


1Department of Dermatology, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences & Peking Union Medical College, Beijing, 2Department of Dermatology, Chengdu Second People’s Hospital, Sichuan, 3Department of Dermatology, Shuangqiao Hospital of Chaoyang District, Beijing, and 4Department of Dermatology, Tianjin Academy of Traditional Chinese Medicine Affiliated Hospital, Tianjin, China
Wolf’s isotopic response refers to the occurrence of a new skin disease at the exact site of an unrelated skin disease that had previously healed. Various cutaneous lesions have been described after herpes zoster. This study included 24 patients with Wolf’s isotopic response after herpes zoster infection, which presented as manifestations ranging from inflammatory disease to carcinoma. Histopathological examinations in 12 patients and immunohistochemical analyses in 10 patients allowed exploration of secondary microscopic changes in the lesions. CD4+/CD8+ T-cell ratios were normal and infiltrating cells included mast cells, eosinophils, and tumour cells. Our study has described additional patients with confirmed Wolf’s isotopic response following herpes zoster infection; moreover, it has extended the spectrum of Wolf’s isotopic response to include impetigo. We suggest Wolf’s isotopic response classification categories for herpes zoster-associated Wolf’s isotopic response. Additionally, clinicians should consider the possibilities of different diseases in Wolf’s isotopic response, especially malignancies.
Key words: Wolf’s isotopic response; herpes zoster; syringoid eccrine carcinoma; lichen sclerosus et atrophicus.
Accepted Jul 17, 2019; E-published Jul 17, 2019
Acta Derm Venereol
Corr: Yuehua LIU, Department of Dermatology, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences & Peking Union Medical College, No. 1 Shuai Fu Yuan, Dongcheng District, Beijing 100730, China. E-mail: yuehualiu@263.net
Wolf’s isotopic response (WIR) is widely accepted as a clinical concept. Twenty-four new patients presented with WIR after herpes zoster were enrolled in this study including first described disease. Based on the mini literature review and histopathological study in this study, we tend to a hypothesis that WIR caused by neuro-immune impairment and propose a classification method based on pathological findings, the epidermal and follicular changes, dermal tissue changes, inflammatory infiltrations and malignant invasions in WIR. Through the study in this paper, clinicians are reminded to be aware of this phenomenon, especially the possibility of associated tumorous diseases.
Wolf’s isotopic response (WIR) was first described in 1955 and refers to the occurrence of a new skin disorder at the exact site of an unrelated skin disorder that had previously healed. Wolf et al. recognised this dermatological phenomenon and established a precise definition for WIR (1). Until recently, controversy has surrounded the definitions of WIR and isomorphic response – also known as the Köebner phenomenon – which describes the development of the same disease at a site with damaged or traumatised skin (2, 3). Many cutaneous WIR reactions have been reported in the literature (4–6). In a recent commentary, Wolf et al. (2) expanded the definition of healed skin diseases that trigger an isotopic response; the definition now includes ‘scars, pigment changes, colour changes or various other minimal changes by the first disease’.
Herpes zoster (HPZ) is a localised disease that results from the reactivation of an endogenous varicella-zoster virus (VZV) infection which persisted in latent form within sensory ganglia following an earlier attack of varicella. During an HPZ outbreak, the virus continues to replicate in the affected dorsal root ganglion and produces painful ganglionitis. Neuronal inflammation and necrosis can result in severe neuralgia, which intensifies as the virus spreads down the sensory nerve. Many cutaneous lesions at the site of healed HPZ have been described as WIR; thus, HPZ is the most common primary disease to induce WIR (7), and a new term, ‘Wolf’s postherpetic isotopic response’, has been suggested by several authors (8). The pathogenesis of WIR after HPZ remains unclear, although various theories have been proposed to explain this phenomenon; these include viral, vascular, and immunologic hypotheses, as well as a neural hypothesis (6), which may be the most widely accepted. There are several descriptions of this clinical phenomenon, and it requires further classification and investigation. In the present study, we enrolled 24 patients who had WIR after HPZ. We characterised the clinical manifestations and explored the dermatopathological features of WIR. In addition, we conducted a concise literature review of WIR, including epidermal changes, inflammatory infiltration, and malignant invasion.
