


1Department of Dermatology, Venereology and Allergology, and 2Department of Geriatrics, Wroc?aw Medical University, Wroc?aw, Poland
Ageing is associated with numerous medical afflictions, including dermatological symptoms and diseases. Chronic itch (CI) in elderly people is a frequent symptom of diverse aetiology. This study assessed the prevalence and detailed clinical features of CI among 153 elderly patients hospitalized in the geriatric ward, including associations with comorbidities and pharmacotherapy. CI affected 35.3% of subjects, most commonly due to cutaneous conditions, mixed aetiology and neurological disorders (53.7%, 25.9% and 11.1% of pruritic subjects, respectively). The mean itch intensity assessed with the 4-Item Itch Questionnaire (4IIQ) was 6.6 ± 2.8 points. Viral hepatitis (p = 0.02), higher serum creatinine concentration (p = 0.02) and coexistent purpuric lesions (p = 0.002) were associated with higher 4IIQ scores. In logistic regression analysis CI correlated positively with female sex, atopic dermatitis, immobility, rheumatoid arthritis and ischaemic neurological diseases, while low-molecular-weight heparins, antipruritic drugs, allergy, rosacea and higher haemoglobin concentration had the contrary effect. CI is a frequent and interdisciplinary problem among elderly subjects, which requires a holistic clinical approach.
Key words: itch; elderly; comorbidities; pharmacotherapy.
Accepted Aug 5, 2019; E-published Aug 6, 2019
Acta Derm Venereol 2019; XX: XX–XX.
Corr: Jacek C. Szepietowski, Department of Dermatology, Venereology and Allergology, Wroc?aw Medical University, ul. Cha?ubi?skiego 1, PL-50-368, Wroc?aw, Poland. E-mail: jacek.szepietowski@umed.wroc.pl
Chronic itch is a frequent problem of complex aetiopathogenesis, especially among elderly patients. This study extensively evaluated the prevalence, clinical characteristics and possible associations of chronic itch with systemic comorbidities and pharmacotherapy in a cohort of elderly patients hospitalized in a geriatric ward, which, to the best of our knowledge, have rarely been reported in the literature. The results of this study support the role of an interdisciplinary diagnostic and therapeutic approach to elderly patients with chronic itch.
Due to increased life expectancy, the elderly population is constantly increasing worldwide, with an estimated 2.1 billion seniors living in 2050 and possibly 3.1 billion in 2100 (1). In addition, in the course of ageing these individuals are more prone to experience numerous clinically evident comorbidities or, at least, possess subclinical pathologies in various organs (2). Another associated problem of increasing importance is polypharmacy, which is characterized by prescription and use of multiple drugs to manage concomitant diseases (3). Ageing affects all organs, and skin is no exception, as it undergoes both intrinsic (physiological and inevitable) and extrinsic ageing (mainly associated with exposure to ultraviolet (UV) light) (4, 5). Unsurprisingly, cutaneous issues in elderly people are profuse, as demonstrated by various studies throughout the years (6–10). Chronic itch (CI), defined as an unpleasant sensation eliciting the urge to scratch, which lasts at least 6 weeks (11), is a flagship example of a condition with multifactorial aetiopathogenesis (12). The International Forum for the Study of Itch (IFSI) classifies pruritus according to its suspected causes as dermatological (I), systemic (II), neurological (III), psychogenic (IV), mixed (V; several categories) and other (VI) (13). Regardless of the cause, CI remains one of the crucial dermatological condition in older individuals, owing to its high frequency and detrimental impact on sleep and quality of life (QoL) of the affected individuals (14, 15). Overall, the detailed aspects of itch in elderly people have rarely been reported in the literature (14, 16). Therefore, this study aimed to investigate the frequency and detailed clinical characteristics of CI in elderly patients, along with possible associations of the aforementioned with comorbidities and co-administration of pharmacotherapy.
Study population and design
This prospective cross-sectional study was performed between January 2018 and May 2018. We approached 185 patients aged 65 years or older who were hospitalized in the geriatric ward, among whom 153 (82.7%) agreed to participate in the study. The inclusion criteria were: age 65 years or more and informed agreement to participate in the study. Exclusion criteria were: patients who were unable to understand the study procedures (e.g. due to mental state). In addition to basic demographic data, a detailed medical history was gathered, with a particular focus on systemic comorbidities and systemic drug intake. The results of routine laboratory blood tests performed during the hospitalization were also noted. If multiple laboratory tests were performed during the hospitalization, the results closest to the day of dermatological examination were chosen. The laboratory data encompassed concentrations of haemoglobin (Hb; reference range 12–16 g/dl in females, 14–18 g/dl in males), C-reactive protein (CRP; reference range 0.2–5 mg/l), aspartate aminotransferase (ASPAT) (reference range 5–34 U/l), alanine aminotransferase (ALAT) (reference range 0–35 U/l), serum creatinine (reference range 0.73–1.18 mg/dl) and glomerular filtration rate (GFR; according to Cockcroft-Gault equation). Concerning the skin, the data on coexisting dermatoses and application of emollients (including daily frequency) was obtained; no data was collected concerning the type of emollients (bland vs. urea containing emollients).
