


1Department of ENT-Head and Neck Surgery and 5Department of Dermatology, University Cancer Institute Toulouse and Toulouse University Hospital, Hôpital Larrey, 2Department of Surgery and 3Department of Biostatistics, Institut Claudius Regaud, University Cancer Institute Toulouse – Oncopole, 4Department of Maxillofacial and Facial Plastic Surgery, University Cancer Institute Toulouse and Toulouse University Hospital, Hôpital Pierre-Paul Riquet, Toulouse, France
#These authors contributed equally to this manuscript.
Ten to fifty percent of high-risk cutaneous squamous cell carcinoma may potentially metastasize. However, the concept of sentinel lymph node biopsy remains controversial for cutaneous squamous cell carcinoma. The aim of this study was to identify prognostic factors associated with sentinel lymph node positivity. A bicentric retrospective analysis was conducted between January 2006 and January 2018. All patients undergoing sentinel lymph node biopsy for high-risk cutaneous squamous cell carcinoma were included, based on the criteria of the prognostic classification of the French Society of Dermatology. Seventy-four patients were included. Five (6.8%) procedures failed. Of the 69 patients assessed, the positive sentinel lymph node biopsy rate was 11.6% (n = 8) with a false negative rate of 5.7% (n = 4). The positivity of sentinel lymph node biopsy was associated with tumour size (p = 0.0194). Sentinel lymph node biopsy is an effective staging procedure for clinically N0 high-risk cutaneous squamous cell carcinoma, with an acceptable morbidity. To date, 2 risk factors of sentinel lymph node positivity have been identified with statistical significance: tumour size and poor tumour differentiation.
Key words: high-risk cutaneous squamous cell carcinoma; sentinel lymph node biopsy; risk factor; tumour size.
Accepted Aug 12, 2019; E-published Aug 13, 2019
Acta Derm Venereol 2019; XX: XX–XX.
Corr: Emilien Chabrillac, Department of ENT-Head and Neck Surgery, University Cancer Institute Toulouse and Toulouse University Hospital, Hôpital Larrey 24 Chemin de Pouvourville, FR-31400 Toulouse, France. E-mail: emilien.chabrillac@gmail.com
Among patients presenting a cutaneous squamous cell carcinoma, this study analyses the patient’s and tumour’s characteristics associated with metastasis in the first draining lymph node, called the “sentinel lymph node”. The results show that a large tumour size is a risk factor for lymph node metastasis.
Cutaneous squamous cell carcinoma (cSCC) is the second most common cancer in humans. Its incidence varies worldwide and is estimated at approximately 25/100,000 inhabitants in France (1). Indeed, the highest incidence is 499/100,000 for Australian men and 291/100,000 for Australian women (2). Seventy-five percent of cases develop on sun-exposed areas of the head and neck (3, 4). The lifetime risk ranges from 4% to 14% (3), and is currently increasing as the population ages (5).
Most cSCCs have a favourable prognosis and can be cured by a surgical excision when treated at an early stage. However, when a cSCC has some high-risk features, its potential to metastasize increases up to 10–50% (6, 7). Small metastases can be clinically and radiologically occult. cSCC mortality usually results from uncontrolled regional metastasis (8, 9), which should therefore be tracked. Distant metastases are rare and generally occur at a later stage of the disease, after regional nodal involvement.
Sentinel lymph node biopsy (SLNB) allows the identification and pathological analysis of the first tumour-draining lymph nodes. This concept was initially used in breast cancers and, more recently, in cutaneous melanoma and oral cavity squamous cell carcinomas. The value of the SLNB is well-established in these indications: this staging procedure ensures better sensitivity and specificity than the imaging work-up (10–12), lower morbidity than the prophylactic lymph node dissection (13, 14) and seems cost-effective (15).
However, SLNB is still not routinely recommended in the work-up of clinically N0 high-risk cSCC because of a lack of high-level evidence, not in terms of efficiency (16, 17) but in terms of patient screening. Although more data are being published on this topic, to our knowledge, the largest series reported included 83 patients with high-risk cSCC (18) and the procedure remains controversial.
This paper discusses the experience of 2 Toulouse-based teams in SLNB for cSCC. The aim of this study was to identify prognostic factors associated with SLN positivity.
