


Departments of Dermatology: 1Bordeaux University Hospital, Bordeaux University, Bordeaux, 2General Hospital, Périgueux, 3General Hospital, Bayonne, and 4Henri-Mondor Hospital, AP-HP, Paris-Est University Créteil (UPEC), Créteil, France
#Contributed equally as last senior author.
Gram-negative toe-web infection can cause pain and disability, be complicated by a long healing time, management failure, and cellulitis, and recur due to persistent predisposing factors. To describe the clinical features and management of Gram-negative toe-web infection and evaluate predisposing factors and associated diseases, their management, and the effect of controlling them on the rate of recurrence, we conducted a retrospective real-life study of patients with Gram-negative toe-web infection. Among the 62 patients (sex ratio 9:1), 31 experienced more than one episode of Gram-negative toe-web infection. Pseudomonas aeruginosa was the most prominent bacteria. Predisposing factors/associated diseases were eczema (66%), suspected Tinea pedis (58%), humidity (42%), hyperhidrosis (16%), psoriasis (11%), and vascular disorders (40%). Patients in whom associated diseases, such as eczema or psoriasis, were controlled did not relapse, suggesting the benefit of management of such conditions. We suggest that management of Gram-negative toe-web infection be standardised, with a focus on diagnosis and treatment of associated diseases.
Key words: Gram-negative toe-web infection; Pseudomonas aeruginosa; eczema; contact dermatitis.
Accepted Sep 10, 2019; E-published Sep 10, 2019
Acta Derm Venereol
Corr: Marie Beylot-Barry, MD, PhD, Department of Dermatology, Saint-André Hospital, Bordeaux University Hospital, 1 rue Jean Burguet, FR-33075 Bordeaux Cedex, France. E-mail: Marie.beylot-barry@chu-
bordeaux.fr
Gram-negative toe-web infection is a disabling painful disease with long healing time and high recurrence rate. In a French retrospective real-life study, we described features and management of Gram-negative toe-web infection and evaluated the effect of controlling predisposing factors/diseases on the rate of recurrence. Among the 62 patients included, mainly male, 31 experienced more than one episode. Pseudomonas aeruginosa was the prominent bacteria. Predisposing factors/associated diseases were eczema, suspected Tinea pedis, humidity, hyperhidrosis, psoriasis and vascular disorders. Patients in whom associated diseases were controlled did not relapse. Subsequently, an algorithm of Gram-negative toe-web infection management is proposed with a focus on associated diseases.
Gram-negative toe-web infection (GNTWI) is characterised by marked denudation of the toe-web spaces, extending along the plantar surface with a well-delimited hyperkeratotic macerated rim and a purulent, sometimes greenish and malodorous exudate (1–5). Pseudomonas aeruginosa is the most commonly identified of the various causative microorganisms (Proteus sp., Escherichia coli, Morganella morganii, Enterobacter sp., and Enterococcus faecalis) (2–4). The predisposing factors can be local or regional; i.e. interdigital tinea; occlusion; humidity; history of inappropriate treatment with antifungals, antibiotics, and topical corticosteroids; and contact/atopic eczema (2–5).
The long healing time and high recurrence rate of GNTWI make treatment challenging (2, 3, 5). Two small case series and a prospective study of 123 cases discussed the use of systemic antibiotics in severe and refractory GNTWI (2–4). However, the efficacy of systemic antibiotics has not been assessed, nor has the risk of development of antibiotic-resistant strains. In this retrospective multicentre study, we evaluated the clinical features, predisposing factors, and associated diseases of GNTWI, with the aim of proposing a standardised management algorithm.
