


1Dr. Phillip Frost Department of Dermatology and Itch Center, University of Miami, Miami, FL, USA, 2Department of Dermatology and French Expert Center on Itch, University of West Brittany, Brest, France, 3Department of Dermatology, University of Kiel, Kiel, 4Department of Dermatology and Allergy, Charité-Universitätsmedizin Berlin, Berlin, 5Department of Dermatology, Centre for Chronic Pruritus, University of Münster, Münster, and 6Department of Experimental Pain Research, University of Heidelberg, Mannheim, Germany
Barrier damage, dry skin and itch are intricately linked and form the basis of many common skin diseases. Damage from environmental insults, or genetic or inflammatory causes, can impair the skin barrier, resulting in an increase in transepidermal water loss and activation of itch-associated nerve fibres. The itch–scratch cycle can perpetuate skin barrier damage and itch. Topical therapeutic strategies are utilised to overcome dry skin and itch, primarily in the form of emollients. Recent advances in our understanding of the mechanisms underlying itch have enabled the development of new topical therapies, which may be incorporated into existing treatment regimes. Ultimately, treatment of dry skin and itch must be highly tailored to the individual according to their needs.
Key words: pruritus; dry skin; skin barrier; emollients.
Accepted Aug 22, 2019; E-published Aug 22, 2019
Acta Derm Venereol
Corr: Gil Yosipovitch MD, Dr. Phillip Frost Department of Dermatology, Miller School of Medicine University of Miami, 1600 NW 10th Ave RMSB 2067B Miami FL 33136, USA. E-mail: yosipog@gmail.com
Itch is a common symptom of many skin barrier-related dermatoses and can severely impact quality of life. However, there are a limited number of effective anti-itch topical therapies currently available and several unmet needs not addressed by current itch management strategies. As our knowledge of the mechanisms underlying itch has improved, several novel therapies have recently emerged that can be incorporated into existing regimens to enhance itch therapy and management. Here, we summarise research and current opinion on available topical therapies and give recommendations for the optimal management of itch.
Many chronic skin disorders, such as atopic dermatitis (AD) and psoriasis, are associated with impaired skin barrier function (1–3). The skin barrier prevents the entry of harmful agents, such as antigens and infectious microorganisms, and prevents moisture loss (2–4). Impaired barrier function has been linked to dry, itchy skin characterised by redness, flakes, cracks and a rough texture (“outside-in”), but epidermal inflammation can also weaken the barrier (“inside-out”) (5, 6).
Pruritus, an important feature of many dermatoses with impaired skin barrier function, is a sensation that drives the urge to scratch and can severely affect quality of life (QoL) and psychosocial wellbeing (7–9). Itch intensity has been associated with stress and negative life events, and can place a burden on patients’ day-to-day activities (10).
The underlying dermatoses associated with dry skin (xerosis) and itch can differ between patient populations (11, 12). Structural and physiological changes in the skin barrier occur with age and, when combined with comorbidities and polypharmacy, lead to an increased incidence of barrier abnormalities among the elderly (11, 12). Xerosis is the most common cause of skin barrier-related pruritus in this population and has been reported in 69% of elderly chronic itch patients (13, 14). However, in children and adults, one of the most common causes of pruritus is AD (15), a chronic inflammatory disorder in which patients experience itch with high intensity (16). Itch can place a heavy burden on QoL, with AD having a profoundly negative impact on those afflicted and their families (17).
Topical therapy is the backbone of treatment for skin barrier-related pruritus and includes emollients, corticosteroids, immunomodulators, capsaicin, local anaesthetics and antihistamines (18). As our knowledge of the mechanisms underlying the sensation of itch have improved, several novel antipruritic therapies have emerged. This review aims to summarise the advantages and disadvantages of current and emerging topical therapies to treat dry skin and itch and highlight considerations to be made when choosing an appropriate therapy. Finally, we will discuss unmet needs in itch therapy.
For this review article, a PubMed search was performed using various search terms, with studies selected based on their scientific rigor and the strength of their results. Selected studies were compared and summarised according to existing theories and mechanistic models, in addition to the experience of the authors, who are key opinion leaders in the fields of itch and skin barrier function. Conclusions were made on a qualitative, rather than quantitative, basis.