Skin dryness (xerosis) was evaluated using a 5-point scale (0: no xerosis; 1: mild; 2: moderate; 3: severe; 4: very severe) (17). The main clinical parameter, the presence of CI, was documented, including the affected anatomical locations. The 4-Item Itch Questionnaire (4IIQ) (18–21) was utilized to assess CI extensity, severity, frequency, and associated sleep impairment. Our modified questionnaire for the description of itch (22) was completed, evaluating the presence of itch in the last 3 days. A numerical rating scale (NRS; 0: no itch; 10: worst imaginable itch) was utilized to assess maximal values of itch intensity both in the last 3 days and during the course of the symptom. Furthermore, the description of cutaneous sensations associated with itch, emotional burden of itch, sleep impairment, certain factors influencing itch intensity and itch impact on psyche were noted. QoL and stigmatization were measured with the Dermatology Life Quality Index (DLQI) questionnaire (23) and 6-Item Stigmatisation Scale (6ISS) (24), respectively. This study was conducted in concordance with the approval of Bioethics Committee of Wroc?aw Medical University (KB-124/2018).
Statistical analysis
Data were collected for 153 subjects; 54 (35.3%) of whom reported having CI. The data from the latter subgroup was additionally extracted for subsequent analyses. Descriptive statistics were used to display the variables in different age groups (65–79 years; 80 years and older), with an appropriate application of significance tests (Student’s t-test, χ2 test, Mann–Whitney test). Pearson correlation coefficient (cc), Spearman rank cc, point-biserial, rank-biserial, and the standardized contingency coefficient (C Pearson) were utilized for correlational purposes, where appropriate. We also performed a logistic regression for the CI variable (as dependent), establishing the crucial impacting factors (independent variables) and their odds ratios (OR). A p < 0.05 was considered statistically significant. All procedures were conducted using Statistica 13 (Dell, Inc., Tulsa, USA) software.
General demographics, systemic comorbidities, basic laboratory tests and pharmacotherapy
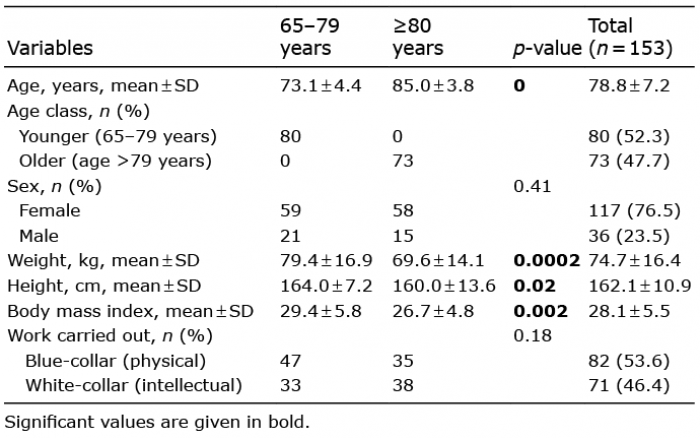
The study involved 153 patients (36 males and 117 females; 23.5% vs. 76.5%). The age of the participants ranged from 65 to 95 years (mean ± standard deviation (SD) 78.8 ± 7.2 years), with 73 subjects (47.7%) aged 80 years or older. Clinical characteristics of the examined individuals displayed in different age groups (65–79 vs. 80 years and older) are shown in Table I. The most common systemic comorbidities encompassed arterial hypertension (73.9%), joint disorders (58.8%; mostly osteoarthritis), neurological disorders (51.6%; most commonly ischaemic), cardiovascular disorders (51%; mostly ischaemic heart disease) and gastrointestinal disorders (33.3%; mostly peptic ulcer disease). Basic laboratory evaluations encompassed haemoglobin concentration (mean 12.8 ± 1.5 g/dl), serum creatinine (mean 0.9 ± 0.3 mg/dl), GFR (mean 71.7 ± 21.2 ml/min), ASPAT (mean 23.0 ± 7.5 U/l), ALAT (mean 21.3 ± 9.5 U/l) and CRP concentration (mean 10.4 ± 38.7 mg/l). All patients (100%) were taking at least one systemic drug, most commonly angiotensin converting enzyme inhibitors (ACEI) and angiotensin receptor blockers (ARB) (59.5% in total, mostly ACEI), β-blockers (55.6%), statins (49%), Ca-blockers (45.1%), and diuretics (43.8%; mostly thiazides). Drugs with proven antipruritic properties were used by 28.1% of patients (mostly H1-antihistamines).