Twenty-four patients with cutaneous lesions after HPZ were enrolled in this study. Patients’ clinical medical histories were obtained if available. Age, sex, time interval between acute HPZ and biopsy, treatment received, and medical history prior to HPZ were also recorded for each patient. Skin biopsies were performed for 12 patients. Immunohistochemical staining, including staining for CD4 (Maxim Biotechnologies, Fuzhou, China), CD8 (Leica Biosystems, Shanghai, China) and CD117 (c-kit; Leica Biosystems), was conducted for 10 patients; CD138 (Leica Biosystems) staining was conducted for two patients. Patient 7 was only assessed using direct immunofluorescence and indirect immunofluorescence to test antibodies BP180 and 230 (ELISA; Euroimmun, Beijing, China), whereas slides for patient 11 showed only stained elastic tissue with no staining for CD4, CD8, or CD117 (9). Patient 20 underwent additional immunohistopathological staining to diagnose the tumour.
Informed consent was obtained from all patients. Oral or written ethical statements were obtained when patients were photographed, and written consent was obtained when patients were biopsied.
We performed a literature search to collect data regarding WIR. Relevant literature published from 1987 to 2018 was obtained from PubMed and Embase using the keywords: ‘Wolf’s isotopic response’, ‘isotopic response’, and ‘herpes zoster’. The search and selection of the literature was restricted to publications written in English or abstracts in English. All reviews, case series, case reports, and letters to the editor mentioning this phenomenon and describing relevant histopathological changes were reviewed.
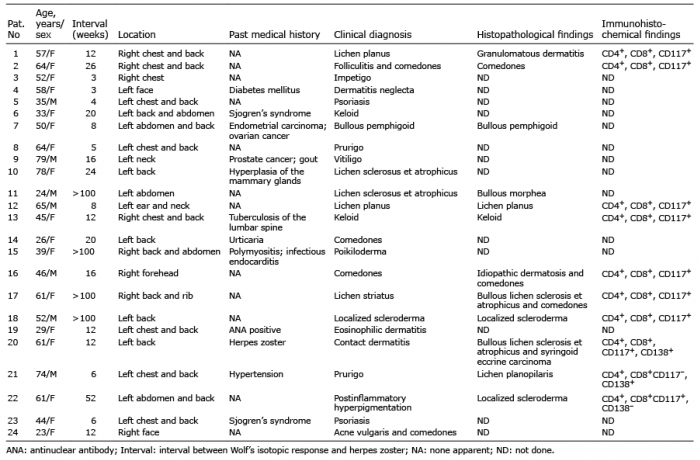
Clinical findings for our series are shown in Table I, including 17 women and 7 men, with an age range of 23–79 years (mean 50.8 years). Thirteen patients had no noteworthy medical history. Two patients had a history of cancer; in particular, patient 7 had been diagnosed with endometrial carcinoma and ovarian cancer, whereas patient 9 had been diagnosed with prostate cancer and gout. Patient 10 had hyperplasia of the mammary glands. Eight patients had chronic diseases, including 3 with autoimmune diseases (Sjögren’s syndrome in patients 6 and 23; polymyositis and infectious endocarditis in patient 15); these 8 patients regularly received systemic corticosteroids and/or immunosuppressive agents. Patient 19 had a positive antinuclear antibody (titre 1:160), but exhibited no definite rheumatoid diseases. Diabetes mellitus, tuberculosis of the lumbar spine, urticaria, and hypertension were found in patients 4, 13, 14, and 21, respectively.
Table I. Clinical and histopathological characteristics of the 24 patients in this study
Nineteen lesions were on the trunk, 4 on the face and neck, and one on the neck and shoulder. As shown in Table I, the time intervals between HPZ and the presentations of cutaneous reactions at the sites of HPZ scars varied, ranging from 3 to > 100 weeks (mean 28.3 weeks). Clinically, patients’ cutaneous manifestations exhibited various appearances. Twelve patients were diagnosed based on a dermatologist’s clinical findings without further histopathological tests. Diagnoses included impetigo (patient 3), dermatitis neglecta (patient 4), psoriasis (patients 5 and 23), keloid (patient 6), prurigo (patient 8), vitiligo (patient 9), lichen sclerosus et atrophicus (LSA; patient 10), comedones (patient 14), poikiloderma (patient 15), eosinophilic dermatitis (patient 19), and acne vulgaris and comedones (patient 24). Impetigo and dermatitis neglecta (patients 3 and 4) were not reported previously in WIR.