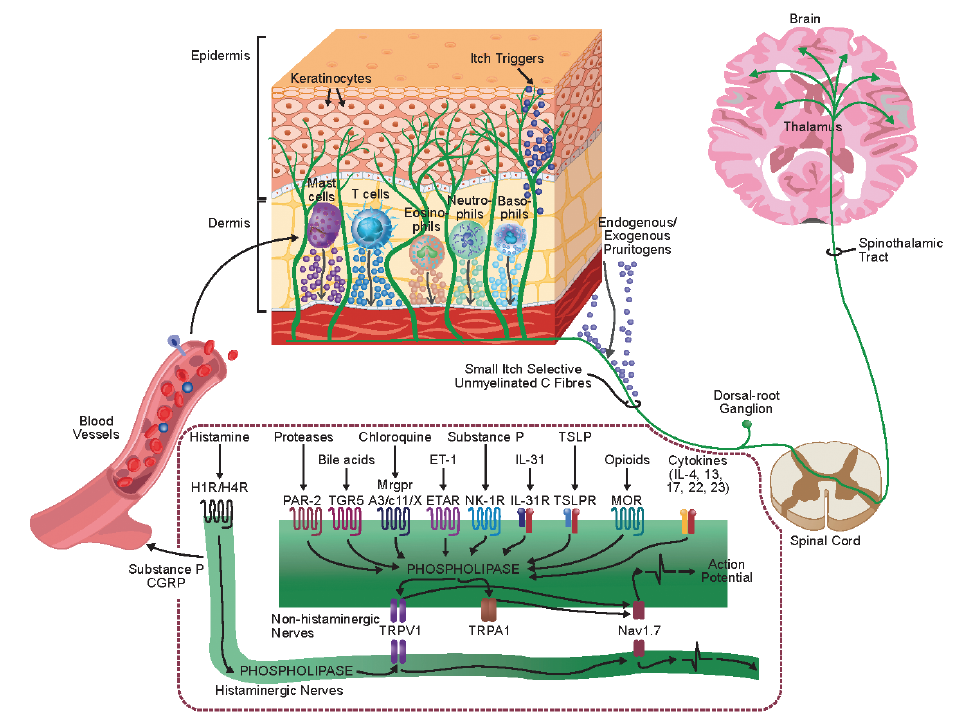
The sensation of itch can arise from the activation of epidermal nerve fibres that either belong to a specialised class of itch-provoking neurons (“pruriceptors”) or that are characterised by a highly focal spatial activation pattern (19). The chemical mediators that drive neuronal activity originate from complex interactions between keratinocytes, inflammatory cells and nerve endings, coupled with upregulated immune cascades, epidermal barrier function and potential penetration of Type I allergens into the skin (20, 21). Several factors including pH gradient, skin barrier integrity, irritant exposure and the microbiome modulate the impact of these interactions on neurons (2, 3, 9, 22).
In healthy skin, the corneocytes and lipid-rich matrix of the stratum corneum prevent the entry of potential pruritogens, such as infectious agents and allergens (23). Disruption of the skin barrier can be the result of a variety of factors, including epidermal inflammation and environmental insult (24); thus, both endogenous inflammatory mediators and penetrating exogenous mediators can activate itch-associated unmyelinated C fibres to induce the sensation of itch (25). Among the non-histaminergic receptors that mediate this interaction, protease-activated receptor (PAR)-2 and PAR-4 are the most prominent (25).
PARs are activated by endogenous and exogenous proteases on keratinocytes and sensory nerve endings (26). Activation of PARs can be linked to downstream activation of transient receptor potential (TRP) vanilloid 1 and ankyrin 1 (TRPV1 and TRPA1, respectively) (27); a large variety of inflammatory mediators also directly activate these TRP channels (28, 29).
