


1Department of Dermatology, University Hospital La Zarzuela, Madrid, 2Faculty of Medicine, University of Granada, 3Department of Dermatology, University Hospital San Cecilio, 4Department of Dermatology, University Hospital Virgen de las Nieves, and 5Institute of Biosanitary Investigation ibs. Granada, Spain
Frontal fibrosing alopecia has been related to some auto-immune diseases, but the association with rosacea is not clear. The objective of this study was to analyse the prevalence of rosacea in a group of patients with frontal fibrosing alopecia. A cross-sectional study, including 99 women with frontal fibrosing alopecia and 40 controls, was performed, in which clinical, dermoscopic and hormonal data were analysed. Women with frontal fibrosing alopecia presented a higher prevalence of rosacea than the controls did (61.6% vs. 30%, p = 0.001), especially those with severe grades of alopecia (77.8% in grade V vs. 33.3% in grade I, p = 0.02). Binary logistic multivariate analysis showed that perifollicular erythema (odds ratio (OR) 8.5; 95% confidence interval (95% CI) 1.73–42.30), higher body mass index (OR 1.16; 95% CI 1.01–1.34) and lower progesterone levels (OR 0.15; 95% CI 0.028–0.89) were associated with a higher risk of rosacea in patients with frontal fibrosing alopecia. In conclusion, patients with frontal fibrosing alopecia presented a higher prevalence of rosacea than did controls. Perifollicular erythema, higher body mass index and lower progesterone levels were associated with a higher risk of rosacea in the group with frontal fibrosing alopecia.
Key words: frontal fibrosing alopecia; scarring alopecia; cicatricial alopecia; rosacea; hormones; comorbidity.
Accepted Aug 12, 2019; E-published Aug 13, 2019
Acta Derm Venereol 2019; XX: XX–XX.
Corr: Mª Librada Porriño-Bustamante, Department of Dermatology, University Hospital La Zarzuela, Calle de Pleyades, 25, ES-28023 Madrid, Spain. E-mail: mporrinobustamante@gmail.com
The association between frontal fibrosing alopecia and rosacea is not clear. In this cross-sectional study, including 99 women with frontal fibrosing alopecia and 40 controls, women with frontal fibrosing alopecia presented a higher prevalence of rosacea than the controls did (61.6% vs. 30%), especially those with severe grades of alopecia (77.8% in grade V vs. 33.3% in grade I). Moreover, perifollicular erythema, higher body mass index and lower progesterone levels were associated with a higher risk of rosacea in the group with frontal fibrosing alopecia.
Frontal fibrosing alopecia (FFA) is a lymphocytic scarring alopecia characterized by progressive recession of the frontal and temporoparietal hairline with loss of follicular openings. The eyebrows are often affected, and sometimes also the eyelashes and body hair (1). Typical dermoscopic findings include perifollicular erythema and hyperkeratosis (2). Lonely hair sign occurs in some patients (3).
Despite the initial description of FFA in postmenopausal women, increasing number of cases in premenopausal women have been described (4). Moreover, some men with FFA and familial cases have also been reported (2). The pathogenesis of this disease is not well known and autoimmunity, genetic, hormonal, and environmental factors may play a role. Lichen pigmentosus, discoid lupus or vitiligo have been associated with FFA (5–7). Recently, a cross-sectional study without a control group found that 34% of patients with FFA presented rosacea. In this study erythematotelangiectatic rosacea was the most frequent subtype, followed by papulopustular rosacea (8).
Rosacea is an inflammatory skin condition characterized by recurrent or persistent episodes of centrofacial erythema (9). Rosacea is more frequent in women (female: male ratio 2–3:1), typically aged between 30 and 50 years, and is considerably more common in light-skinned people. The lesions predominate on the cheeks and chin in women, and on the nose in men. The National Rosacea Society (NRS) Expert Committee recognizes 4 subtypes, which frequently overlap (i.e. erythematotelangiectatic, inflammatory papulopustular, phymatous and ocular rosacea) (10, 11). Moreover, a single variant, namely granulomatous or lupoid rosacea, is also recognized (10). This classification was proposed in 2002 and has been used worldwide to compare data about rosacea, although recently the NRS has proposed a new classification based on phenotypes (12).
