurrent febrile disease. All other adverse events were managed without treatment interruption. None of the patients developed neutropaenia during follow-up.
Literature review
Of the 304 articles identified in the literature search, 7 retrospective case series (13, 15, 29, 41–44) and 1 phase II study (7) were included, corresponding to 90 and 60 patients, respectively. Sex distribution included 73 (49%) females, 58 (38%) males and for 19 patients (13%) the sex was not reported. Regarding the age at which sirolimus treatment began, no data on compatible stratification were available for 101 patients and therefore we referred to the median age as reported. The majority of patients (80%) started sirolimus treatment between 2–13 years of age. Among the VAs presented in this review, 19% (n = 29) were VTs, mostly KHE/tufted angioma, and 81% (n = 121) were VMs, mostly LMs. All patients had severe symptoms before sirolimus treatment was started, which were detailed in 49 cases: 17 (35%) had coagulopathies, 13 (27%) experienced organ dysfunction, 9 (18%) had chronic pain, 4 (8%) had overgrowth, and 7 (14%) had recurrent cellulitis.
Oral sirolimus treatment was administered to all patients. A starting dose of sirolimus, 0.8 mg/m2 twice daily, was administered orally to most patients (96%), while for the remaining 4% the starting dose was 0.05 mg/kg twice daily. The sirolimus target serum level was heterogeneous. In 62% of patients the levels were maintained between 10 and 15 ng/ml, in 8% the target level was 5–15 ng/ml and in 27% data were not reported. Most of the patients reported in this review (72%) were still taking sirolimus at the end-point of each study. Sirolimus therapy was withdrawn in 40%. Of these, 30% had worsened after the withdrawal and therefore re-started therapy.
Criteria considering the efficacy of the treatment were variable and included clinical, radiological, laboratory, quality of life related or combined criteria. Clinical criteria were diverse and included a stabilization or decrease in the lesion size, a reduction in transfusion requirements, an improvement in pain level, decreased events of cellulitis, and improved vital functions. The most common radiological evaluation was magnetic resonance imaging (MRI) performed according to a standardized protocol. Computer tomography (CT) scans and radiographs were also considered for efficacy criteria. Laboratory criteria included haemoglobin, platelets, fibrinogen and D-dimer levels. Health-related quality of life (HRQoL) was assessed using scales, mostly the Paediatric Quality of Life Inventory 4.0. In this review, sirolimus was found to be efficient in 85% of cases, including 5 cases of complete remission (CR). The median response time was 7.9 weeks (range 1–90 weeks) for 59 cases, while in 91 cases the data were not reported.
Overall, in this review sirolimus was well tolerated with easily manageable adverse effects. The most commonly reported adverse effects attributed to the sirolimus treatment included gastrointestinal (28%), blood/bone marrow (22%), metabolic/laboratory (16%) and mucositis (13%). Only 6 patients (4%) interrupted treatment due to adverse effects, which included neutropaenia, elevation of liver enzymes, nausea interfering with the quality of life, persistent lymphoedema, a brief interruption for intravenous (IV) antibiotics and associated alopecia, each in a single patient. Four of these patients resumed treatment after stopping sirolimus therapy. The characteristics and responses of 150 patients included in this review are shown in Table II.
Table II. Review of literature: characteristics and response of patients treated with sirolimus for complicated vascular anomalies
This study is a retrospective case series report on the use of sirolimus for the treatment of complicated Vas, and a literature review. Data were assessed for 19 patients and for 150 patients, respectively. To the best of our knowledge, this paper is the largest review study referring to the use of sirolimus treatment for VA, with the aim of characterizing the demographics and clinical features of the patients, as well as assessing the sirolimus treatment efficacy and safety in different VAs.
In this retrospective study, more favourable responses to sirolimus were seen in younger patients. Five patients (26%) started sirolimus treatment before the age of 2 months. All 5 patients had a good response to sirolimus treatment. Dramatic response was demonstrated in 4 patients, including a nearly complete resolution in 1 patient with CLOVES syndrome. In our literature review, 5 patients reported starting with sirolimus treatment before the age of 2 months. All had a good response to sirolimus, with 3 of them achieving complete remission. Sirolimus was also very efficient in a group of young patients (n = 15) who started therapy between the ages of 2 months and 2 years, with 100% partial response and 1 complete response. Furthermore, it was previously suggested that younger patients may respond better than older patients (7, 15). Our experience also suggests that the early use of sirolimus should be considered in order to reduce morbidities associated with the VAs, invasive interventions and to improve prognosis.