Barrier dysfunction results in an increase in transepidermal water loss (TEWL) (16). In healthy skin, water is responsible for preserving the flexibility of the stratum corneum and is involved in the regulation of metabolic processes in the epidermal layer, such as desquamation (5). The skin of infants under the age of 2 years has a thinner epidermis and stratum corneum, smaller corneocytes, a higher water content and increased TEWL (30). In aged skin, barrier integrity is normal under basal conditions (31). TEWL, as a marker of barrier function, can even be reduced compared with younger adults, due to reduced blood flow (11, 32–35). However, the skin barrier in aging is sensitive to irritation that can occur as a result of extensive rubbing by clothes, washing with detergents, and hot, cold, dry or humid air, which may result in an impaired skin barrier (36). In the elderly, skin barrier function and reconstitution after damage is reduced because of thinning of the skin (11, 14). Reduced blood flow, reduced stratum corneum hydration and elevated skin pH, decreased enzyme activity, an altered cytokine profile and changes in the properties of epidermal stem cells contribute to impaired reconstitution (11, 37, 38).
Elevated TEWL is a marker of the disrupted skin barrier in inflammatory skin diseases. These diseases are also associated with a higher epidermal pH, which activates proteases to promote stratum corneum turnover and desquamation (3, 39–42). These proteases also lead to further activation of PAR-2 (26), creating a ‘vicious cycle’ of dry skin and itch.
Another self-perpetuating cycle is the itch–scratch cycle. Scratching mechanically disrupts the skin barrier, promotes inflammation and transiently activates inhibitory neurons at the spinal level to reduce itch sensation and prolong pruritus (25). Severe scratch-induced epidermal injury also injures sensory nerve endings that may be rendered hyperexcitable upon regeneration (25). Complications, such as secondary bacterial infections, may arise from scratching due to the introduction of pathogens from under the fingernails (12).
In addition to the non-histaminergic PAR-2-stimulated pathway, itch can also be induced via a histamine-dependent pathway (43). In an inflammatory environment, histamine is released from mast cells and activates a subset of mechanically insensitive C fibres that are different to those activated with the other pruritogens (44). Many Mas-related G protein-coupled receptors (MRGPR) are expressed on the surface of itch-associated sensory nerves and act as receptors for histamine-mediated itch (45). Interleukin (IL)-31, -4 and -13 are among the various cytokines and chemokines that may act as agonists for MRGPR. However, the extent of their individual roles in itch is debated (46). Itch is a complex modality with multiple components and pathways (Fig. 1), many of which have yet to be fully elucidated.
In AD, there is controversy as to whether the branching of epidermal nerve fibres is higher or lower compared to healthy individuals. Current data suggest that there is less epidermal innervation in those with AD or psoriasis compared to those with healthy skin (47). On the other hand, scratch-induced lesions can also include neuronal injury leading to hyperexcitability; however, they may also lead to reduced epidermal nerve fibre density (25, 48).
Fig. 1. Key peripheral mediators and neural circuitry involved in itch. Upon skin barrier damage or inflammation, skin cells and immune cells can release itch mediators that can activate pruriceptors on the nerve terminal of C fibres. Adapted from J Allergy Clin Immunol, 142(5), Yosipovitch G, Rosen JD, Hashimoto T. Itch: From mechanism to (novel) therapeutic approaches, 1375-1390, Copyright (2018), with permission from Elsevier.
As skin barrier damage can cause pruritus, topical therapies that target the keratinocytes, nerves and itch receptors in close proximity to the stratum corneum may provide significant relief for itch. Topical therapies include emollients, corticosteroids, immunomodulators, capsaicin, anaesthetics and antihistamines (9). Improved knowledge of the structure of the skin and underlying mechanisms of keratinocyte differentiation have enabled a more rational approach to therapy; some topical therapies aim to restore normal epidermal differentiation rather than occlude the surface to prevent TEWL (49). Depending on the origin of pruritus, topical treatments may also be combined with systemic therapies, such as gabapentin, as well as education and psychological strategies to help break the itch–scratch cycle (10, 50–52).
Treatment of itch must be tailored to the underlying cause/disease, itch severity, body site, lifestyle, climate and age (51). The risk to benefit ratio should be calculated if the intent is to treat large areas of the skin using a topically applied active agent. One must take into account that young children present particular challenges because of their increased surface area to volume ratio and therefore relatively increased absorption, slower metabolism than adults and more pronounced systemic effects (53).