Histopathological findings enabled a definitive diagnosis in 12 patients. Comedones were found in 5 patients (20.8%); 3 patients were confirmed by slide staining and two patients by clinical diagnosis. In slides from 9 patients, we observed mast cells (MCs) diffusely distributed in the region of inflammation (9/12, 75.0%). Immunohistochemical staining was positive for CD4+ and CD8+ T cells in 10 patients, and CD4+/CD8+ ratios were normal. CD117 staining was positive in slides from 9 patients (9/10, 90.0%). CD138 staining was performed in two slides; one was positive. Syringoid eccrine carcinoma (SEC) accompanied by bullous LSA (BLSA) was diagnosed in patient 20; this represents a novel report in the WIR literature, and the detailed description is given below in the Case 20 subsection.
Case 17. A 61-year-old woman presented with band-like patches over her right back and ribs, which had persisted for 3 months. The patient exhibited white and black papules and patches, as well as petechiae (Fig. 1a). There had been an HPZ skin lesion in the same region 2 years previously, which had been treated with traditional Chinese herbs for 14 days. The patient was otherwise in good health.
Her linear skin lesion was initially diagnosed as lichen striatus. Histopathological examination of atrophic follicular lesions on the upper back showed basket-weave hyperkeratosis in the epidermis, atrophy and flattening of the rete ridges, vacuolar degeneration in the basal layer, cleft formation, homogenisation, and melanin incontinence. Perivascular lymphocyte infiltration was observed on skin appendages (Fig. 1b, c). These findings were consistent with a histological diagnosis of BLSA. In addition, slides showed follicular invagination obstructed by keratin. A diagnosis was made of BLSA and comedones after HPZ. Immunohistochemistry staining was positive for CD4, CD8, and CD117 (Fig. 1d). A corticosteroid cream was given to the patient, and she underwent regular follow-up.
Fig. 1. Case 17. (a) White or black papules, patches, and petechiae on the right side of the back. (b) Biopsy of atrophic follicular lesions on the upper back shows typical comedo and atrophic epidermis with hydropic degeneration of the basal cell layer, forming a subepidermal split with pronounced dermal oedema and homogenisation of collagen in the upper dermis; dense lymphocytic periappendageal infiltrate is present in the mid-dermis. (c) High-power view of a typical comedo. (d) Positive staining for CD117.
Case 20. A 61-year-old woman presented with band-like erythema and bullae over the right side of her back, which had persisted for 3 weeks. Physical examination revealed band-like well-demarcated hypopigmented patches, with erythema, vesicles, and bullae over the hypopigmented patches. The surrounding skin was extremely thin and translucent (Fig. 2a). Past medical history revealed that she had been diagnosed with HPZ 6 years prior, with residual atrophy and hypopigmentation since then. She had recurrent HPZ one year prior, which had caused residual subcutaneous nodules.
Skin biopsies were taken from the bullous and nodular areas. Histopathological analysis led to a diagnosis of SEC accompanied by BLSA (Fig. 2b). Immunohistochemistry showed inflammatory cells that were positive for CD4, CD8, CD117, and CD138. Infiltrated tumour cells were positive for smooth muscle actin, p63, cytokeratin 7 (Fig. 2c), S100 (Fig. 2d) and β-catenin. The Ki67 index was approximately 5%. After resection and skin grafting, no recurrence was observed during 1-year of follow-up.
Fig. 2. Case 20. (a) Band-like, well-demarcated hypopigmented patch, with erythema, vesicles, and bullae over the hypopigmented patch. (b) Hydropic degeneration of the basal cell layer forming a subepidermal split with pronounced dermal oedema and homogenisation of collagen in the upper dermis, as well as atypical infiltrating glands in the mid-dermis. (c) Positive staining for cytokeratin 7. (d) Positive staining for S100.
Our case series is unique in that we enrolled 24 patients with WIR after HPZ. A variety of clinical manifestations of the second dermatosis differed from initial HPZ. Compared with previous reports, we have added several new diseases and extended the spectrum of WIR to include impetigo, dermatitis neglecta, and a rare instance of SEC accompanied by BLSA. Our patients had various medical histories and ages, and their disease manifestations ranged from pure pigment abnormalities to dermal adnexal carcinoma. Nevertheless, we believe that all of these WIR reactions were caused by local pathological structural changes, where HPZ was the driving factor leading to abnormal immune function. We have reviewed the previous literature and found that there remains a lack of unified labelling of WIR classification. Unlike disease category and disease manifestation, classification based on pathological changes can enable clinicians to more clearly understand WIR (Fig. 3).