Table I. Baseline demographics of the subjects
Cutaneous comorbidities, emollients application and xerosis
All patients presented at least one cutaneous comorbidity. The most frequent comprised lentigines (76.5%), seborrhoeic keratosis (41.8%), varicose veins (39.9%), senile angiomas (29.4%) and pigmented naevi (28.8%). Daily application of emollients was confirmed by 61.4% of subjects, with the frequency of application once a day (median). Skin dryness (xerosis) concerned 94.1% of individuals, with a median intensity of 2 points.
Itch characteristics
CI was reported by 35.3% of examined patients, with no significant difference between age groups (31.3% vs. 39.7%; p = 0.27). Among CI group there were 46 females and 8 males (85.2% vs. 14.8%). The majority of these subjects reported itch episode during the last 3 days (75.9%). The most common aetiology of CI involved cutaneous conditions (IFSI I; 53.7% of pruritic subjects); mixed aetiology (IFSI V; 25.9%) and neurological disorders (IFSI III; 11.1%). CI mostly affected the back (48.2%), upper and lower limbs (40.7% each), head (29.6%) and anogenital area (9.3%). Generalized itch bothered only one patient (1.9%). The mean 4IIQ score was 6.6 ± 2.8 points, with no differences between younger and older age groups (6.5 ± 2.2 vs. 6.8 ± 3.2 points; p = 0.68). Notably, nearly half of pruritic patients reported longer duration of single itch episodes, lasting over 10 min (46.3%). Itching occurred most frequently during the evening (90.7%), although it was often present in the morning, midday and night (74.1%, 74.1% and 57.4%, respectively). The mean NRS score for itch intensity during last 3 days was 3.7 ± 3.0 points, whereas maximal NRS score was 6.8 ± 2.5 points. Notably, NRS following a mosquito bite was also marked (6.2 ± 2.9 points). Usually, itch was not accompanied by other unpleasant cutaneous sensations (64.8%). Patients frequently described itch as irritating (77.8%) and burdensome (72.2%). Itch contributed to difficulties in falling asleep, awakenings and the use of soporifics in 25.9%, 22.2% and 11.1%, respectively. The most common exacerbating factors included sweating (51.9%), heat (44.4%), hot water (20.4%), fatigue (18.5%) and stress (16.7%), while physical activity, cold water, hot water, cold ambient temperature and dry air were considered as alleviating (in 33.3%, 27.8%, 25.9%, 16.7% and 11.1%, respectively). Nearly two-thirds (63%) of subjects regarded itch as a factor negatively influencing their mood. The detailed data concerning CI characteristics are listed in Table II and Table SI, whereas the data concerning systemic comorbidities, laboratory scores, pharmacotherapy and cutaneous comorbidities are presented in Table SII.
Table II. Detailed characteristics of chronic itch (CI) patients (n = 54)
Quality of life and stigmatization among subjects with chronic itch
The mean DLQI score was 3.3 ± 3.2 points (range 0–15 points), with no statistically significant difference between age groups (3.3 ± 2.6 for patients aged 65–79 years, 3.2 ± 3.7 for those aged 80 years and over; p = 0.97). In general, patients exhibited low stigmatization levels (mean 0.4 ± 1.2 points).