A key consideration of topical therapies is pH. High skin pH results in the release of proteases and the activation of PARs, which mediate itch signalling (42, 54). In patients with AD, the skin surface is between 0.1 and 0.9 pH units higher than healthy control subjects, indicative of a reduced pH gradient across the stratum corneum.(55). Restoring pH to that of healthy skin (pH 4–6) is an important therapeutic consideration (3).
Adherence rates for topical therapies strongly influence favourable disease outcomes (56). Although many topical preparations have been shown to be effective in highly controlled clinical trials, their frequency of use by patients varies dramatically in practice. Unachievable routines and unpleasant smell and consistency are commonly cited reasons for poor adherence (51, 57).
Emollients
Emollients are emulsions consisting of water and lipids (water in oil [W/O] or oil in water [O/W]) that act to rehydrate the corneocytes by replenishing the content of the extracellular medium with water-binding compounds and lipids. This reduces TEWL (5, 10, 18) and the penetration of substances into the skin to repair the dysfunctional skin barrier (41). Emollients or barrier-improving creams are the first-line therapy for the treatment of all skin barrier-related itch (41, 58).
Emollients can contain supplementary ingredients with anti-itch properties to target multiple components of the itch pathway (5). In the skin, the endocannabinoid system plays a regulatory role in proliferation, differentiation and cytokine release (59). Incorporation of an endocannabinoid-targeting component within a cream, such as N-palmitoylethanolamine, can decrease the sensation of itch by increasing the lipid content in the barrier (18, 60, 61).
Some emollients may have anaesthetic properties. Polidocanol is the polyethylene glycol ether of lauryl alcohol and has been widely used in galenic formulations for more than 50 years (62, 63). However, despite the long usage of polidocanol, there have only been two double-blind, placebo-controlled clinical studies investigating its efficacy. Polidocanol was found to reduce cowhage-induced itching during a 30-min test period, but had no significant effect on histamine-induced itch (62). This may explain the clinical efficacy of polidocanol in AD, in which the PAR2-dependent pathway is thought to be involved in itch sensation, rather than the histamine pathway (62). In the second study, itch severity, skin moisture, lipid content and pH were assessed after two emollients containing lactic acid and refined almond oil with/without polidocanol were administered on the left versus right body sides (63). Both emollients reduced itching and restored skin barrier integrity after first application and for up to 14 days later (p < 0.0001). However, effects specifically related to polidocanol could not be determined. Polidocanol should be investigated further in a clinical setting (63).
Different emollients can be prepared in distinct galenic formulations, such as lotions, creams and ointments (51). Lotions contain more water than lipids; creams contain lipids, water and an emulsifier; and ointments are primarily lipid based (49, 51). The most appropriate formulation for the patient can depend on a variety of factors, including season, tolerability, cost, mechanism of action, fragrance, age, body area and gender (51, 57, 58). For example, emollients targeting the face aim to be non-comedogenic (64, 65). Despite their benefits, patients often find ointment application to be a messy process, which reduces compliance. Therefore, the suitability of the topical preparation for the specific requirements of the patient must be considered.
Topical corticosteroids
Mild AD can typically be managed using topical therapies such as emollients (52), with topical corticosteroids a mainstay of anti-inflammatory treatment (66) in those with moderately to severely inflamed skin. Topical corticosteroids involve the activation of glucocorticosteroid receptors that inhibit proinflammatory cytokine release by transcriptional repression (67), diminishing the inflammatory component of skin barrier-associated itch. However, in non-inflammatory itch, topical corticosteroid use provides limited to no benefit (9).
Topical corticosteroids are associated with adverse effects (53), especially in younger children. In the elderly, topical steroids should also be used with care as potent formulations can result in thinning of the skin, which is already a significant problem in this patient population (14).
Topical immunomodulators
Topical calcineurin inhibitors, such as pimecrolimus, have been shown to be effective at reducing pruritus within 48 h of application (68). Calcineurin inhibitors regulate T-cell activation, inhibit proinflammatory cytokines and help to restore the skin barrier (69, 70). Treatment with 1% pimecrolimus twice daily for 3 weeks reduced TEWL and restored regular lipid bilayers in the stratum corneum (69). They may also mediate their antipruritic effects by activating and desensitising TRPV1 (71).
