


1Department of Dermatology, Mehiläinen Länsi-Pohja Oy, Kemi, 2Department of Dermatology and Medical Research Center Oulu, PEDEGO Research Unit, University of Oulu, Oulu University Hospital, 3Faculty of Medicine, University of Oulu, Oulu, 4Jyväskylä Health Centre, Jyväskylä, and 5Infrastructure for Population Studies, Faculty of Medicine, University of Oulu and Unit of General Practice, Oulu University Hospital, Oulu, Finland
#These authors contributed equally.
Pemphigus is an autoimmune skin disease characterized by blistering and erosions of the skin and mucous membranes. Pemphigus is rare in Northern and Western Europe, but its incidence is higher around the Mediterranean Sea. The most common type worldwide is pemphigus vulgaris. The aim of this study was to investigate the incidence of pemphigus subtypes in Northern Finland between 1985 and 2017. A total of 46 patients diagnosed with pemphigus at the Department of Dermatology of Oulu University Hospital were found; the female/male ratio was 1.7. In contrast to many other countries, it was found that, in Northern Finland, the superficial pemphigus subtypes were the most common: erythematosus or foliaceus (65%) followed by pemphigus vulgaris (26%). Over the past 4 decades the annual incidence of pemphigus in Finland has increased from 0.76 to 2.8 cases per million persons.
Key words: autoimmune blistering skin disease; pemphigus; epidemiology; incidence; Finland.
Accepted Aug 8, 2019; E-published Aug 9, 2019
Acta Derm Venereol 2019; XX: XX–XX.
Corr: Anna-Kaisa Försti, Mehiläinen Länsi-Pohja Oy, Department of Dermatology, Kauppakatu 25, FIN-94100 Kemi, Finland. E-mail: anna-kaisa.forsti@student.oulu.fi
Pemphigus comprises a group of autoimmune skin diseases characterized by blistering and erosions of the skin and mucous membranes. Pemphigus is rare in Northern and Western Europe, but its incidence is higher around the Mediterranean Sea. The most common type worldwide is pemphigus vulgaris. To the best of our knowledge, there are no recent reports of the incidence of pemphigus in Nordic populations. The latest study into the incidence of pemphigus in Finland is from the 1970s. However, the incidence may have been affected, for example, by immigration. This is a retrospective database study of all patients with pemphigus diagnosed in the Oulu University Hospital between 1985 and 2017. The current study included 46 patients, and interestingly, the most prevalent subtype was superficial pemphigus foliaceus or erythematosus (65%). This study also reports comorbidities of study patients and treatments used for pemphigus in the Oulu University Hospital.
Pemphigus comprises a group of rare autoimmune bullous diseases, characterized by the production of autoantibodies against desmogleins, a family of epidermal adhesion proteins. Autoantibodies against desmogleins (Dsg) 1 and 3 cause loss of intraepidermal adhesion, resulting in epidermal acantholysis, blistering and erosions of the skin and mucous membranes (1–4). Due to the rarity of pemphigus and the diversity of its variants, it is challenging to distinguish the different types of pemphigus using clinical findings alone. Therefore, diagnosis of pemphigus relies on direct and indirect immunofluorescence microscopy, serology and histopathology. The gold standard diagnostic technique is direct immunofluorescence microscopy of skin biopsy, which reveals intercellular binding of immunoglobulin G (IgG) and/or complement 3 (C3) within the epidermis. In addition, Dsg antibodies are detectable by enzyme linked immunosorbent assays (ELISA) of patient sera, and the histology of skin biopsy can help to determine the sub-type of pemphigus (3, 4).