Relevant itch-related correlations, including comorbi-dities, pharmacotherapy and laboratory results
Unsurprisingly, patients taking drugs with proven beneficial effects on itch reported CI less often (cc –0.34; p = 0.004), especially those taking H1-antihistamines (cc –0.29; p = 0.02). Remarkably, CI was also less common in patients with allergic disorders (atopic asthma, allergic rhinitis, allergic conjunctivitis, oedema of Quincke) (cc –0.26; p = 0.04) and malignancies (excluding cutaneous) (cc –0.35; p = 0.004). Higher 4IIQ values were reported by subjects with viral hepatitis (cc=0.32; p = 0.02), purpura (cc=0.42; p = 0.002), benign prostatic hyperplasia (BPH) (cc=0.28; p = 0.04) as well as those with higher creatinine levels (cc=0.31; p = 0.02) and lower GFR (cc –0.27; p = 0.05). On the other hand, diabetes mellitus (cc –0.28; p = 0.04), lower limb oedema (cc –0.27; p < 0.05) and administration of ACEI/ARB (cc –0.37; p = 0.01) were associated with lower 4IIQ scores. With higher age the likelihood of itch being alleviated by cold water was increased (cc=0.31; p = 0.02). Itch located on lower limbs occurred more often in individuals with chronic venous insufficiency (cc=0.49; p = 0.01), hypothyroidism (cc=0.44; p = 0.04), as well as those taking psychiatric drugs, excluding selective serotonin reuptake inhibitors (SSRI) (cc=0.50; p = 0.01) and novel oral anticoagulants (NOAC) (cc=0.45; p = 0.02). Abdominal location of itch was strongly correlated with higher concentrations of CRP (cc=0.67; p< 0.001). The intake of α-blockers was associated with higher NRS scores in the last 3 days (cc=0.30; p = 0.03), higher maximal NRS scores (CC=0.31; p = 0.02) and the need to use soporifics (cc=0.43; p = 0.002). Anxiety disorders strongly favoured itch occurrence during midday (cc=0.70; p = 0.03). Furthermore, the coexistence of arrhythmia (cc=0.51; p = 0.02) or ischaemic heart disease (cc=0.45; p = 0.03) was commonly associated with itch accompanied by burning sensation.
Chronic itch in logistic regression model
Logistic regression analysis (CI as a dependent variable) revealed that CI correlated positively with female sex (OR 4.4), immobility (OR 21.4), atopic dermatitis (OR 13.9), rheumatoid arthritis (RA) (OR 25.2) and ischaemic neurological diseases (OR 2.5). Interestingly, a contrary effect was observed for co-administration of low molecular weight heparins (OR 0.04) and antipruritic drugs (OR 0.07), as well as coexistence of allergy (OR 0.09), rosacea (OR 0.2) and higher serum haemoglobin concentration (OR 0.9) (Table III).
Table III. Logistic regression parameters for chronic itch (CI) as an effect
This study has several limitations. Firstly, it involved elderly patients hospitalized in a geriatric ward. Therefore the findings presented here may not necessarily reflect the possible associations in the general population of elderly people. Secondly, the number of subjects with CI was relatively small (n = 54). In addition, the descriptive nature of the study has to be taken into account. The presence of multiple comorbidities limits statistical analyses and may possibly present national variations according to different geographical and lifestyle factors. Finally, due to the trend of increased life expectancy of women, there were more women than men.
The prevalence of CI in geriatric patients (35.3%) remains in concordance with our previous epidemiological report (9) in which this symptom was diagnosed in 34.8% of elderly subjects, although differences in its prevalence were observed between patients hospitalized in dermatology and geriatric wards (44.3% vs. 23.9%, respectively; p < 0.01). Other recent papers reported the prevalence of CI among geriatric subjects between 6.3% and 25% (10, 14), although in an Indian study (25) CI concerned 78.5% of examined subjects aged 55 years and over. In the most comprehensive clinical report focusing on CI in elderly people so far, Valdes-Rodriguez et al. (14) recounted that the mean VAS score for CI was 6.0 ± 2.1 points among elderly Mexicans, which is a higher value than in our cohort. Similar to our study, the most commonly affected anatomical areas were the legs (54%) and the back (45%). In contrast to our study, however, CI was correlated with the presence of diabetes mellitus (OR 2.3) and chronic venous insufficiency (OR 4.4), whereas no correlations were found in relation to drug intake. Among CI group, diabetes affected 27.8% of subjects.
Interestingly, the QoL impairment of CI subjects in our study was relatively low (mean DLQI score 3.3 ± 3.2 points) when compared with the results of a study conducted in Singapore (mean DLQI value 6.7 points) (26). Even more surprising is the fact that geriatric ward inpatients in our study presented low stigmatization levels. We speculate that these individuals were able to develop sufficient coping mechanisms due to the chronicity of this symptom.
