


1Department of Dermatology, Oslo University Hospital, PB 4950 Nydalen, NO-0424 Oslo, 2Institute of Clinical Medicine, 3Oslo Centre for Biostatistics and Epidemiology, Department of Biostatistics, Institute of Basic Medical Sciences, University of Oslo, Oslo, Norway. E-mail: mohammad.rizvi@ous-hf.no
Accepted Aug 6, 2019; E-published Aug 6, 2019
Actinic keratoses are common in organ transplant recipients (OTRs) and may be difficult to treat successfully. Several treatment modalities are available (1), including photodynamic therapy (PDT), i.e. applying a topical photosenzitiser to the lesions and exposing them to either artificial or natural daylight (2). Ablative fractional laser treatment (AFL) has been introduced to increase the absorption of the photosenzitiser and thereby increasing the treatment response in PDT (3). With very few clinical trials on the treatment of AKs in OTRs (1, 4), we set out to perform a clinical trial on AFL-assisted daylight PDT versus daylight PDT for AKs and field cancerization on scalp and forehead in OTRs, using a within-subject randomized controlled study design.
From the out-patient clinic at the Department of Dermatology, Oslo University Hospital, we recruited OTRs > 18 years and with stable graft function and multiple (> 5) AKs in two areas of identical size on scalp and/or forehead. Exclusion criteria were allergy to photosensitizing cream, previous PDT in the scalp and forehead < 6 months before inclusion, infiltrating tumours, porphyria or known tendency to produce hypertrophic scars. All AKs were graded according to Olsen et al. (5). Treatment areas in each patient were randomized by a computer-generated list to either AFL-assisted daylight PDT or daylight PDT (for flowchart, see Fig. S1).
Treatment areas randomized to AFL-assisted daylight PDT were treated with a 30 W Lutronic carbon dioxide laser (eCO2; Lutronic, Ilsan Techno Town, Korea), first targeting AK2- and AK3-lesions, followed by treatment of the whole field. Methylaminolaevulinate cream (Metvix®, Galderma, Biot, France) was then applied on both treatment areas. After 30 min, both treatment areas were exposed to sunlight for 2 h. Patients were then instructed to record pain on a 100 mm visual analogue scale (VAS) on paper after 30 min, 2, 24 and 48 h and 5 days (6). After one week, all patients were contacted by phone to report possible adverse effects. After 4 months, patients were examined by an assessor blinded for treatment allocations. Primary outcome was complete response, defined as no clinical sign of AKs. Secondary outcomes were partial response, defined as reduction in AK grade from baseline, occurrence of new AKs, and patient-reported pain.
Descriptive results are presented as frequencies (percentages) and medians (ranges). To evaluate treatment effect, we used a logistic regression model with generalized estimating equations (GEEs; robust estimator and exchangeable working correlation), taking multiple AKs in the same patient into account. Results are presented as odds ratios (ORs) with 95% confidence intervals (CIs), comparing AFL-assisted daylight PDT with daylight PDT. Due to few observations in some cells of the frequency table, AK2 and AK3 were combined in the GEE analysis of partial response. Patient-reported pain, recorded as VAS scores, was analyzed by Wilcoxon signed rank test. p-values < 0.05 were considered significant.
The study was approved by the Regional Committee for Ethics in Medical and Healthcare Research (Reference: 2013/194/ REK) and registered in clinicaltrials.gov (ID: NCT01898936). All patients gave their informed written consent. The study was conducted according to the Helsinki declaration.
We recruited 14 OTRs, of whom two were later lost to follow-up; thus 12 patients (10 kidney, 1 heart and 1 lung transplant recipients) were included in the analyses. Median age was 69 years (range 48–79), and median years after transplantation was 12 (range 1–42). Of 209 AKs, 92 (44%) were AK1, 88 (42%) were AK2 and 29 (14%) were AK3.