The association between FFA and rosacea is not clear, although rosacea-like lesions have been reported on the cheeks in patients with FFA (i.e. perifollicular erythema, sometimes with follicular keratosis, such as keratosis pilaris-like papules) (13, 14).
The objectives of this study were to analyse the prevalence of rosacea in a group of women with FFA compared with a control group, and to explore associated factors.
A cross-sectional study with a control group was performed in the University Hospital of Granada, Spain. Patients with a clinical diagnosis of FFA and controls were included. Inclusion criteria for patients were: age over 18 years, absence of active hormonal therapies, and recession of the frontal and/or temporoparietal hairline, with typical dermoscopic features of FFA, i.e. loss of follicular openings with or without perifollicular erythema and scaling. Eye-brow loss may sometimes be present. A control group with women consulting the Dermatology Department for other reasons (naevi, seborrhoeic keratosis, etc.) was included. The exclusion criteria for controls were the presence of any primary scarring alopecia. All patients and controls signed an informed consent and the project was approved by the local ethics committee.
Age, menarche and age of menopause, and time of evolution of FFA were obtained. The weight and height of participants were measured, and their body mass index (BMI) (kg/m2) was calculated. Personal history of diabetes, hypertension or dyslipidaemia was recorded. Moreover, the use of sunscreens by the participants was also registered. The severity of the alopecia was assessed using a classification that includes 5 grades of severity and is determined by measuring the area of cicatricial skin between the initial hairline and the recessed one, in the frontal and temporal region. The largest of these areas was used to define severity, with the following grades: I (< 1 cm), II (1–2.99 cm), III (3–4.99 cm), IV (5–6.99 cm) and V (≥ 7 cm, also called “clown alopecia”) (15). Also, typical signs of FFA, such as perifollicular hyperkeratosis/erythema, lonely hair sign and facial papules, were collected. The presence of pruritus of the scalp or trichodynia were also registered. Diagnosis of rosacea was based on clinical history and physical examination (fixed facial erythema and telangiectasias, facial flushing, papules, pustules or phymatous lesions). The subtypes of rosacea considered were erythematotelangiectatic, inflammatory papulopustular, and phymatous. Clinical information regarding other skin diseases, such as vitiligo, lichen planus or psoriasis, was also obtained.
Blood tests searching for hormonal anomalies were performed in both groups, including follicle-stimulating hormone (FSH), luteinizing hormone (LH), oestradiol, progesterone, testosterone, sex hormone binding globulin (SHBG), prolactin (PRL), 17-hydroxy-progesterone, dehydroepiandrosterone sulphate (DHEAS), androstenedione and dihydrotestosterone.
Student’s t-test was applied to compare mean values of quantitative variables, the Shapiro–Wilk test to examine the normality of their distribution, and the Levene’s test to study the variance. Qualitative variables were analysed with χ2 test or, when conditions for this test were not fulfilled, with Fisher’s exact test. Binary logistic regression model was performed to analysed factors associated with rosacea in patients with FFA. Differences were considered significant at p ≤ 0.05 and nearly significant at p ≤ 0.1. Software (SPSS 20.0, SPSS Inc., Chicago, IL, USA) was used for data analyses.
This study included 99 women with FFA and 40 controls. No significant differences between patients and controls were detected regarding age (63.3 vs. 61.7 years, p = 0.26), age of menarche (12.6 vs. 13 years, p = 0.17), age of menopause (50.4 vs. 49.9 years, p = 0.49) for patients and controls, respectively. Ten percent of patients with FFA and 10.1% of controls were premenopausal (p = 0.98). Patients with FFA presented higher significant weight and BMI than controls (68.9 vs. 63.6 kg, p = 0.012; 28.7 vs. 26.4 kg/m2, p = 0.013) without differences in height (155 vs. 156.6 cm, p = 0.23). Regarding personal history of hypertension (45.5% vs. 40%), diabetes (14.1% vs. 12.5%) or dyslipidaemia (44.4% vs. 42.5%), no significant differences were observed between patients and controls. Four percent of patients were active smokers vs. 15% of controls (p = 0.07) and, regarding alcohol intake, 39.4% of patients and 45% of controls drank less than 40 g/day and 60.6% of patients and 55% of controls did not drink any alcohol (p = 0.69). Regarding the use of sunscreens, 83.2% of patients with FFA and 62.5% of controls used them (p = 0.014).