Fig. 3. Illustration of neuroimmune dysfunction-induced secondary histopathological classification in Wolf’s isotopic response after herpes zoster (HPZ). LP: lichen planus; LSA: lichen sclerosus et atrophicus; BP: bullous pemphigoid; BCC: basal cell carcinoma; SCC: squamous cell carcinoma.
The pathogenesis of WIR following the resolution of HPZ lesions remains incompletely understood. In the literature, type III or IV hypersensitivity reactions and Köebner’s phenomenon have been suggested to elicit the onset of WIR (5). Researchers have found VZV DNA in early lesions with no histologically observed viral cytopathic changes, suggesting that the virus induces an atypical delayed hypersensitivity reaction that is unaffected by antiviral therapy (10). Another study found no association between the persistence of VZV DNA and granuloma formation (11). Other investigations have indicated that cutaneous reactions appearing at sites of HPZ scars are not due to the presence of persistent VZV DNA within lesions (5, 12, 13). One study suggested that the previously unrecognised existence of resident memory CD8+ T cells may contribute to the pathogenesis of lichenoid reactions in postherpetic WIR lesions (14). The density of epidermal nerve endings in previously HPZ-affected skin is reduced, compared with normal skin (15). The effects of nerve injury causing immune dysfunction are related to neuropeptide release, thus altering immune control in the affected dermatome (16). Immunity-related disorders caused by peripheral neuropathy other than HPZ-induced neuropathy have been observed in both acne (17) and bullous pemphigoid (18). We propose that this mechanism of neuroimmune destabilisation in the VZV-infected site, which leads to the onset of various immunity-related disorders along the affected dermatome, is caused by the continued influence of viral DNA. In addition to conducting sensorial stimuli centripetally, sensory nerve fibres modulate the skin immune response centrifugally by secreting neuromodulators (such as substance P, vasoactive intestinal peptide, and calcitonin gene-related peptide) that interact with membrane receptors of immune cells (MCs, lympho-cytes, and Langerhans’ cells) (16). Clinically, other common skin diseases where isotopic responses may occur (e.g., insect bite reaction) may not fit with the nerve injury hypothesis. In this study, we found CD117+ MCs in 9 of 10 patients. This was representative of excessive local immune reactions in VZV-infected dermatomes. Clinically, we observed bullous pemphigoid (patient 7), lichen planus (patient 12), BLSA (patients 17 and 20), bullous morphoea (patient 11), scleroderma (patients 18 and 22), and psoriasis (patients 5 and 23). In addition, we found infections with bacteria and fungi due to local immune destabilisation including acneiform dermatosis (patients 2 and 24), impetigo (patient 3), and dermatitis neglecta (patient 4).
In our case series, we found typical acne or comedones in 5 patients (patients 2, 14, 16, 17, and 24). There have been a few reports of the development of comedones, as well as acneiform eruption, at the site of healed HPZ (7, 19–22). In addition, there have been reports of patients with localised dermatitis neglecta, scleroderma, LSA, psoriasis, lichen planus, and pigmentation changes in melanocytes (such as vitiligo and poikiloderma). Although these patients differed from each another in clinical and pathological diagnoses, obvious epidermal changes, such as hyperkeratosis, follicular plug, atrophy of stratum spinosum, or psoriatic hyperplasia showed that epidermal and follicular changes are common in WIR skin. In addition to the diseases mentioned above with skin and hair follicle changes, there have been diseases reported in the literature with the above manifestations, such as lupus erythematosus (23, 24), granulomatous folliculitis (5, 25), acquired perforating folliculitis (26), Trichophyton rubrum folliculitis (27), epidermal cyst (28), giant lichenification (29), poliosis (30), and molluscum contagiosum (31). As we noted above, we propose that the local network of nerve fibres is destroyed after VZV infection. The release of neuropeptides, such as substance P, from damaged nerve endings might play a crucial role in inducing the development of epidermal changes at the site of healed HPZ. Similarly, it has been reported that capsaicin treatment of trigeminal neuralgia after trauma improves pain and acne on the cheeks, thus indicating that local nerve abnormalities can cause local skin tissue lesions by changing the concentration of substance P (17).