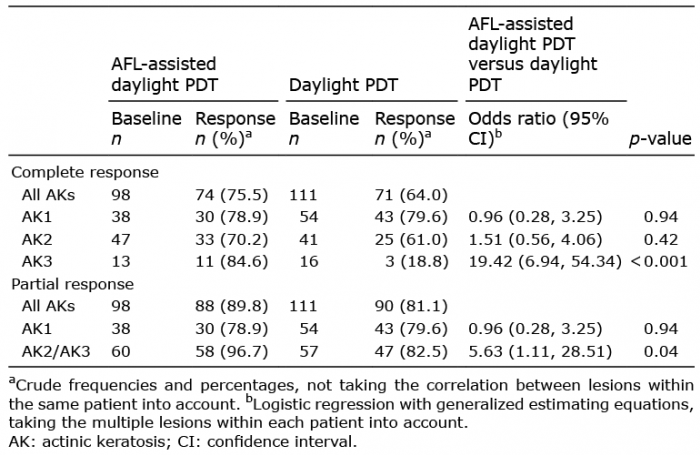
At 4 months follow-up, overall complete response was 75.5 % in areas treated with AFL-assisted daylight PDT and 64.0 % in areas treated with daylight PDT (Table I). There was a significant interaction between complete response and AK grade (p = 0.001), as well as between partial response and AK grade (p = 0.007), meaning that treatment effect differed according to AK grade. Complete response for AK3 lesions was significantly higher in areas treated with AFL-assisted daylight PDT than in areas treated with daylight PDT only (OR 19.42; 95% CI 6.94, 54.34). Partial response for AK2/AK3 lesions was significantly higher in areas treated with AFL-assisted PDT (OR 5.63; 95% CI 1.11, 28.51) (Table I).
Patient-reported pain was significantly higher in areas treated with AFL-assisted PDT in the first two days (p-values 0.008, 0.02 and 0.03), but not after 5 days (p = 0.11). All patients developed some degree of local inflammation and crusting.
Table I. Clinical findings at baseline and response at 4 months follow-up after ablative fractional laser (AFL)-assisted daylight photodynamic therapy (PDT) and daylight PDT
In this small study, AFL-assisted daylight PDT was superior to daylight PDT in the treatment of thick AKs of the scalp and forehead in OTRs. AFL-assisted daylight PDT was more painful than daylight PDT.
Conventional PDT is increasingly used in the treatment of AKs and field cancerization in OTRs with reported response ranging from 56 to 72% (7–9). Some studies suggest that conventional PDT is less effective in OTRs than in immunocompetent patients, with possible explanations being a higher number of AKs, increased hyperkeratosis inhibiting the absorption of the photosensitizer, and reduced immune response (10). The purpose of AFL-treatment before PDT is to increase the absorption of photosensitizer, especially in thick AK lesions (3). In one study among immunocompetent patients, AFL-assisted convential PDT was found to be more effective than convential PDT (11), but another study did not find any difference (12). In the first study of this kind in OTRs, AFL-assisted daylight PDT was found to be superior to daylight PDT alone in the treatment of AKs and field cancerization on scalp, chest and extremities (13). The results in our small study support these findings, although a statistical significant effect was found only for thick lesions.
In some studies, daylight PDT induced less pain than conventional PDT (14, 15). This may be explained by a continous production and activation of protoporphyrine IX during daylight PDT yielding less pain than rapid activation of accumulated protoporphyrine IX in conventional PDT (14). In our study, patient-reported pain was higher in areas treated with AFL-assisted daylight PDT than in areas treated with daylight PDT only, probably reflecting a higher phtotoxic activity and improved clinical response.
Statistical analyses in our study were based on multiple AKs in all patient, and the randomization were performed on treatment areas with multiple AKs, not on patients (Fig. S1). Nevertheless, the study is small, and the results should be interpreted with caution. Each pair of treatment areas received the same amount of sun exposure, so possible differences in weather conditions between patients did not have any significant impact on the results. Other limitations are short follow-up time, no comparison with untreated areas with AKs, no evaluation of cosmesis, and no evaluation of costs. AFL-pretreatment do complicate the PDT procedure and adds costs, probably limiting its usefulness in clinical practice.
We conclude that AFL-assisted daylight PDT in this small study was superior to daylight PDT in the treatment of thick AKs on the scalp and forehead in OTRs, indicating that AFL-assisted daylight PDT, although more expensive, may be a viable treatment option in such patients.
Dr. Linn Landrø and Dr. Ingrid Roscher are acknowledged for recruiting patients to the study.


 Click to show fullsize
Click to show fullsize