Use of calcineurin inhibitors in paediatric patients for prolonged periods of time should be monitored carefully. Although the evidence available is insufficient to suggest causality, the Pediatric Advisory Committee for the Food and Drug Administration has retained a ‘black box’ warning for use in the United States, citing a potential risk of B cell leukaemia with the use of calcineurin inhibitors in paediatric patients (72, 73).
Crisaborole, a non-steroidal phosphodiesterase 4 (PDE4) inhibitor, has shown efficacy in the treatment of mild-to-moderate AD (74). PDE4 inhibitors reduce the production of proinflammatory cytokines by activated keratinocytes, resulting in decreased inflammatory cell recruitment (75). In a post-hoc analysis of two phase II studies comparing crisaborole ointment to a vehicle control, significantly more patients experienced an early improvement in their pruritus with crisaborole than the vehicle (74).
Topical capsaicin
Topical capsaicin is an alkaloid compound that activates TRPV1 on cutaneous sensory nerves, leading to calcium influx that triggers the release and subsequent depletion of pruritogenic neuropeptides, such as substance P (18), but also desensitizes and locally ablates the sensory endings, thus limiting the transmission over time via these nerve fibres (18, 76).
Application of a 0.05% capsaicin cream 4 times daily to patients with atopic dermatitis resulted in relief of pruritus in 40% (4/10) of treated patients, with two patients discontinuing treatment due to a transient burning sensation (77). Blockade of TRPV1 has been shown to accelerate skin barrier recovery and alleviate AD-like symptoms (78).
Capsaicin-containing creams should be applied 3–4 times a day. However, a recently developed 8% capsaicin patch only requires a single application (79). Local erythema at the site of application and a transient burning sensation are common adverse effects; to manage these side effects and increase adherence, a topical anaesthetic, such as lidocaine, should be simultaneously applied for the first few days of use (18).
Topical antihistamines
Antihistamines, which antagonise H1 receptors to block the activation of the histamine-stimulated pathway (80), are only recommended for use with urticaria (as a systemic treatment) and insect bite-related pruritus. There is a lack of evidence to support the use of antihistamines in AD and other barrier defect-related skin diseases, as most types of chronic itch are non-histaminergic (81, 82). Only doxepin has shown efficacy as a topical agent in reducing pruritus, but it can cause allergic contact dermatitis, and its use is cautioned in children and the elderly (18, 83, 84).
Optimal treatment of itch will address all of its components: barrier dysfunction, inflammation and neuronal hypersensitivity (41). Treatments for the management of dry skin-related pruritus should be selected based on age, sex and any underlying aetiology (Table I). If dry skin is caused by an underlying disease, this should be addressed first (85).
Table I. Common skin barrier-related diseases with pruritus as a prominent symptom and their pathogenesis
Treatment of elderly patients must be tailored to their specific needs and comorbidities and should appreciate any physical or cognitive limitations that may make the application of topical treatments and adherence difficult (86). The increased likelihood of polypharmacy in this age group (> 65 years) confers a greater risk of adverse reactions than for other age groups or may even be a cause of the pruritus itself (14, 86).
Sex must also be taken into account during treatment as there are sex-specific differences in the localisation, triggering and scratching behaviour, and in the underlying causes of dry skin (96). For example, women are more likely to report the localised itching as occurring in attacks and have more chronic scratch lesions (96). The changing levels of oestrogen and progesterone in post-menopausal women lead to changes in hydration and collagen content, which can lead to pruritic inflammatory vulvovaginal dermatoses (97).
Temporal and seasonal factors are implicated in itch onset. For example, itch sensation is usually increased at night due to higher skin temperature, heat under the blanket, circadian rhythms of neuropeptides and cytokines, and fewer distractive thoughts (98, 99). Seasonally, barrier damage is usually worse during winter, which is a consequence of the dry environment outdoors (100). This is exacerbated when people come to the warmer conditions indoors, resulting in increased blood flow and increased metabolic activity in the skin. However, factors relating to warmer weather have also been implicated in itch onset. Extensive sweating during summer may irritate the skin and the skin barrier, particularly in those with AD, which leads to increased itching (3). In addition, sweating may increase the skin pH which can also lead to itch. In the winter, an ointment preparation is preferred, whereas in the summer a cream preparation is more suitable, as an ointment may result in unpleasant plugging of the sweat ducts (51).