The occurrence of CI in our cohort seemed to correlate with several factors. Firstly, antipruritic drugs (especially H1-antihistamines) decreased the probability of its occurrence. Histamine is considered as a classic itch mediator (27), although numerous other mediators also play a role in eliciting CI of various aetiology (28). Paradoxically, patients with allergic disorders were less prone to develop CI, possibly as a result of a more frequent intake of H1-antihistamines. However, we deem the supposed “protective” role of systemic malignancies to occur accidentally (none of the 16 patients with malignancies reported CI), especially when acknowledging the reports linking CI with various malignancies (29, 30). Higher itch intensity in subjects with purpura might reflect, at least partially, chronic skin insufficiency (dermatoporosis). Indeed, Saurat et al. (31) recounted that the presence of dermatoporosis was correlated with itching. Viral hepatitis has been associated with pruritus in the literature (32, 33), while higher creatinine levels along with lower GFR may denote CKD, which is a classic itchy disorder, especially in its advanced stages (34). The association of more severe itch with BPH is peculiar, although an association with the intake of α-blockers (especially tamsulosin) might be considered (35). Notably, among itch-alleviating factors, physical activity was reported most commonly by our patients. Previous reports on subjects with CI due to atopic dermatitis, CKD or psoriasis concordantly mentioned physical activity as an exacerbating factor of itch (19, 36, 37), perhaps as a result of sweating and friction from clothes. We hypothesize that physical activity in our elderly cohort served as a protective factor because it provided psychological distraction from itch.
Our logistic regression model demonstrated a vast impact of RA on itch occurrence. Douglas et al. (38) reported that 34% of patients with RA complained of itch, compared with 40% of controls with miscellaneous rheumatic non-inflammatory disorders (p-value non-significant). Other autoimmune disorders frequently manifesting with itch encompass Sjögren’s syndrome, systemic sclerosis and dermatomyositis (39–41). Immobility was another factor strongly impacting itch occurrence in the current study. It complicates effective topical care of the skin (12) and is associated with decreased water content in the skin (42), fostering xerosis and facilitating itch. Immobility may also stem from neurological disorders, e.g. ischaemic stroke. The latter is another possible cause of itch itself, as reported by several groups (43, 44). Other CI-precipitating factors in our study involved atopic dermatitis (in which itching is a predominant and essential diagnostic feature) (45) as well as female sex. In fact, itch differences between sexes have been reported by Ständer et al. (46), with women being more prone to neuropathic and multifactorial causes of itch. On the other hand, current therapy with low molecular weight heparins seemed to play a role in decreasing the probability of CI in our study. This remains in concordance with studies reporting beneficial effects of enoxaparin in lichen planus, both in terms of cutaneous lesions and pruritus (47, 48). A possible explanation involves the decreased expression of T-lymphocyte heparanase by heparin, subsequently inhibiting T-cell migration and delayed type hypersensitivity (48). The seemingly protective role of rosacea in our cohort is difficult to account for, as pruritus is a typical feature of this disease (49). It is possible that the role of UV exposure might play a role. As described earlier, immobile patients were more prone to develop CI; it also seems that their limited activity results in less exposure to UV. Therefore, we speculate that higher activity status and subsequent exposure to UV might predispose to rosacea and concurrently decrease the probability of CI occurrence. Higher haemoglobin concentration might also be associated with lower risk of pruritus; conversely, the role of anaemia in eliciting pruritus is widely acknowledged (50–52).
All of the aforementioned observations require a cautious approach in the clinical decision-making process, as the data in the literature, particularly regarding the causative relationships between different aspects and factors influencing CI, is still lacking. Multifactorial aetiology of CI is well-known; however, the relative impact of individual factors remains an issue. Nevertheless, our experience clearly demonstrates that patients with CI will benefit from a holistic and interdisciplinary approach. Although challenging and time-consuming, managing coexistent disorders and acknowledging polypharmacy is a sine qua non of therapeutic success in CI in the elderly population.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize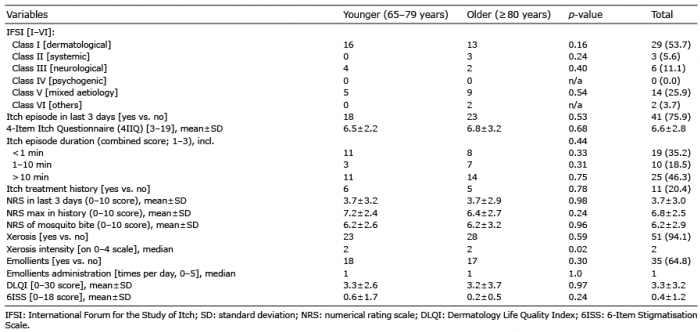 Click to show fullsize
Click to show fullsize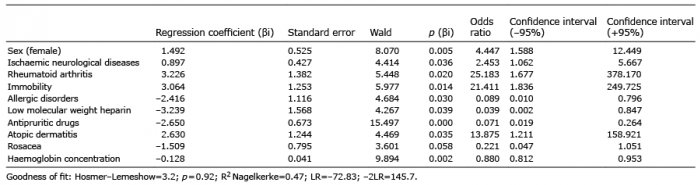 Click to show fullsize
Click to show fullsize