The 2 main forms of pemphigus are pemphigus vulgaris (PV) and pemphigus foliaceus (PF). A third notable type is paraneoplastic pemphigus, which is a rare variant associated with malignancies and a more severe clinical phenotype (2). An essential difference between PV and PF is the degree of mucosal involvement and serological status. PV generally begins in the oral mucous membranes and can be manifested in the skin, whereas PF typically exhibits skin symptoms only, with no mucosal involvement (5). In both PV and PF, the disease can be manifested in the skin, and Dsg 1 antibodies are then present. In PV manifesting solely on the mucous membranes, only Dsg 3 antibodies are detected. Dsg 1 and 3 antibodies also correlate with disease activity (2, 4). Pemphigus vegetans is a special form of PV, in which symptoms are predilected to axillary, umbilical, mammary and other intertriginous areas. Papillomatosis and fissured vegetation may develop. PF has its own variant, pemphigus erythematosus (PE), which resembles PF clinically, but usually has a less severe clinical manifestation that is limited to the face (1).
The incidence of pemphigus varies significantly by geographical region and ethnicity. The reported incidence of PV varies from 0.78 to 16.1 per million persons per year (1, 6). It is lowest in Northern and Western Europe, and highest in Israel and other Mediterranean areas (1, 6). The presence of certain HLA class II alleles predispose some populations to pemphigus, particularly HLA-DRB1*04, which is common among Ashkenazi Jewish patients with PV (1). PF, for its part, is particularly common in some rural areas of Brazil, which is why it is also known as endemic PF (fogo selvagem (‘wild fire’) in Portuguese) (1, 6–8). In a British population-based study, 1-year mortality among patients with PV was 12%, 3 times higher than that of an age- and sex-matched population (9). PF generally has a better prognosis than PV, and a lesser or non-existent effect on mortality (1, 2).
Patient records with the International Statistical Classification of Diseases and Related Health Problems (ICD) codes for pemphigus (694 in ICD-8, 6944 in ICD-9, and L10 in ICD-10) were extracted from the Oulu University Hospital database. All of the patient records were checked by the authors. The study included all patients treated in the outpatient clinic and those admitted to the hospital between 1985 and 2017, whose pemphigus diagnosis was confirmed by positive direct or indirect immunofluorescence analysis (3). Data on the general population in the Northern Ostrobothnia Hospital District (NOHD) were provided by Statistics Finland (www.tilastokeskus.fi). Statistical analyses were performed using IBM SPSS statistics and Stata version 13 (Stata Statistical Software: Release 13, College Station, TX, USA: StataCorp LP, 2013). The crude incidence rate was calculated as the ratio of the number of new cases of pemphigus between 1985 and 2017 to the mean number of individuals who were at risk. Approval of the study methods was obtained from the medical director of Oulu University Hospital. Since this study was based on health records, the agreement of the ethics committee was not required.
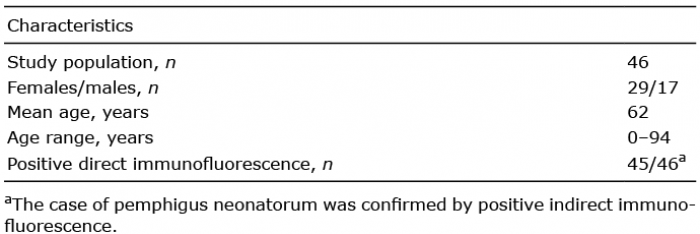
Between 1985 and 2017, 46 patients were diagnosed with pemphigus in Oulu University Hospital, which has the only department of dermatology in the NOHD. There were 29 females (63%) and 17 males (37%), a female/male ratio of 1.7. Mean age at diagnosis was 62 years (median 65 years) and the range varied from 0 to 94 years. When one case of pemphigus neonatorum was excluded, the youngest patient was 21 years old (Table I). One patient was originally from Southern Europe, the others were born in Finland.
Table I. Characteristics of the study population
The crude annual incidence of pemphigus in the NOHD between 1985 and 2017 was 2.8 new cases per 1 million persons (95% confidence interval (95% CI) 2.0–3.9). Eleven patients, despite having been treated in the Oulu University Hospital, had been referred there from other hospital districts, and were therefore excluded from the incidence calculations. When we analysed the number of new cases of pemphigus in the years 1985–2017, taking into account the increase in the general population in the NOHD area from 340,863 to 409,043 in that time period, we found no overall or seasonal change in the incidence of pemphigus.