Different body sites may have specific therapy needs. Mapping itch therapy according to sweating, skin barrier disruption and severity of dry skin should be performed. On the arms, legs and trunk, a greasy ointment may be preferential, whereas a cream preparation is advised for the face (particularly the eyelid) where prolonged use of greasy formulations may lead to perioral dermatitis (101, 102). A cream preparation is also recommended for use in the body folds and genital regions.
For the scalp, a preparation that is not too greasy is preferred by patients to avoid an “oily” look of the hair, and which can easily be washed out by water and a shampoo (103).
Novel targets for topical treatments and ingredients
There are several compounds currently undergoing preclinical or clinical trials. Strontium salts have been shown to suppress sensory irritation (104). Topical strontium chloride significantly reduced the peak intensity and duration of cowhage-induced itch (105). Inclusion of strontium into acid preparations can reduce burning and stinging sensations associated with some topical preparations, such as lactic acid-containing emollients (106), and could be used to increase adherence (39).
TRP cation channel subfamily M member 8 (TRPM8) channels are located on the end of epidermal nerve fibres and Merkel cells (107). TRPM8 channels are cold-gated ion channels that inhibit both the histaminergic and non-histaminergic itch sensory pathways when activated (108). A novel TRPM8 cooling compound has been developed that, when incorporated into a lotion, significantly reduced pruritus as assessed by a global score and a verbal rating scale (109, 110). TRPM8 agonists are promising novel compounds, especially for patients who report that cooling reduces their itch, that could be added to existing topical therapies and therefore warrant further investigation.
A combined topical application of ketamine-amitriptyline-lidocaine has demonstrated antipruritic properties effective in the treatment of chronic itch (111, 112). Ketamine, a N-methyl-D-aspartate antagonist, has a role in the treatment of pain in subanaesthetic doses (113). However, the mechanism of action of this topical combination is unknown and likely acts peripherally through blockade of sodium channels (111).
Another example of rationally selected novel topical therapies for itch are topical tropomyosin receptor kinase A (TrkA) inhibitors. These act to inhibit the nerve growth factor (NGF) pathway and are currently in development (114). Increased signalling via the NGF-TrkA-TRPV1 pathway is considered to be a key mechanism of cutaneous itch, thus presenting a viable target for antipruritic treatments (114).
PAR-2, which is highly implicated in itch sensation, is a direct target for several novel anti-itch therapeutics currently under development. The pepducin, PZ-235 significantly reduced the PAR-2-mediated expression of the proinflammatory nuclear factor-κB, thymic stromal lymphopoietin, tumour necrosis factor-α and the differentiation marker K-10 in human keratinocytes by 94–98% (115).
Tapinarof 1% cream is a naturally derived small molecule that activates the aryl hydrocarbon receptor to inhibit specific proinflammatory mediators, including IL-17A, enhance skin barrier function and reduce itch (116). Efficacy has been demonstrated in mouse models and in vivo human skin studies of atopic eczema and psoriasis (116, 117).
Unmet needs in the management of itch
The pathophysiology of itch is complex, especially with regards to cutaneous disorders. The exact mechanisms of initial barrier damage remain unclear. However, the recent elucidation of some components of the itch pathway have led to the identification of several novel therapeutic targets.
Despite the importance of pH in effective skin barrier function, the pH of many topical preparations remains unknown (39). When both healthy individuals and those with AD were exposed to the alkaline agents 0.5% sodium lauryl sulphate and 0.15% NaOH, natural moisturising factor levels were significantly reduced in both groups (118). The use of acidic emollients has been investigated in several murine models, with acidic preparations even showing a preventative effect against AD (119). These findings may be translatable and could lead to the development of novel emollients.