There are few changes in dermal components after WIR; these primarily manifest as fibroblast proliferation, widening and densification of collagen, keloid (patients 6 and 13), bullous morphoea (patient 11), scleroderma (patient 19), or LSA (patients 17 and 20). As reported previously, local immune response, vascular injuries, and trauma caused by viral infection can elicit the onset of morphoea (9, 32–34). We have added here two rare instances of BLSA, as well as a patient with bullous scleroderma; these might have a similar pathogenesis. Another major component in dermal tissue is mucin produced by fibroblasts. Mucinosis has been reported, but its pathogenesis is unknown (35).
We explored inflammatory infiltrations in biopsy slides from 10 patients. Both CD4+ and CD8+ T cells were detected, and the CD4+/CD8+ T-cell ratios were normal. Patients 12 and 21 showed lichenoid infiltration, and CD4+ and CD8+ T cells in the epidermis and dermis were both present at near normal ratios; this finding differs from that of previous reports. Ise et al. (14) found that most lymphocytes in the epidermis were CD8+, while approximately equal numbers of CD4+ and CD8+ lymphocytes were detected in the dermis in a lichenoid reaction. We compared the clinical features in Ise’s report with those in patients 12 and 21 in the present study. The former patient presented with many red papules that were rarely fused. However, in patients 12 and 21, the red papules were small and darkened, approaching the stage of regression. Thus, the differences between these two studies may reflect differences in lymphocyte infiltration during progression of inflammation.
Nine of 10 patients’ slides in our study showed CD117+ MCs infiltrating the WIR lesion, which was not addressed in previous studies. However, MCs are involved in many pathophysiological processes and immune responses in the skin because they produce and release various cytokines and inflammatory mediators that can cause disease; these include psoriasis (patient 5) (36–38), keloid (patients 6 and 13) (39, 40), bullous pemphigoid (patient 7) (5, 41), and lichen planus (patient 12) (42). We speculate that MCs play key roles in skin lesions after HPZ.
However, in patient 21, the slides showed lichen planopilaris; CD117+ MCs were negative, but CD138+ plasma cell infiltration was detected. In patient 20, CD117+ MCs and CD138+ plasma cells revealed that inflammatory infiltration might differ, as clinical manifestations varied. Moreover, eosinophils (43, 44) and neutrophils (14) were found in patients 3, 7, 19, and 24 in our study, as well as in previous studies.
Most inflammatory infiltrations in WIR are granulomatous (4, 12, 45). Therefore, we speculate that nerve damage and residual virus particles after virus infection may lead to the secretion of interleukin-4 and other chemokines, as well as infiltration of the above inflammatory cells.
SEC (patient 20) is a rare malignant adnexal tumour of eccrine origin. In a search of PubMed, we found no report of SEC as a WIR. However, reports of malignant invasion in WIR are not uncommon in the literature. Wolf et al. reviewed and reported 66 patients with WIR; 35 had malignant disease, including breast carcinoma, basal cell carcinoma, squamous cell carcinoma, baso-squamous carcinoma, Kaposi’s sarcoma, angiosarcoma, metastasis, Bowen’s disease, lymphoma, and leukaemia cutis (1). Instead of administering antiviral drugs or other treatments, we suggest that biopsy should be performed to exclude neoplasm (4, 46, 47).
The number of patients included in our study was small, and the numbers of specimens for histopathological and immunohistochemical examinations were limited; thus, assessments of VZV-DNA, CD8+ resident T cells, and/or neuropeptides could not be performed. Although we detected CD117 and CD138 in MCs and plasma cells, we did not assess the mechanism of inflammatory factors associated with these cells in WIR. WIR is uncommon in clinical practice, partly because of the lack of knowledge regarding this disease, and partly because of patients’ poor recall regarding previous primary diseases. When WIR is given closer attention by clinicians, more patients may receive a diagnosis of WIR; thus, additional in-depth studies on this phenomenon are needed in the future.