Of the diagnoses, 30/46 (65%) were defined as superficial pemphigus, which covers PE and PF. Diagnosis of PV accounted for 12/46 cases (26%). In addition, there was 1 case each of pemphigus vegetans; pemphigus herpetiformis; pemphigus neonatorum, and IgA pemphigus (Fig. 1). In 7 of the superficial pemphigus cases it could not be determined retrospectively whether the diagnosis was PF or PE, but, excluding these cases, the most prevalent diagnosis was PE, with 14 cases.
Fig. 1. Subtypes of pemphigus in Northern Finland 1985–2017.
In all cases the clinical features were consistent with the diagnosis. The diagnosis was confirmed by direct immunofluorescence microscopy in 45/46 (97.8%) of cases, and histology in 31/43 (72.1%) of cases. Indirect immunofluorescence was positive in 23/31 (74.2%) of cases, and Dsg 1 and/or 3 IgG antibodies could be detected by ELISA in 19/24 (79.2%) of cases. Not all of the diagnostic tests were performed in all cases, and ELISA was not available in the Oulu University Hospital before 2002.
The disease manifested solely on the skin in 28/29 patients with PF or PE. One patient with PF had very mild symptoms in the oral mucosa. Seven of the 12 patients with PV had symptoms only in the mucous membranes, 4 in both the skin and mucous membranes, and 1 in the skin only.
Used in 25/46 (54%) of cases, the most common first-line treatment was topical glucocorticoids. In one-third (15/46; 33%) of patients treatment was started with systemic glucocorticoids, with a mean starting dose of 50 mg (range 15–200 mg) of prednisolone per day (1). Dapsone and tetracycline were each used as initial treatment in 2 cases.
In this study, the prevalence of pre-selected comorbidities was recorded as follows: cardiovascular diseases occurred in 17/46 (37%) patients, other skin diseases in addition to pemphigus in 15/46 (33%), neurodegenerative diseases in 3/46 (6%), type II diabetes in 3/46 (6%), other autoimmune diseases in 3/46 (6%), and malignancy in 2/46 (4%).
This study found that the annual incidence of pemphigus in Finland has increased to 2.8 new cases per million inhabitants from 0.76 in the 1970s (10). To the best of our knowledge, there are no other recent reports of the incidence of pemphigus in Nordic countries, although the prevalence of pemphigus in Denmark was 70 per million inhabitants (11). The increase of the incidence in Finland (12) is probably partly explained by improvements over time in diagnostic techniques and increased awareness of the disease. Pemphigus is comparatively rare in contemporary Nordic populations (1, 6), and it is possible that immigration may in future increase the number of patients with pemphigus in Finland. However, since only 1 person in our study population was not of Finnish origin, immigration does not explain the increase seen so far. Some previous studies have suggested that the incidence of pemphigus is increasing, possibly also as a result of ageing populations (9, 13), but not to the same extent as the other autoimmune blistering skin disease, bullous pemphigoid (9, 13, 14). At 2.8 cases per million persons per year, the current incidence of pemphigus in Finland is close to reported rates in Mali (2.9) and Mediterranean Turkey (2.4) (1, 15, 16). Surprisingly, it is markedly higher than rates previously reported for Germany (0.5–0.8) and Switzerland (0.6), but less than reported for Southern European countries (6, 12, 17, 18).
At 62 years, the mean age of pemphigus onset in Finland is relatively high, and at the same level that has previously been reported for Germany and Switzerland (12, 17). In Southern Europe, the mean age at onset of pemphigus mostly varies between 50 and 60 years (1, 6). The mean age at presentation of endemic PF is remarkably low, with most patients aged under 40 years at onset (1, 6, 8, 19). The female predominance found in this study is typical of pemphigus (1, 6).
Interestingly, the most prevalent subtype of pemphigus in Finland is PF/PE, which accounted for 30/46 (65%) cases in this study. The same finding was previously seen in a study by Hietanen & Salo in 1982, with PE being the most common subtype (10). Worldwide, sporadic PF is considered to be rare, covering about 20–30% of cases of pemphigus, and PE is far rarer still (1, 6). In this study population, some cases of superficial pemphigus had been diagnosed as PE, even in the absence of clear immunofluorescence in the dermo–epidermal junction, or the detection of antinuclear antibodies. It is therefore questionable whether these cases in fact may represent PF. There were a few rarer pemphigus types in our population, including pemphigus vegetans, pemphigus herpetiformis, pemphigus neonatorum, but no cases of paraneoplastic pemphigus.