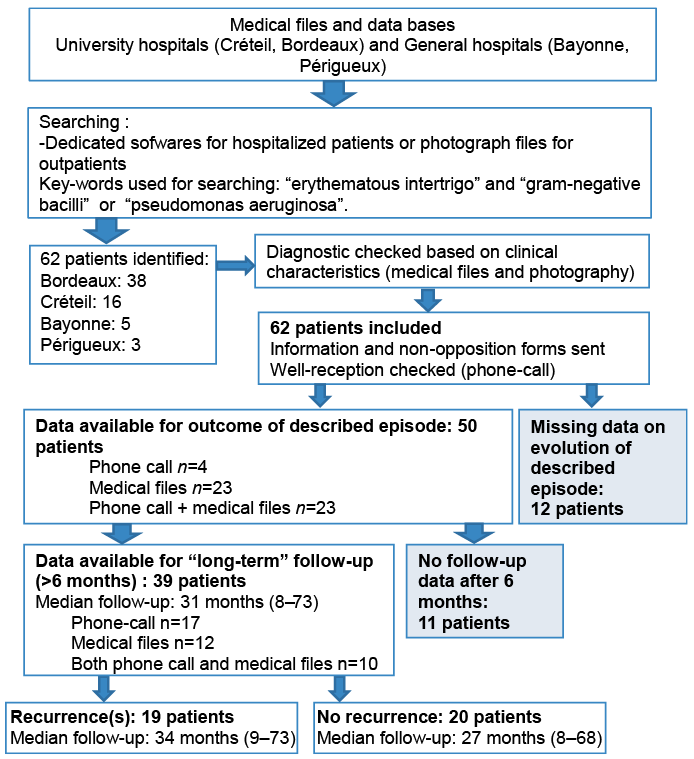
This real-life retrospective study was undergone in two university hospitals (Créteil and Bordeaux, and two general hospitals (Bayonne and Périgueux), all in France) from January 2011 to December 2017 (Fig. 1). The design was non-interventional and declared to the French national data-privacy agency (GP-CE 2018/21) in accordance with data-protection regulations. Information and non-opposition notes with our contact details were sent to the patients, all of whom were telephoned in July 2018 to verify receipt of the note.
Case identification was based on the medical information system and dedicated software for inpatients and a photograph database for outpatients, with the key words “erythematous intertrigo” and “Pseudomonas aeruginosa” or “gram-negative bacilli.” We checked the medical records for the diagnosis of GNTWI based on clinical evidence (photographs and clinical description) and bacteriological swabs, or on clinical symptoms (2, 5).
A standardised questionnaire was completed by one of the investigators (AG) for each patient. The data collected were as follows: age, sex, employment category, hobbies, atopic background, diabetes, immunosuppression, body mass index (BMI), hygiene, social issues, use of safety shoes or rubber boots, number of previous episodes and hospitalisations, symptoms, infectious complications, predisposing factors and/or diseases, duration of intertrigo before referral to a hospital, hospitalisation or ambulatory management, bacteriologic and mycologic swabs, biopsy, blood tests, patch tests, local and general treatment of intertrigo and associated diseases, outcomes, control of associated diseases, and recurrence.
We assessed outcomes from the first clinical episode to the most recent point in time for which adequate data were available. We gathered follow-up data for ≥ 6 months to evaluate recurrence.
Statistical analysis was performed on proportions and means. The association between control of associated diseases and the recurrence rate was analysed by Fisher’s test.
Fig. 1. Flowchart of the study.
Study population
The study involved 62 patients, 56 of whom were male (90.3%); the median age was 52.5 years (range: 10 to 94 years). Half of the patients (n = 31) had a BMI of > 25 (median, 30; range: 26 to 56.3). Diabetes and immunosuppression were rare (8%, n = 5 and 11.3%, n = 7) (Table I).
Concerning social factors, 19.4% (n = 12) of the patients had poor hygiene and 9.7% (n = 6) were homeless or lived in an insalubrious place. Of the patients, 29% (n = 18) had a physical job that required prolonged standing.
Table I. Demographic and clinical parameters of the study population (n = 62)
Clinical characteristics of Gram-negative toe-web infection
Of the patients, 39% (n = 24) had GNTWI for > 3 months. Pain was the most frequent symptom (89%; n = 55), followed by disability (85.5%; n = 53) and pruritus (63%; n = 39). Intertrigo was bilateral in 66% (n = 41) of the patients and several interdigital spaces were affected in 98.5% (n = 61) (Table II). Erosion, erythema, maceration, and abundant exudate were the most common features (Fig. 2) including a large proportion of patients with extension of the lesions to the foot, beyond intertrigo in association with a hyperkeratotic rim. Concomitant cellulitis was noted in 15 patients and impetiginisation in 3. One patient had concomitant otitis, and another had concomitant chondritis due to P. aeruginosa. Five patients had a fever of > 38.5°C at the time of management.