In our retrospective study, 79% of patients (n = 15) with VAs exhibited beneficial overall responses to sirolimus, including patients with CLOVES syndrome, KTS, LMs, LVMs, unknown tumour, BRBNS and AVM/PTEN. Patients who showed no response included one patient with KTS and one patient with PWS. Two patients with GLA showed temporary stabilization, followed by progression of their underlying disease. In the literature review, sirolimus treatment was effective in 85% of cases, including KHE, tufted angioma, VMs, BRBNS, LMs, LVMs, CLVM, PTEN/AVM, GLA and GSD. Most of the VAs that responded to treatment had a lymphatic component, including a novel finding of a lymphatic component in 4 cases of BRBNS (41). However, 11% of cases showed no response to treatment/progressive disease, including AVM, VM, GSD, LM, KLA, lymphangiectasia/abnormalities of the central conducting lymphatic channels and unknown tumour. Good response to sirolimus was previously reported in literature for many cases of the VAs, including KHE, LM, LVM, CLVM, GLA and GSD. There had been mixed results concerning VMs and AVMs, as the result of this review confirms. It is therefore evident that some VAs, mainly low-flow lesions, overgrowth syndromes with low-flow components, and VAs that demonstrate upregulation of the mTOR pathway, respond to sirolimus treatment in most cases, probably due to inhibition of lymphatic expansion and soft-tissue overgrowth. However, some VAs seem to respond poorly. Hence, it is clear that further studies are needed to identify high-risk VA patients presenting with specific disease phenotypes and/or genotypes, in whom sirolimus treatment may be effective.
In this literature review, oral sirolimus therapy was administered to all patients. In our retrospective review, 17 of the patients were treated orally, while 2 were treated with topical sirolimus (KTS n = 1, LVM n = 1). The 2 cases treated with a topical application of sirolimus responded very well, probably due to the presence of superficial lymphatic components, and without any reported adverse effects. To the best of our knowledge, this is the first reported case of a successful use of topical sirolimus for the treatment of KTS (with CLVM) and LVM. From reports to date, the topical use of sirolimus was found to be beneficial for LM cases and was studied in combined therapy with pulsed dye laser for capillary malformations (32–34). It was suggested previously that percutaneous delivery of the mTOR inhibitors may allow for an effective long-term therapy, while avoiding systemic toxicities (32). Indeed, from our limited experience, it appears that the topical use of sirolimus in cases of the VMs with lymphatic components, such as the LVM and CLVM, and not only in cases of pure LMs, is both efficient and safe.
In both retrospective study and literature review, most patients were still taking sirolimus at the end-point of the study. As of today, there are no guidelines that determine the duration of sirolimus therapy, when the treatment should be stopped, or if it should be done gradually. Moreover, information regarding the long-term toxicities of sirolimus remains limited.
Conclusion
Sirolimus appears to be effective in children and young adults with complicated VAs. Treatment was tolerated well, with acceptable adverse effects. Further study is needed into early use of sirolimus in cases of low-flow lesions, overgrowth syndromes with low-flow components, and VAs with an overexpression of the mTOR pathway. Topical use of sirolimus in cases of VM with a lymphatic component, such as LVM and CLVM, is both efficient and safe. Although a phase II clinical study was published recently, further prospective studies are needed to evaluate the long-term adverse effect of sirolimus treat-ment and to identify high-risk VAs patients presenting with specific disease phenotypes and/or genotypes, in whom sirolimus is effective and safe.