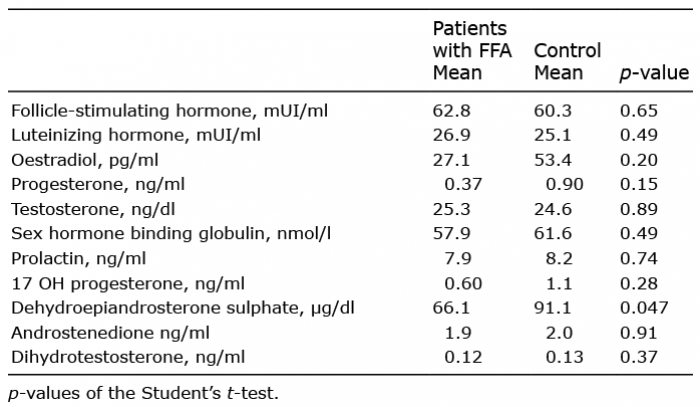
Sex hormone values are summarized in Table I, and no significant differences were observed between patients and controls, except in dehydroepiandrosterone sulphate (66.1 vs. 91.9 μg/dl, p = 0.047, for patients with FFA and controls, respectively). Of the patients with FFA, 30.3% presented androgenetic alopecia and no significant differences in prevalence of psoriasis, vitiligo or lichen planus were observed between patients and controls.
Table I. Serum hormonal levels in patients with frontal fibrosing alopecia and controls
The mean age of onset of FFA was 58.7 years and the mean duration of the disease was 58.8 months. The severity of FFA in the sample of patients was: 3% grade I, 42.4% grade II, 34.3% grade III, 11.1% grade IV and 9.1% grade V. Of patients with FFA, 74.7% had pruritus and 18.2% had trichodynia. Erythema, follicular hyperkeratosis, facial papules and lonely hair sign were observed in 86.9%, 92.9%, 16.2% and 70.7%, respectively. Eyebrow alopecia presented in 83.8% and eyelash alopecia in 27.3%. Alopecia at other body sites presented as follows: 13.1% occipital, 88.9% arms, 92.9% legs, 56.6% axilla, and 42.4% pubis.
Clinical signs of rosacea presented in 61.6% of patients compared with 30% in the control group (p = 0.001). Erythematotelangiectatic rosacea was the most frequent form (88.5% [54/61]) (Fig. 1a, b), followed by the papulopustular form (11.5% [7/61]) (Figs 2a, b and 3a, b). Patients with more severe FFA were more likely to have rosacea than those with mild grades of alopecia (prevalence of rosacea 77.8% in grade V vs. 33.3% in grade I, p = 0.02) (Table II). No statistically significant differences regarding rosacea were encountered in patients related to menopause; being the percentage of rosacea in menopausal patients 61.8% vs. 60% in non-menopausal patients (p = 0.91). No significant differences were observed in age of menarche (12.6 vs. 12.6 years, p = 0.98) or menopause (50 vs. 50.2 years, p = 0.68) regarding the presence of rosacea. Pruritus or trichodynia were not related to a higher prevalence of rosacea. Regarding clinical signs of FFA, the presence of perifollicular erythema (Figs 1c, 2c and 3c) correlated significantly with rosacea (64.7% in patients with rosacea vs. 32.6% in patients without rosacea; p = 0.002), whereas perifollicular hyperkeratosis (Figs 2c and 3c) did not show that correlation (60.9% in patients with rosacea vs. 39.1% in patients without rosacea; p = 0.58). Neither facial papules nor lonely hair sign match the presence of rosacea. No correlation was found between duration of FFA and rosacea, or between presence of rosacea and alopecia of the eyelashes, eyebrows or occipital area.
Fig. 1. (a) Frontal side: intense centrofacial fixed erythema with telangiectasias in a patient with grade II frontal fibrosing alopecia. (b) Lateral view: erythema and telangiectasias on the cheek. (c) Dermoscopy showing loss of follicular openings and marked perifollicular erythema. Permission from the patient is given to publish these photos.
Fig. 2. (a) Frontal side: mild centrofacial fixed erythema with telangiectasias and small papules in the glabellar area and on the cheeks and nose, in a patient with grade III frontal fibrosing alopecia. (b) Lateral view: erythema and telangiectasias on the cheek, and few small papules. (c) Dermoscopy showing loss of follicular openings and perifollicular hyperkeratosis and mild erythema. Permission from the patient is given to publish these photos.