Cardiovascular diseases and skin diseases other than pemphigus were the most common comorbidities, being present in over one-third of cases. Previous studies have reported other autoimmune diseases being overrepresented among patients with pemphigus, including autoimmune thyroid diseases, type 1 diabetes, and rheumatoid arthritis (20, 21). Autoimmune diseases occurred in 6% of our patients with pemphigus, which is a similar rate to the 4% reported in Danish National Patient Registers (11). However, it is possible that some diagnoses of auto-immune diseases may not have been revealed by the current database search, if they were reported in health organizations other than the Oulu University Hospital. Malignancies were diagnosed in 4% of our patients either before or after pemphigus diagnosis. No association of pemphigus with malignancies has yet been unambiguously established, with the exception of paraneoplastic pemphigus. In a German study, PV was associated with haematological, oropharyngeal, gastrointestinal, and colon cancer, while PF was associated with non-melanoma skin cancer (22).
Glucocorticoids have been the mainstream therapy for pemphigus since their introduction in the 1950s. Systemic glucocorticoids act rapidly and are usually effective, but their long-term use is limited by side-effects (3, 23) (European Dermatology Forum (EDF) guideline, https://www.edf.one/home/Guidelines/EDF-Guidelines.html). In our study, topical corticosteroids were the most common first-line treatment (used in 54% of cases), which is understandable because 65% were diagnosed with PF or PE. European guidelines recommend azathioprine and mycophenolate mofetil as first-line adjuvant immunosuppressive therapy in pemphigus (EDF guideline), and these are widely used, especially in PV. The British Association of Dermatologists’ 2017 guideline for PV adds rituximab to the list of first-line adjuvants (24). Many other immunosuppressants, such as cyclo-phosphamide, dapsone, methotrexate, and intravenous immunoglobulin, have also been used in combination with prednisolone. A recent review comprehensively discusses medications used in PV and recommended treatment strategies (23).
The strength of this study is a long follow-up period of over 30 years, and the fact that all diagnoses of autoimmune bullous skin diseases in the NOHD area are made at the Oulu University Hospital’s Department of Dermatology. Thus, it is reasonably safe to conclude that the study was able to capture all cases of pemphigus during the study period. The study is limited by a relatively small population due to the rarity of the disease in Finland. Further studies are needed to provide more information about the changes in incidence of pemphigus. More prospective, randomized, and controlled studies are also required in order to investigate therapeutic options for patients with pemphigus and to develop evidence-based treatment strategies.


 Click to show fullsize
Click to show fullsize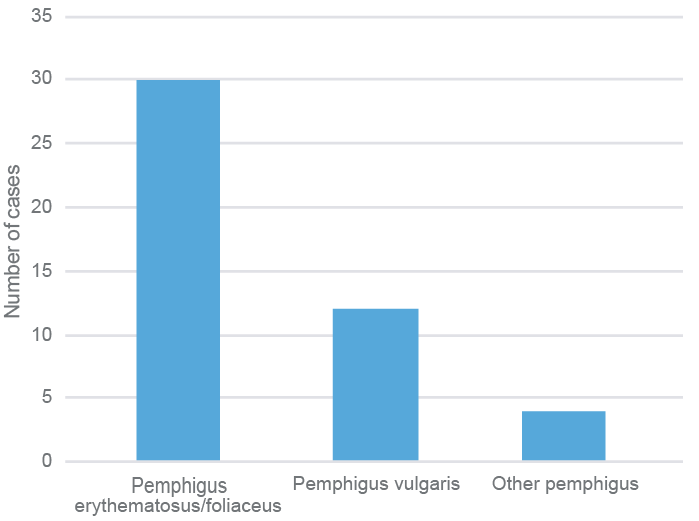 Click to show fullsize
Click to show fullsize