


1Department of Dermatology, Teikyo University School of Medicine, 2-11-1 Kaga, Itabashi-ku, Tokyo, 173-8605, and 2Teikyo Academic Research Center, Teikyo University, Tokyo, Japan. *E-mail: mkamata-tky@umin.ac.jp
Accepted Aug 22, 2019; E-published Aug 22, 2019
Rhododendrol (RD) inhibits melanin synthesis, and has been used in skin-whitening cosmetic products. How-ever, some individuals have developed leukoderma on the skin at the site of RD application and refractory depigmentation has occurred even after ceasing application of RD (1–4). Skin-whitening cosmetic products containing RD were discontinued in 2013. Bimatoprost is a prostaglandin F2α analogue, which is often used to promote eyelash growth (5) for cosmetic reasons and in the treatment of glaucoma (6, 7). Following reports that bimatoprost induces skin pigmentation as an adverse effect (8–12), we previously conducted an open-label single-centre pilot study to evaluate the effectiveness of bimatoprost on refractory RD-induced leukoderma (13). Following the previous study, in which patients applied bimatoprost for 6 months, one patient requested to continue application of bimatoprost. Five months after discontinuation of bimatoprost at the end of the pilot study, she re-started topical application of bimatoprost and continued for 14 months. We report here a case of refractory RD-induced leukoderma treated with bimatoprost for approximately 1.5 years in total.
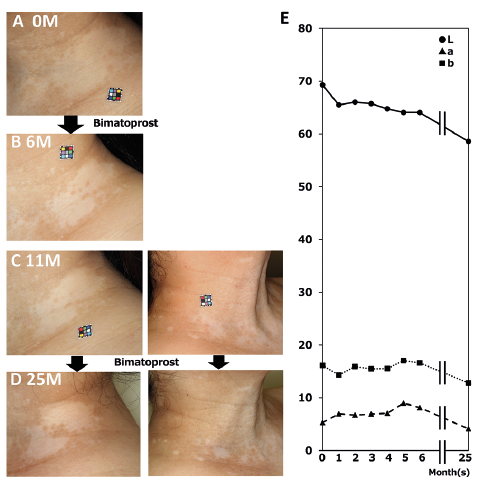
A 40-year-old Japanese woman started using cosmetics containing RD in April 2011. She developed leukoderma on her face and neck in April 2013 where she had applied RD. Thereafter, she discontinued the cosmetics containing RD in August 2013. Although the leukoderma on her face gained repigmentation without any further treatment after discontinuation of RD, the leukoderma on her neck had not improved for more than 3 years. The patient was enrolled in the previous pilot study to evaluate the effectiveness of bimatoprost on refractory RD-induced leukoderma in November 2016 at the age of 45 years (patient number RD-07), and applied bimatoprost on leukoderma on the left side of the neck once daily for 3 months, and then twice daily for another 3 months. The method is described in detail in the previous paper (13). The area of leukoderma on her neck, which was treated with bimatoprost, reduced in size significantly (Fig. 1A, B), and the patient requested to continue applying bimatoprost after the end of the study. After receiving another approval from Teikyo University Institutional Review Board, 5 months after discontinuation of application of bimatoprost in the study, she re-started to apply bimatoprost on leukoderma on both the right and left side of her neck and continued application of bimatoprost for 14 months (Fig. 1C, D). The areas of leukoderma reduced in size further after application of bimatoprost.
The colour of the skin was evaluated objectively using a colour-difference meter, “CM-2600d” (Konica Minolta, Inc., Tokyo, Japan). L* represents lightness, with the darkest black at 0 and the brightest white at 100. The a* axis represents red/green opponent colours, with green at negative a* values and red at positive a* values. The b* axis represents yellow/blue opponent colours, with blue at negative b* values and yellow at positive b* values. The colour-difference meter showed that the L* value slightly decreased after application of bimatoprost, especially on the left side of the neck, indicating that the skin became darker (Fig. 1E). The patient did not report any pruritus. Erythema as an adverse event was not observed. No other adverse events were observed.
Fig. 1. Case report. (A) Rhododendrol (RD)-induced leukoderma before topical application of bimatoprost to the neck. (B) RD-induced leukoderma on the neck 6 months after starting application of bimatoprost in the pilot study. (C) RD-induced leukoderma 5 months after discontinuation of topical application of bimatoprost and before re-starting to apply bimatoprost. (D) RD-induced leukoderma 14 months after re-starting to apply bimatoprost. mo: month; mos: months. (E) Changes in the results of the colour-difference meter on leukoderma on the left side of the neck. Time 0: time at which bimatoprost application was started in the pilot study in this patient. Circle: L* value; triangle: a* value; square: b* value.
In the previous study, bimatoprost was applied on RD-induced refractory leukoderma in 11 patients for only 6 months. The patient we report here extended the period of bimatoprost application up to 14 months, indicating long-term effectiveness and safety of bimatoprost application. Bimatoprost improved RD-induced leukoderma in our patient. However, it is difficult to draw a conclusion about the effectiveness of bimatoprost on RD-induced leukoderma based on a single case. As described previously (13), the area of skin affected was not measured, since the shape of the leukoderma was complex and it was on the neck of our patient. The surface of the leukoderma was uneven and difficult to measure. Furthermore, the results of a colour-difference meter do not reflect the reduction in size of the leukoderma. These factors make objective evaluation incomplete. Although bimatoprost appeared to be effective in our patient, the results of this single case report cannot be taken to imply that it is effective for all patients. Further studies are required to elucidate susceptibility to RD-induced leukoderma and pigmentation caused by bimatoprost. Moreover, we cannot rule out the possibility that the RD-induced leukoderma gained repigmentation spontaneously regardless of bimatoprost application.
Several papers have reported that RD exerts melanocyte toxicity in a tyrosinase-dependent manner, which leads to a reduction in production of melanin (2, 14–17). Other studies indicate that latanoprost, another prostaglandin F2α analogue, stimulates melanogenesis in iridial melanocytes, and transcription of the tyrosinase gene is upregulated (18). Considering these reports together, bimatoprost may increase or recover the expression of tyrosinase damaged by RD, resulting in repigmentation.
The case reported here suggests that bimatoprost may have the potential to improve refractory RD-induced leukoderma. In this case report it showed tolerable safety over a long period of use.
This study was supported by a grant from Kanebo Cosmetics Inc.


 Click to show fullsize
Click to show fullsize