Table II. Clinical characteristics and outcomes of intertrigo (n = 62)
Fig. 2. Clinical features of the patients. (a) Limited hyperkeratotic rim of several interspaces, (b) plantar extension, (c) dorsal extension, (d) macerated rim, (e) greenish exudate, (f) purulent exudate, (g) erosive feature, and (h) associated eczema.
Associated local and regional findings
Of the patients, 80.6% (n = 50) had more than one local/regional risk factor for GNTWI (median, 2; range: 1 to 4) (Table III). Hyperhidrosis was found in 16% of the patients (n = 10) and 42% (n = 26) experienced humidity or occlusion or both: 16% (n = 10) for professional reasons (use of safety shoes), in 21% (n = 13) in association with sports and hobbies (fishing in rubber boots, use of a swimming pool, and hiking), and in the remaining patients for religious reasons (ablutions). Tinea pedis was clinically suspected in 58% (n = 36) of the patients, but only 5 of 50 mycological swabs during the acute phase, and 1 of 4 during the healing phase, yielded positive results. Eczema was found in 66% (n = 41) of the patients. Dyshidrosis was frequent prior to (n = 25) and concurrently with (n = 16) GNTWI, and 11% (n = 7) of the patients had palmoplantar psoriasis prior to (n = 3) or concomitantly with (n = 4) GNTWI; this was confirmed by cutaneous biopsy in two patients. One patient had histologically confirmed erosive lichen of the feet concomitantly with GNTWI. Regional anomalies (lymphoedema, venous insufficiency, neuropathy, and/or lower-limb arteriopathy) were observed in 40.3% of the patients (n = 25).
Table III. Associated local and regional findings and dermatoses
Management of the current episode
Paraclinical investigations. Bacterial culture of swabs was performed in 93.5% of the patients (n = 58). P. aeruginosa was the predominant pathogen (84.5%, n = 49), followed by Staphylococcus aureus (39.7%, n = 23). Only P. aeruginosa was isolated from 6 of the patients (10%); the other patients had polymicrobial infections. Notably all cases where Gram positive bacteria were isolated were found to be polymicrobial and Gram-negatives were always present. Five of the 50 mycological swabs yielded positive results: Candida parapsilosis (n = 2), Trichophyton rubrum (n = 2), and Trichophyton interdigitale (n = 1). Thirty patients had received antifungal treatment in the last 15 days. One of the 4 mycological swabs taken during the healing phase was positive for T. rubrum.
Patch tests were planned in 18 patients (21%) but were only performed in 13. The results of all of the 13 patch tests were positive, of which 11 were considered relevant (17.7%): sensitisation to topical products in 6 patients, to shoes in 2 patients, and to both shoes and topical products in 3 patients (Table SI)
Therapeutic management (Table SII). Of the patients, 75.8% (n = 47) required hospitalisation, in most cases (n = 29) after failure of the initial outpatient treatment. The median duration of hospitalisation was 11 days (range: 3 to 33 days) and the median number of consultations for monitoring of the current episode of GNTWI was 2 (range: 0 to 10).
In total, 74% of the patients (n = 46) had undergone one or more of the following treatments before their first visit to a hospital: systemic antibiotics (40.3%; median, 2 [range: 1 to 4]), local antifungals (51.6%), antiseptics (29%), and local antibiotics (17.7%).
In the overall patient population, 54.8% (n = 34) of the patients received only topical treatment and 45.2% (n = 28) received systemic antibiotics and topical treatment. Topical treatments were comprised of antiseptics (82.3%, mainly hydrogen peroxide and boric acid), topical antibiotics (43.5%; typically silver sulfadiazine or gentamycin), or topical steroids (58%).
Of the patients, 25.8% (n = 16) received topical antifungals and 6.5% (n = 4) systemic antifungals. Ten of the patients underwent mechanical debridement. Systemic antibiotics were directed against P. aeruginosa in 16 of the patients (most frequently piperacillin–tazobactam without or with ciprofloxacin) and against S. aureus or β-haemolytic streptococci in 12. Two patients received systemic antibiotics for urinary infection and one for P. aeruginosa chondritis.