The impact of pruritus on a patient’s QoL is not always appreciated by healthcare professionals; this educational gap should be addressed as a priority (120, 121). Patients should also be educated in correct application of topical therapy to increase adherence. For example, sufficient emollient should be applied such as to make the skin glisten, but heavier application may make the patient uncomfortable, and stain clothes or furniture (51). In addition to topical therapies, there is a need for stress reduction in the management of the itch–scratch cycle along with psychological and behavioural interventions, such as habit reversal and cognitive behavioural therapy (10, 50, 122).
The physiological mechanism of itch comprises a complex interaction between keratinocytes, the immune system and the nervous system. As our understanding of the role of the skin barrier in itch onset has improved, topical treatments can evolve to adopt a more targeted approach to itch management; the inclusion of specific antipruritic ingredients in emollient preparations, for example, could provide a tailored product that is suitable for itch management.
The nature of itch varies depending on body site, with different parts of the body (the face in particular) presenting their own unique requirements for itch management. Mapping itch therapy according to body zone can ensure that the most appropriate galenic formulation is selected to meet patients’ individual needs.
In recent years, there has been a shift towards patient empowerment and self-care in chronic dry skin conditions; consequently, availability of an effective over-the-counter itch treatment with proven benefit would be a valuable addition to the market. Although itch can place a heavy burden on patients’ QoL, this is not always appreciated by healthcare professionals; there is a need to address this educational gap.
Medical writing support, including assisting authors with the development of the outline and initial draft and incorporation of comments was provided by Jessica Gorrill, MSc, and editorial support, including fact checking, referencing, figure preparation, formatting, proofreading, and submission was provided by Rachael Cazaly, BSc, both of Core, London, supported by Bayer Consumer Health according to Good Publication Practice guidelines. The Sponsor was involved in the review of information provided in the manuscript. However, ultimate responsibility for opinions, conclusions and data interpretation lies with the authors.
GY has been a consultant and advisory board member for Bayer, Sanofi, Regeneron, Trevi Therapeutics, Menlo, Galderma, Novartis, Pfizer Eli Lilly Kiniksa, and AbbVie. He has been the Principal Investigator for Pfizer, Eli Lilly, Sun Pharma, Kiniksa and Menlo Therapeutics and Regeneron. LM has been a consultant, advisory board member or principal investigator for: Bayer, Beiersdorf, Bioderma, Clarins, Expanscience, Johnson & Johnson, Leo Pharma, Eli Lilly, Menlo Therapeutics, Nestlé Skin Health, Novartis, Pierre Fabre, Pfizer, La Roche-Posay, Sanofi, Solabia, Trevi Therapeutics, UCB and Uriage. MM has been a consultant and/or advisory board member for Bayer, Beiersdorf, Celgene, Menlo Therapeutics, Merz Pharma, Novartis, NeRRe, Pierre Fabre, Roche, Sanofi and Sienna Biopharmaceuticals. EP has taken part in an expert panel organised by Bayer Consumer Health. SS has taken part in advisory boards organised by Sienna Therapeutics, Bayer, Celgene and Menlo Therapeutics, received research funding from Menlo Therapeutics, Dermasence, Trevi Therapeutics, Galderma, Novartis and Kiniksa, and received consulting fees from Beiersdorf, Celgene, NeRRe Therapeutics, Sienna Therapeutics, ACO HUD Nordic, Cemka, Trevi Therapeutics and Menlo Therapeutics. MS has taken part in an expert panel organised by Bayer Consumer Health.


 Click to show fullsize
Click to show fullsize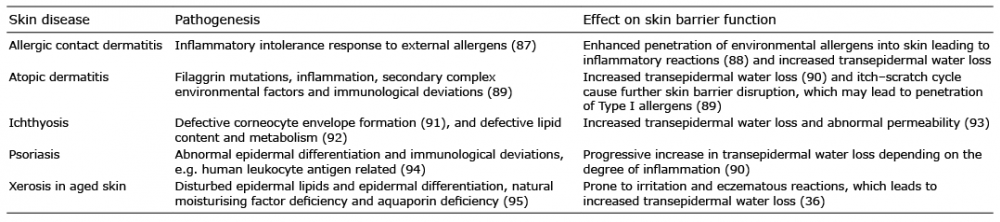 Click to show fullsize
Click to show fullsize