This bicentric retrospective analysis was conducted between January 2006 and January 2018. We included all patients who underwent SLNB for a cN0 high-risk cSCC in the ENT, maxillo-facial or plastic surgery department of 2 French tertiary referral centres in Toulouse. As there is no clear-cut recommendation, the regional dermatology multidisciplinary tumour board indicated SLNB in both centres on a case-by-case basis, for cN0 cSCCs with an expected high potential to metastasize (usually with multiple high-risk criteria). Some lip cancers were discussed by other multidisciplinary tumour boards (otorhinolaryngology and maxillofacial). According to the prognostic classification of the French Society of Dermatology (19), one of these criteria staged tumours as “high-risk”: immunodeficiency, recurrent tumour, fixation to deep plane, size ≥ 20 mm (or ≥ 10 mm if the following were involved: nose, lip, eyelid, external ear, sun-protected sites, site of prior radiotherapy or chronic inflammatory process), neurological symptoms, thickness > 3 mm, Clark’s level ≥ IV, perineural invasion, aggressive histological subtypes (acantholytic, adenosquamous, metaplastic), moderately or poorly differentiated tumour. We chose this classification because it is consistent with the European approach and includes the entire National Comprehensive Cancer Network (NCCN) (20) risk factors apart from rapid tumour spread and the 2 mm-thickness threshold. The SLNB procedure was the same in both centres: injection at the tumour site or prior resection site of technetium-99m nanocolloid tracer the day before surgery (dose 19 MBq) or the morning of surgery (dose 9 MBq), then single photon emission computed tomography (SPECT) plus CT scan or SPECT-CT, and intraoperative use of a portable gamma-camera. The use of blue dye was optional. Vermilion SCCs were included if their origin was not behind the wet/dry line. Exclusion criteria were: patients with previous history of loco-regional radiotherapy or lateral neck surgery, anogenital SCCs. The following additional data were collected: patients’ characteristics (age, sex, relevant comorbidities including immunodeficiency), preoperative work-up, previous treatment (if applicable), tumour location and histopathological characteristics (level of differentiation, tumour size, T staging according to the 8th American Joint Committee on Cancer (AJCC) classification (21), tumour thickness, Clark’s level, tumour embolism, perineural invasion), intra- and post-operative assessments (method of detection, procedural failure and complications), sequelae, SLN histopathological analysis (including immunohistochemical staining for some cases), adjuvant therapy, recurrences and survival.
Statistical analysis
Qualitative variables were summarized as frequency and percentage, and quantitative variables as median with range (min–max). The comparisons between the positive (SN+) and negative (SN–) SLN groups were assessed using the χ2 test or Fisher’s exact test for qualitative variables and the Mann–Whitney test for quantitative variables. Tests were 2-sided and p-values < 0.05 were considered significant. Statistical analyses were performed using STATA version 13.1.
A total of 74 patients underwent the procedure and satisfied the inclusion criteria: 65 men and 9 women (male:female ratio 7.2:1). Median age at surgery was 72 years (range 39–92). Five procedures failed (6.8%). These 5 patients were excluded from further statistical analyses.
Among the 69 patients undergoing a successful procedure, 2 groups were compared: positive SLN (n = 8; 11.6%) or negative SLN (n = 61; 88.4%). The main characteristics of patients and tumours are shown in Table I. The features staging tumours as “high risk” according to the French Society of Dermatology (19) are shown in Table II.
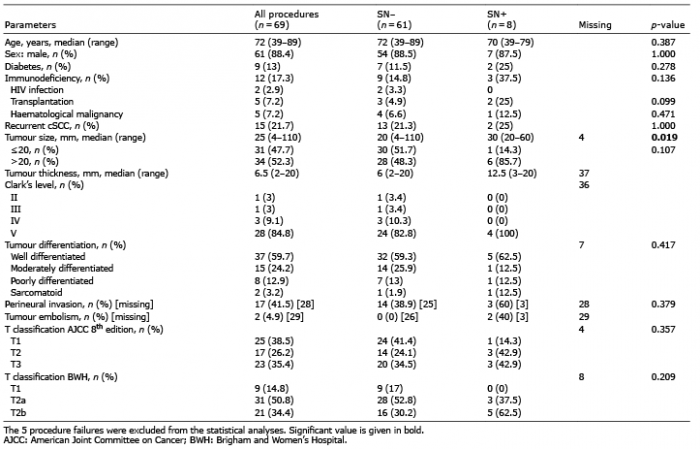
Table I. Main characteristics of patients and tumours
Table II. Features staging tumours as “high risk” according to the French Society of Dermatology (19)
Some patients had a medical history of cutaneous carcinoma (40.6%), diabetes (13%) or immunodeficiency (17.3%): HIV infection (2.9%), solid organ transplantation (7.2%) or haematological malignancy (7.2%). The strongest association with SLN positivity was transplantation (p = 0.099), but this was not statistically significant.