Cellulitis
Among the 15 patients with cellulitis, 11 had vascular disorders: venous insufficiency or lymphoedema (n = 6), lower-limb arteriopathy (n = 2), or both (n = 3). The antibiotics prescribed to these patients were directed against S. aureus and β-haemolytic streptococci (n = 7 and n = 10, respectively).
Management of associated diseases
Eczema was treated most frequently using topical steroids, and with methotrexate and alitretinoin in one patient each. Six patients did not receive any treatment for eczema. Psoriasis was treated by topical steroids alone (n = 2), acitretin (n = 3), or methotrexate (n = 1), or was untreated (n = 1). In 15 patients, clinically suspected Tinea pedis was treated by systemic and topical antifungals, in 2 patients by systemic antifungals alone, and in 12 patients by topicals antifungals alone. Iontophoresis was prescribed to one patient with hyperhidrosis. Six patients received venous contention for venous insufficiency. Data on the control of associated diseases were available for 50 patients; the associated disease was controlled in 14 of the 50 patients.
Outcome
Among the 50 patients with available outcome data, 22 had complete healing and 13 did not experience recurrence of GNTWI. Conversely, 28 patients did not achieve complete healing, as evidenced by abnormal interdigital spaces with persistent erythema, desquamation, or erosion. Of these 28 patients, 11 and 7 did and did not experience recurrence of GNTWI; follow-up data for the remaining 10 patients were missing. Long-term follow-up (> 6 months; median, 31 months; range: 8 to 73 months) data were available for 39 patients, of whom 19 experienced recurrence of GNTWI. In total, 50% (n = 31) of the patients had more than one episode of GNTWI and 23% (n = 14) had more than 5 episodes. Among the 32 patients with GNTWI caused by their profession, 18 (75%) and 2 (8.34%) had to leave and modify their job, respectively.
Control of associated diseases and recurrence of Gram-negative toe-web infection
Among the 39 patients with available long-term follow-up data, the 19 who experienced recurrence of GNTWI had an uncontrolled associated disease. Of the 20 patients who did not experience recurrence of GNTWI, 13 and 7 had controlled and uncontrolled associated diseases, respectively. Control of associated factors was significantly associated with absence of recurrence (p < 0.0001). Among the 13 patients in whom associated diseases were controlled, 4 had tinea pedis treated by antifungals, 5 had dyshidrosis or atopic dermatitis (treated by topical steroids in 4 cases and by methotrexate in 1 case), 3 had psoriasis treated by topical steroids (in 2 cases by acitretin), and 1 had an erosive lichen treated by topical steroids.
Among the 19 patients with recurrence of GNTWI, the associated factors were eczema flare (n = 8), psoriasis flare (n = 3), and wearing occlusive footwear (n = 2).
The patients with GNTWI were predominantly male and exhibited clinical features characteristic of this painful and disabling acute intertrigo (1–7). GNTWI was frequently recalcitrant to previous treatments, primarily topical antifungals. P. aeruginosa was the predominant causative agent, most frequently in association with other microorganisms (2–4, 8). Most mycological cultures were negative despite the role of dermatophytes in the development of GNTWI (9, 10).
Systemic symptoms and cellulitis were not frequently associated with GNTWI. Furthermore, diabetes and immunosuppression were infrequent in our patients managed in dermatology wards.
Half of the patients experienced more than one episode of GNTWI, similar to the rates of 7% and 53% of 123 and 17 patients in two prior reports (2, 3). According to Aste et al. (2) the frequency of relapse is related to uncontrolled predisposing factors. Indeed, P. aeruginosa does not persist on normal dry skin (11) and its overgrowth is facilitated by alteration of the stratum corneum, local humidity leading to over hydration of the stratum corneum (12), and suppression of the normal Gram-positive flora by antiseptics or antibiotics. Our data suggest that predisposing factors and diseases that damage the skin barrier and the local microbiota are frequently associated with GNTWI. Hyperhidrosis was infrequent, as in the work of Aste et al. (2); however, the fact that local occlusion and humidity (of professional or recreational causes) were found in almost half of the patients suggests the relevance of these factors.