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Informed consent was obtained from all individual participants included in the study.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize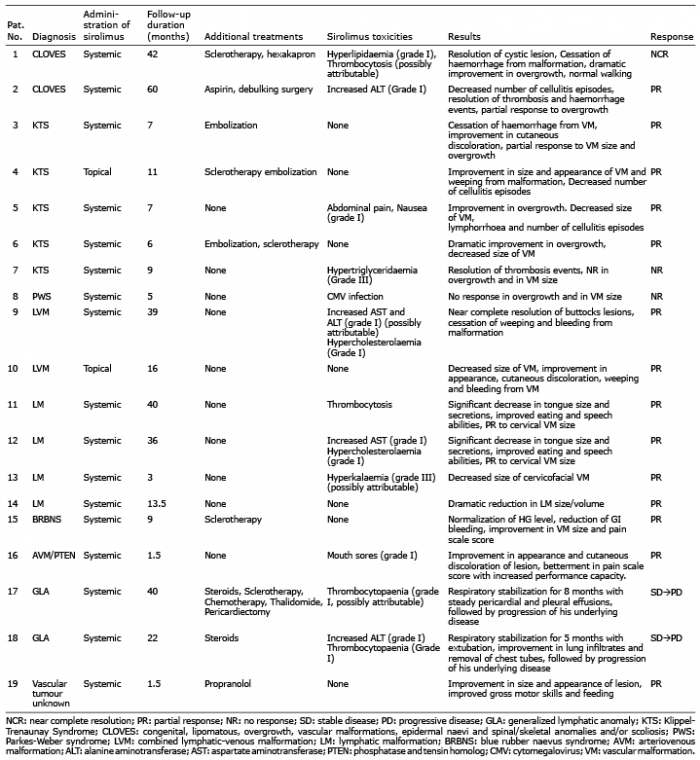 Click to show fullsize
Click to show fullsize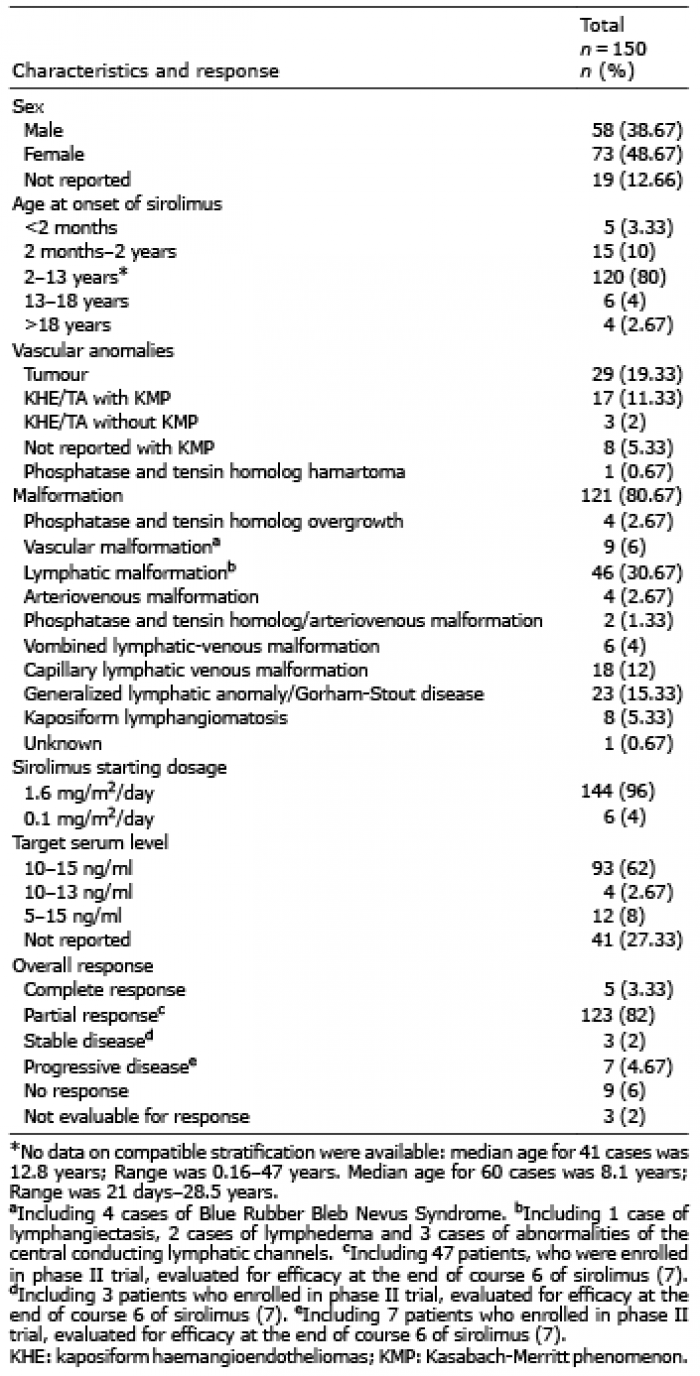 Click to show fullsize
Click to show fullsize