Preoperative workup always comprised at least one loco-regional imaging, according to the French Society of Dermatology recommendations. It could include ultrasonography (17.5% of patients), loco-regional computed tomography (CT) scan (80.7%), and systemic CT scan (36.8%). Three 18F- fluorodeoxyglucose-positron emission tomography (FDG-PET)/CT scans were performed to help determine the nature of a moderately suspicious lymph node. For 10.4% of patients, surgical management required 2 steps: tumour excision revealing unexpected aggressive histopathological features, followed by SLNB with a median interval of 4 weeks. Of the procedures, 10.4% were performed using both a radioisotope and blue dye. Early local complications occurred in 5.8% of patients: 2 surgical-site infections, 1 haematoma, and 1 transient facial nerve palsy. None of these patients required surgical treatment or developed permanent sequelae.
cSCC was recurrent in 21.7% of patients. The most common tumour site was the lip (34.8%), then the external ear (14.5%) and the peri-auricular area (10.1%). Most (92.8%) of cSCCs were located in the head and neck. Other cSCCs concerned sun-exposed areas of the whole body. The median size of the tumour was 25 mm: 20 mm in the SN– group and 30 mm in the SN+ group (missing data: 4 patients). There was a significant association between tumour size and SLN positivity (p = 0.0194). In the SN+ group, 85.7% of tumour sizes were > 20 mm, whereas in the SN– group, only 48.3% were > 20 mm. However, with a cut-off value of 20 mm, the association lost its statistical significance. Median tumour thickness was 6 mm in the SN– group and 12.5 mm in the SN+ group, but the difference was not statistically significant. There was no association between the histological subtypes or the level of differentiation and SLN positivity. Clark level V was always recorded in the SN+ group. The histopathological analyses reported tumour embolism and perineural invasion in 40% and 60% of SN+ patients, respectively. In the other group, no tumour embolism was found, but 37.8% of patients presented perineural invasion.
The median number of harvested lymph nodes was 2 (range 1–7), for a median of 3 detected lymph nodes (range 1–7). Half of the lymph node involvement indicated micrometastases (< 0.2 mm), including one case with 2 micrometastases in 2 different SLNs. The remainder were macrometastases. The size of metastatic lymph nodes ranged from 9 to 20 mm.
After a median follow-up of 23.9 months (95% CI 12.9–39.7), 7 (10.1%) patients died (6 in the SN– group and 1 in the SN+ group) and 4 (5.8%) patients had an uncontrolled disease or died due to the cSCC.
In the SN+ group (n = 8), 3 patients were immunosuppressed (1 liver transplantation, 1 kidney transplantation, 1 chronic lymphocytic leukaemia), 2 other patients had a genetic disorder promoting the onset of cutaneous carcinoma (1 Keratitis-ichthyosis-deafness syndrome and 1 Lynch syndrome), and the 3 last patients presented with tumour of the lip involving the vermilion. Adjuvant therapy was administered in all cases. Seven underwent radical lymph node dissection (6 neck dissections, 1 axillary dissection), and 2 received additional radiation therapy (dose 54 Gy). One patient received a single radiation dose of 70 Gy. Two nodal recurrences occurred (25%) despite adjuvant therapy (lymph node dissection for both patients and radiation therapy for 1 patient). No distant metastasis was observed.
Within the SN– group n = 61), 4 nodal recurrences were observed as the initial event, and were deemed as false-negative SLN procedures (rate = 5.7%). One of these 4 patients eventually presented distant metastatic spread and died.
To our knowledge, this is the second largest ever published series concerning SLNB and non-ano-genital high-risk cSCC. Its positivity rate of 11.6% (n = 8) is consistent with the latest literature reviews, reporting rates ranging from 8% (22) to 14.6% (17). The largest series by Wu et al. included 83 patients, but only 5 SLNB were positive (6%) (18). This is a substantial limit, considering that there were not enough SN+ patients in our series to perform a multivariable analysis and identify independent predictive variables. Only 1 systematic review (23) reported a SLN positivity predictor in cSCC, which was poor tumour differentiation. It was also associated with local and/or nodal recurrence in the SN– group. Using an alternative TNM system based on the number of risk factors (24), Schmitt et al. (25) found a significant link between positive SLN and T2a (1 risk factor) or T2b cases (2 or 3 risk factors).
The literature suggests the importance of tumour size, referring to a 2-cm diameter cut-off value (10, 26) associated with a 3-fold increase in power to metastasize (27). However, our case series is the first study showing a significant link between tumour size and SLN positivity (p = 0.019).