Tinea pedis was frequently suspected and treated, but in most cases no dermatophyte was isolated. This may be due to recent application of antifungal agents or to production by P. aeruginosa of antifungals (10). Eczema, often of the dyshidrotic type, was frequently concomitantly or previously associated with GNTWI. The results of patch tests indicated sensitisation to shoe components and/or topical products. Indeed, contact dermatitis caused by application of multiple topical agents often precedes, and can cause predisposition to or aggravate, GNTWI. Moreover, hyperhidrosis and maceration, conditions frequently associated with GNTWI, promote sensitisation to shoe components. Aste et al. reported that 20% of GNTWI patients had preexisting contact dermatitis but they did not discuss the causative allergens (2). The high frequency of contact dermatitis suggests the need for systematic allergologic investigation in patients with GNTWI.
Vascular diseases, especially lymphoedema and venous insufficiency, may play a role in the development or maintenance of GNTWI because of bacterial colonisation of ulcers, maceration induced by bandages or oedema, impaired wound healing, and varicose eczema. In this study, cellulitis was most frequently associated with underlying vascular disorders.
Broad-spectrum antibiotics active against P. aeruginosa were applied less frequently compared to previous reports (2–4, 7, 13, 14) in which their use was proposed in refractory or severe cases; however, these terms were not defined. Use of broad-spectrum antibiotics for GNTWI, while rarely associated with systemic symptoms, requires rigorous evaluation because of the risk of acquisition of resistance by P. aeruginosa. Moreover, as broad-spectrum antibiotics are associated with local treatment and hospitalisation, isolating their benefits is difficult. In patients with cellulitis, antibiotics were mainly directed against S. aureus and β-haemolytic streptococci, indicating that the physician focused on treating the cellulitis rather than the GNTWI.
Follow-up of patients was insufficient and irregular, and one third of the patients were lost to follow-up. The patients with GNTWI frequently exhibited medical nomadism, non-compliance with the treatment regimen, and self-medication. The high frequency of persistence of interdigital anomalies during short-term follow up suggests the presence of an underlying disease (e.g. tinea pedis or eczema). Conversely, patients in whom predisposing or aggravating diseases or factors were controlled did not experience recurrence of GNTWI. The most frequent related conditions in these patients were inflammatory skin diseases, including psoriasis and eczema. Flare of an inflammatory skin disease was the factor most frequently associated with recurrence.
This study had several limitations. Firstly, as it used a retrospective design, the quality of the data depended on the completeness of the medical records. The total number of physicians consulted, reflecting medical nomadism and self-medication would have been an interesting data to assess because we have seen it as a frequent trend making management more complex. Missing data on psychological and social factors may have resulted in underestimation of negligence with respect to self-care, addictive behaviour, psychiatric conditions, and/or social drift, which may be related to the management of GNTWI. Similarly, we could evaluate the impact of employment category on GNTWI only in a portion of cases. However, to our knowledge, this is the first study to assess socio-professional factors.
To conclude, we suggest that the management of GNTWI be standardised, with a focus on predisposing diseases and conditions (Fig. 3). Improved follow-up, efforts to reduce medical nomadism and self-medication, education on hygiene measures, identification of social factors that complicate management and efforts to increase patient compliance are crucial for the management of GNTWI.
Fig. 3. Proposed management of patients with gram-negative toe-web infection (GNTWI).