Fig. 3. (a) Frontal side: small papules and pustules in the glabellar area surrounded by mild erythema, in a patient with grade IV frontal fibrosing alopecia. (b) Lateral side: small papules and pustules also in the chin and temple. (c) Dermoscopy showing loss of follicular openings and intense perifollicular erythema with hyperkeratosis. Permission from the patient is given to publish these photos.
Table II. Prevalence of rosacea according to the grades of frontal fibrosing alopecia (FFA)
Alcohol and tobacco were not associated with the presence of rosacea in patients with FFA. However, patients with FFA and rosacea presented higher means weight (71.1 vs. 65.4 kg, p = 0.016) and BMI (29.5 vs. 27.3 kg/m2, p = 0.016) than patients without rosacea. Patients with FFA and rosacea did not present a higher prevalence of diabetes, hypertension or dyslipidaemia. There were no statistically significant differences in the use of sunscreens in patients with FFA and rosacea and those with FFA but no rosacea (82.5% vs. 84.2%, respectively; p = 0.82).
Data regarding hormones in patients with FFA with or without rosacea are summarized in Table III. No significant differences were observed between groups, except in levels of luteinizing hormone (LH), progesterone and dihydrotestosterone, which were lower in patients with rosacea and FFA.
Table III. Serum hormonal levels in patients with frontal fibrosing alopecia (FFA) and rosacea and patients with FFA without rosacea
Binary logistic regression analysis in patients with FFA is shown in Table IV. Perifollicular erythema, BMI and progesterone levels were associated with presence of rosacea in patients with FFA.
Table IV. Binary logistic regression analysis in patients with frontal fibrosing alopecia (FFA) and rosacea
Women with FFA presented a higher prevalence of rosacea than the controls did. The most frequent subtype was erythematotelangiectatic rosacea. Severe grades of alopecia were associated with a higher prevalence of rosacea. Multivariate analysis has shown that perifollicular erythema, higher BMI and lower progesterone levels were associated with a higher risk of rosacea in patients with FFA. Menopause or diseases such as diabetes, hypertension or dyslipidaemia were not associated with a higher risk of rosacea.
The prevalence of FFA is currently increasing progressively. Continuous characterization of this disease has been achieved since its description in 1994 by Kossard (16), but several enigmas remain unresolved. Most patients with FFA are women, and the mean age of patients and the mean age of onset of FFA in this study were similar to those in previous reports (15). The majority of patients presented grades II and III alopecia, representing more severe disease than in previous series (15). Typical facial findings of patients with FFA include facial papules, which are thought to be due to involvement of vellus hair, and red dots in the glabella and eyebrows, representing perifollicular inflammation (17, 18).
FFA has been reported to occur concurrently with androgenetic alopecia (2). Autoimmune diseases, such as vitiligo, discoid lupus erythematous, thyroid dysfunction and Sjögren syndrome, have been previously reported to occur simultaneously with FFA in up to 30% of cases (7, 19–21). Moreover, reports of both FFA and lichen planus or lichen planus pigmentosus have been published (5, 22, 23). The association between FFA and rosacea has not been reported clearly, although a recent cross-sectional study without a control group reported a prevalence of 34% for rosacea in patients with FFA. In the current study the prevalence of rosacea was significantly higher than in the control group (8).
Rosacea is a common chronic cutaneous inflammatory disease, mainly affecting the facial area, characterized by flares of centrofacial erythema (flushing or transient erythema), causing a characteristic centrofacial fixed ery-thema, often with telangiectasias. Papules and pustules or less frequently, phymas, may also appear. The cause of rosacea is unknown and probably multifactorial (24). The National Rosacea Society Expert Committee differentiates 4 main subtypes, which frequently overlap, i.e. erythematotelangiectatic, inflammatory papulopustular, phymatous and ocular rosacea (10, 11, 24). The prevalence of this disease is estimated as 22% in the general population, although in our study the prevalence in controls was slightly higher, perhaps because it referred to a specific sex and age group (25).
