


1Department of Dermatology and Allergy, Copenhagen University Hospital Herlev-Gentofte, DK-2830 Hellerup, 2Department of Pathology, and 3Department of Plastic Surgery, Copenhagen University Hospital Herlev-Gentofte, Herlev, Denmark. E-mail: stine.simonsen.01@regionh.dk
A 28-year-old woman presented with a painless tumour on her upper lip (Fig. 1). She had no medical history and used no medications. The tumour had been present since early childhood and had so far been considered benign. Over the last 5 years the tumour had grown slowly, and therefore the patient was referred for dermatological evaluation. On examination, the tumour was 1.5 cm in diameter, well-defined, circular, with marked induration, and non-adherent to the surroundings. The skin cove€ring the tumour was unremarkable apart from mild redness and minor telangiectasia at the periphery. The patient was otherwise asymptomatic and had no palpable lymph nodes.
What is your diagnosis? See next page for answer.
Fig. 1. Clinical presentation. Arrow indicates tumour location. The central papule represents a cicatrice after the first biopsy.
Acta Derm Venereol 2020; 100: XX–XX.
Diagnosis: Microcystic adnexal carcinoma
Two 3-mm punch biopsies were performed. The biopsies showed a diffusely infiltrative dermal tumour composed of narrow basaloid epithelial strands with focal duct formation in the upper dermis. There was slight cellular atypia. Immunohistochemistry showed positive staining for CK5, CK15, CK19, p40, and CD10, as well as weakly positive staining for CK7 and EMA luminally in the duct-like structures. Staining for Ep4, androgen receptor, CK20, Sox10, MelanA, and S-100 were negative. Consequently, a diagnosis of microcystic adnexal carcinoma (MAC) was suspected, along with desmoplastic trichoepithelioma and syringoma. A deeper knife biopsy was performed to assess the border of the tumour and the peripheral pattern of growth. The punch biopsy specimens were compared with the knife biopsy specimen, which showed the same morphology and immunohistochemical staining pattern. Furthermore, muscular invasion and possible perineural invasion (Fig. 2) was found in the deeper biopsy. Therefore, desmoplastic trichoepithelioma and syringoma were excluded and the diagnosis of MAC was confirmed.
Fig. 2. (A) The dermis is expanded by tumour tissue (haematoxylin and eosin (H&E) ×2.5). (B) A tumour islet (arrow) located immediately next to a small nerve fibre (stars) (H&E ×20).
A preoperative positron-emission tomography – computed tomography (PET-CT) scan revealed multiple metabolically active lymph nodes on the neck, including one enlarged lymph node. Ultrasound guided biopsy of the enlarged lymph node showed no metastasis. The MAC tumour was excised with a 3-mm clinical margin, leaving part of the orbicularis muscle intact, and 2 sentinel lymph nodes were removed, both without metastases. Additional muscle tissue had to be excised from 2 small areas because the primary deep margin was only partially clear. Following granulation, the defect was reconstructed with a full thickness skin graft.
MAC is a malignant adnexal tumour, probably deriving from a pluripotent adnexal keratinocyte. MAC is a rare condition with a reported incidence of 1.6–6.5 per 10,000,000 individuals (1). It occurs at all ages, but the reported mean age of incidence ranges between 44 and 64 years (2, 3). Predisposing factors may exist (2, 4, 5).
MAC has a predilection for the head and neck. Upon diagnosis, it has often been present for years. The lesion may be yellowish or skin-coloured, possibly with overlying telangiectasia. Typically, the surface is inconspicuous. The tumour is indurated, but asymptomatic. In some cases, pain, burning, paraesthesia, and anaesthesia have been reported (6, 7).
MAC is an indolent tumour with slow growth. None-theless, it is locally aggressive and early on invades local structures and deep tissue (8, 9). Only rare reports of lymph node metastases exist (2, 6, 10, 11). There is a significant risk of recurrence, possibly due to a high propensity for perineural invasion. In fact, local recurrence has been reported 30 years after primary treatment (12).
Importantly, the diagnosis may be challenging. Indeed, initial histopathological misdiagnosis was reported to range from 27% to 69% of cases (7, 13). This may be due to similar histopathological findings in MAC and other locally aggressive adnexal tumours, especially syringoma, desmoplastic trichoepithelioma, or infiltrative basal cell carcinoma (7, 13). Moreover, unique immunohistochemical markers to distinguish MAC from its differential diagnoses have not been identified and, as in the current case, a deep biopsy is valuable in identifying perineural or muscular infiltration (7, 13).
Characteristically, MAC extends far beyond the clinical margin. Hence, local recurrence has been reported to occur in 40–60% of patients after standard wide excision (13). Consequently, histological verification of clear margins is imperative and Mohs micrographic surgery has been proposed as the optimal treatment. Radiation therapy remains controversial (7).
In summary, the present case emphasizes the difficulty of correctly diagnosing MAC on superficial sections. Without an appropriately deep biopsy, MAC can progress unnoticed, delaying diagnosis and impeding proper treatment. Furthermore, the need to confirm free margins upon surgery, as well as long-term follow-up, must be emphasized.


 Click to show fullsize
Click to show fullsize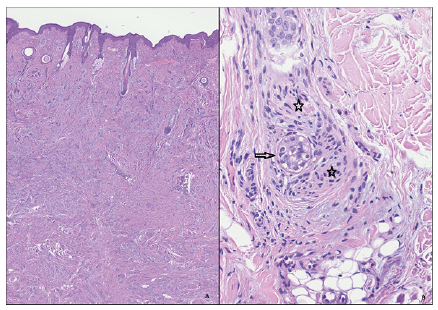 Click to show fullsize
Click to show fullsize