We know that cSCC mortality usually results from an uncontrolled regional clinical course (8, 9). Consequently, early detection of nodal disease is important and may improve the prognosis of the disease in some patients. However, the superiority of SLNB over active monitoring or prophylactic lymph node dissection remains controversial (28). On the one hand, there is no data to confirm that diagnosis of microscopic lymph node metastasis in cSCC leads to a better prognosis than later diagnosis (22, 23). On the other hand, a literature review of 260 procedures taken from 14 studies (17) revealed that patients with confirmed subclinical node metastasis still had a significantly higher mortality rate than SLNB-negative patients (p = 0.008), despite appropriate adjuvant therapy.
The risk cut-off threshold and indications still have to be decided: no academic society has proposed clear-cut guidelines for SLNB (19–21, 29, 30). This shortfall can be attributed to various issues. Firstly, the studies available are not sufficiently large to reliably identify predictors of SLN positivity or its impact on disease-free survival. Secondly, the criteria for recommending SLNB for cSCC vary considerably from one study to the next. Indeed, there are currently 4 main definitions of “high-risk” cSCC presented by the NCCN (20), AJCC (21), Brigham and Women’s Hospital (BWH) (31) and ours, by the French Society of Dermatology (19). Finally, the inclusion of vermilion cSCC is a recurrent bias, as the risk of nodal metastasis is 5 times greater compared with hair-bearing lip cSCC (32). Some authors suggest that we should encourage SLNB (or radiotherapy to nodal basin) for patients with BWH stage T3 cSCC and consider it for T2b patients (33–35).
The false-negative rate in our study (n = 4; 5.7%) is consistent with a recent literature review highlighting a rate of 4.6% (10). Only Wu et al. (18) reported a false-negative rate of 0%, after excluding patients with concurrent local recurrence. In each of our 4 false-negative cases, immunohistochemical staining was carried out. One case presented a negative SLN, but a positive non-sentinel lymph node harvested by the surgeon, as a reminder that bulk lymph node metastasis can alter radiotracer diffusion (36). These results are indicative of a failure in terms of the lymphoscintigraphic or surgical identification of SLN, an anatomical variation in patients or a role for the delay between initial tumour excision and the SLNB procedure by tissue fibrosis and reorganization of lymphatic drainage. Multiple cSCC can also lead to confusion in identifying which tumour caused the nodal spread. The concept of skip metastases remains highly controversial (37). Our patient cohort was too small to estimate procedure sensitivity and negative predictive value.
Another flaw in the SLNB procedure is its failure rate of 6.8% in our series, which is poorly described in oncodermatology literature. In the study by Wu et al. (18), the failure rate was 5.7%.
Our study confirms the low rate of complications already reported in previous studies (13, 14), including allergic reaction to the dye, surgical-site infection or haematoma, seroma, lymphoedema, wound dehiscence or vessel or nerve injury.
Limitations of this study are the lack of consensus for the definition of high-risk factors, the small patient cohort, missing data and some disparities in terms of approach, such as the delay between tumoural and nodal surgery, the recently increased access to immunohistochemistry and the optional use of blue dye. Regarding disease-free survival, there is a lack of perspective as late recurrences may still occur. An important bias of this study is the inclusion of vermilion tumours, which are more aggressive than strictly cutaneous SCC. Another issue is that the clinical significance of pN+ (i+) disease (positive SLN only after immunohistochemical staining) remains uncertain.
SLNB is a very effective staging procedure for clinically N0 non-ano-genital high-risk cSCC, with an acceptable morbidity. To date, 2 risk factors for SLN positivity have proved to be statistically significant: tumour size and poor tumour differentiation. Both can be identified preoperatively and indicate SLNB with tumour excision in a 1-stage surgical procedure.
A general consensus regarding the definition of high-risk factors, randomized controlled trials and larger series are expected to provide clearer insight into associated risk factors and confirm the benefits of this approach in terms of prognosis. This will eventually result in clear-cut indications and guidelines from academic societies.
The authors thank Gilles Poissonnet and Martin Penicaud for their scientific support, and the Research, Development and Innovation Directorate of Toulouse University Hospital for linguistic support.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize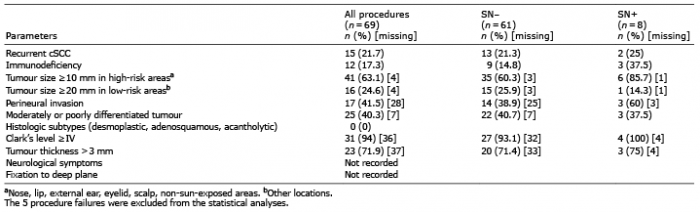 Click to show fullsize
Click to show fullsize