Rosacea has been associated with migraine (suggesting a vascular abnormality), depression, hypertension, dyslipidaemia, coronary artery disease, and other chronic systemic illnesses, although it may be explained by shared environmental or lifestyle factors rather than by a common genetic predisposition (9, 26–29). An increased prevalence of Helicobacter pylori infection has also been found (30). Recently, rosacea has been linked to a cluster of autoimmune diseases, such as type 1 diabetes mellitus, coeliac disease, multiple sclerosis and rheumatoid arthritis. All of these were significantly associated with rosacea in women; whereas the association in men only reached statistical significance for rheumatoid arthritis (9). The genetic component of rosacea could be stronger than assumed so far, and autoimmune inflammatory pathways could contribute to the disease course (9). In this study multivariate analysis revealed that rosacea was significantly associated with higher BMI. A recent study has shown that the risk of rosacea was elevated for those with increased BMI and greater waist and hip circumference in a 14-year follow-up study (31).
Keratosis pilaris-like papules over the forehead and cheeks and follicular erythema on the cheeks have been described in a few patients with FFA (13). Moreover, a recent study found diffuse erythema on the cheeks, forehead or eyebrows, sometimes with a reticular pattern, more visible over the zygomatic area (14). These findings matched with follicular and interfollicular lichenoid infiltrate. Some women in this study also reported episodes of flushing linked to thermal or emotional changes (14). In our study, perifollicular erythema, but not perifollicular hyperkeratosis, was significantly associated with the presence of rosacea after multivariate analysis. A common inflammation of the pilosebaceous unit may be involved in the pathogenesis of rosacea and FFA. Prostaglandin D2 has been reported to inhibit hair growth (32), and has been involved in the development of rosacea (33).
Hormonal factors have been suggested to play an important role in the pathogenesis of FFA due to the higher prevalence of this type of alopecia in postmenopausal women and the response to anti-androgenic drugs. Androgen deficiency was identified in 30% of women with FFA in a recent study (34). However, hormonal levels are not altered in premenopausal women diagnosed with FFA (35). In our study no differences were found in hormonal levels between patients with FFA and controls, with the exception of dehydroepiandrosterone sulphate (DHEA-S), a mainly adrenal hormone, which was lower in patients with FFA. This hormone is elevated in hyperandrogenism and its deficiency in FFA women could be related to the androgen deficiency described previously. Dehydroepi-androsterone (DHEA) is an immunomodulatory hormone essential for peroxisome proliferator-activated receptor (PPAR) functions, and is reduced in some processes characterized by fibrosis, such as idiopathic pulmonary fibrosis (36, 37). PPARγ is the main regulator of lipid cell metabolism and sebocyte development, and is indispensable for the maintenance of stem cells of functional epithelium in hair follicles (38). Deletion of the PPARγ gene in the follicular bulge resulted in a process similar to lichen planopilaris (38, 39). In addition, PPAR is a negative regulator of transforming growth factor-beta 1 (TGFβ1), which promotes fibrotic events (36). Therefore, the reduced activity of this hormone may be related to the fibrogenic inflammatory process of FFA. However, it is important to note that the evaluation of the hormone in the blood does not necessarily reflect the degree of local action at the hormone receptors, therefore patients with normal values may have an impairment in the sensibility or the integrity of the target receptor, as occurs in androgenetic alopecia (40). No relationship between DHEA-S and rosacea has been reported.
In patients with FFA and rosacea, significantly lower serum levels of progesterone were detected by multivariate analysis. Progesterone has not been clearly implicated in the pathogenesis of rosacea; there is only one case report of an association between a progesterone-releasing intrauterine contraceptive device and rosacea (41).
Since the study of Aldoori et al. (42), suggesting a possible association between the use of sunscreens and moisturizers and the development of FFA, an increasing number of publications considering them as a possible trigger in the development of FFA have been reported (43, 44). In accordance with previous reports, the use of sunscreens was higher in the group of patients with FFA than in controls. However, despite the fact that people with rosacea are likely to use more sunscreens than people with no skin disease, there were no statistically significant differences in the use of sunscreens in patients with FFA and rosacea and those with FFA but no rosacea. On the other hand, it is not known whether the higher use of sunscreens in patients with FFA is a cause or consequence of the alopecia (45).
In conclusion, women with FFA presented a higher prevalence of rosacea, and severe grades of alopecia were associated with a higher prevalence of rosacea. Perifollicular erythema, higher BMI and lower progesterone levels were associated with a higher risk of rosacea in patients with FFA. Lower levels of dehydroepiandrosterone sulphate may be implicated in the pathogenesis of FFA. Further studies are required to confirm this association and the pathogenic implications of the risk factors.