WIR is a specific phenomenon that is defined as a secondary disease at the site of a superficial scar, pigment changes, or other minimal changes left by the first disease (48). The pathogenesis of WIR is not yet clear, and neuroimmune instability at VZV infection sites might induce the occurrence of WIR (16). We have described 24 patients with WIR, including some with diseases that were not previously included in the definition of WIR. We reviewed the literature and classified WIR into 4 groups based on dermatopathological changes. As a rare clinical phenomenon, WIR should receive greater attention because of the possibility that it may be associated with malignant diseases.
The authors thank Guangzhou Sagene Biotech Co., Ltd. for their help with illustration and figure making. We also thank Cathel Kerr, BSc, PhD, Gillian Campbell, PhD, and Ryan Chastain-Gross, PhD, from Liwen Bianji, Edanz Group China (www.liwenbianji.cn/ac), for editing the English text of drafts of this manuscript.
This work was supported by the grants from the Fundamental Research Funds for the Central Universities (3332018025); NCMI-ABD02-201709.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize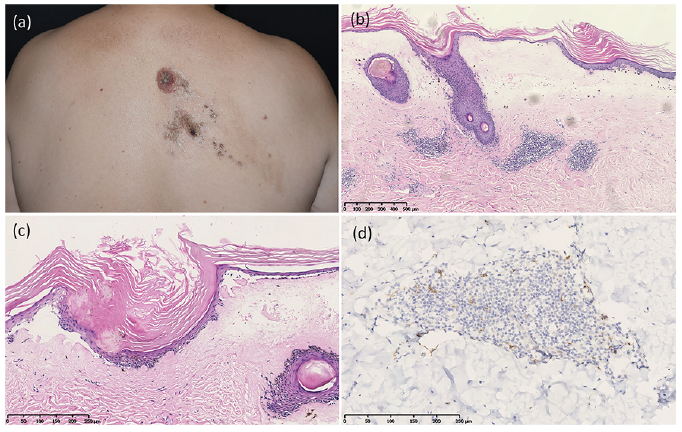 Click to show fullsize
Click to show fullsize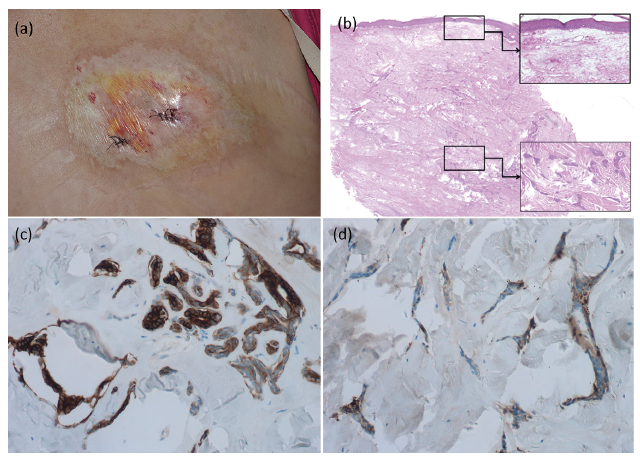 Click to show fullsize
Click to show fullsize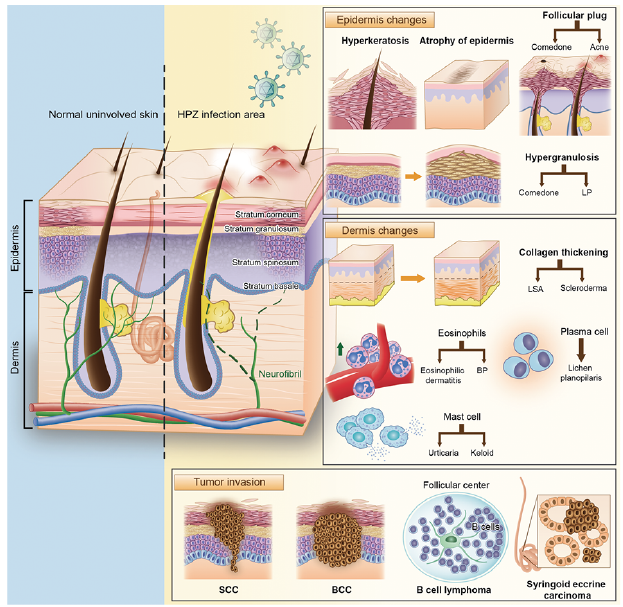 Click to show fullsize
Click to show fullsize