This article is part of María Librada Porriño-Bustamante’s PhD.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize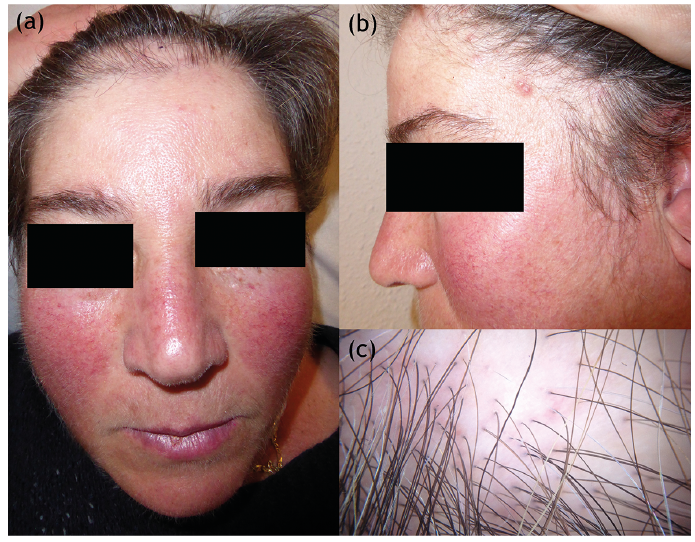 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize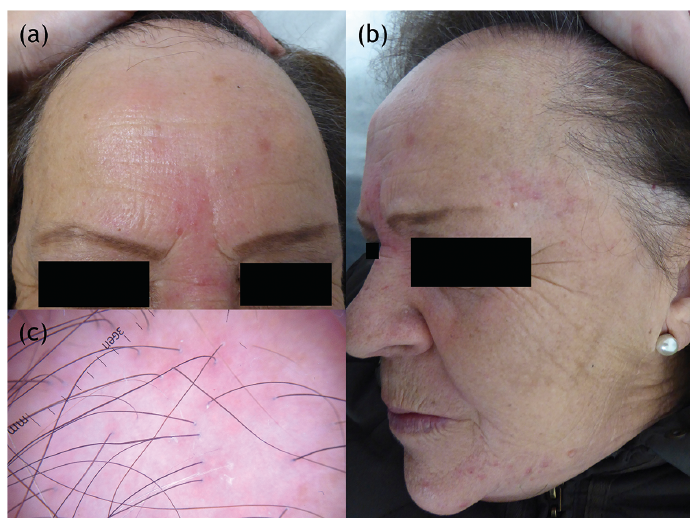 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize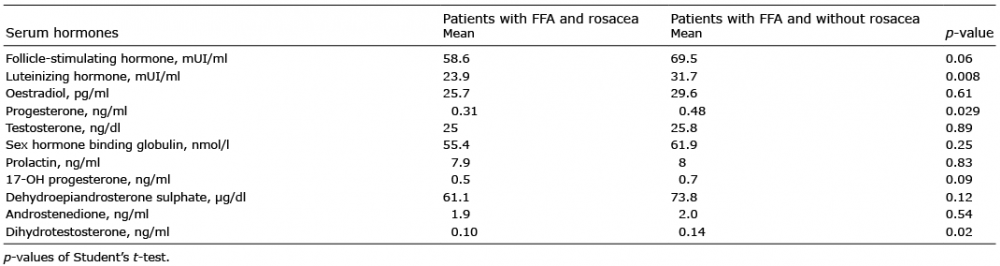 Click to show fullsize
Click to show fullsize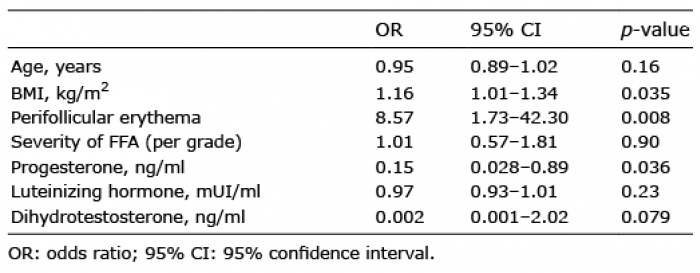 Click to show fullsize
Click to show fullsize