We thank Drs F. Foulet, S. Ingen-Housz-Oro, F. Hemery, Henri-Mondor Hospital, AP-HP, Paris-Est University Créteil (UPEC), Créteil, France for their help in patients’ files selection or management.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize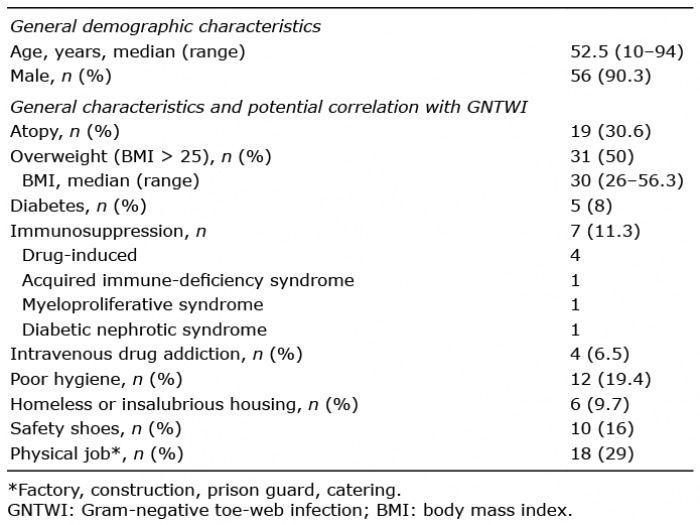 Click to show fullsize
Click to show fullsize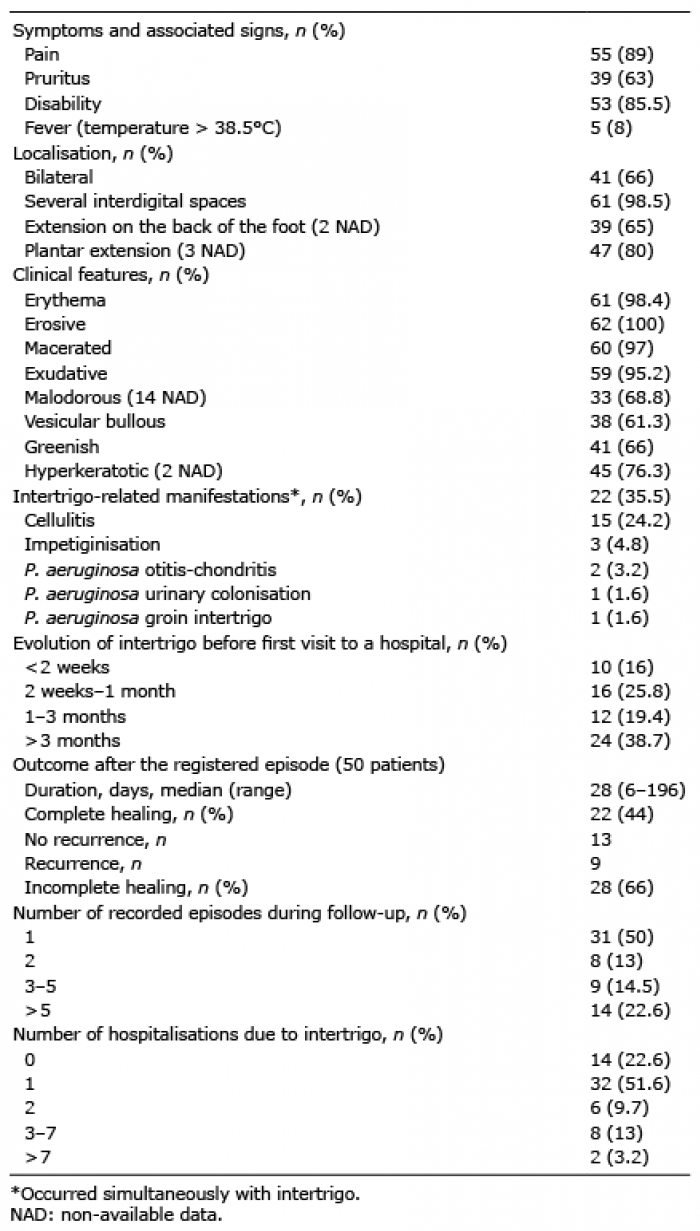 Click to show fullsize
Click to show fullsize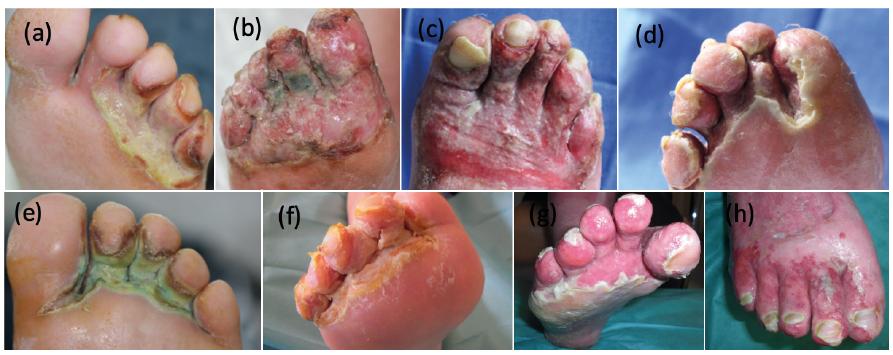 Click to show fullsize
Click to show fullsize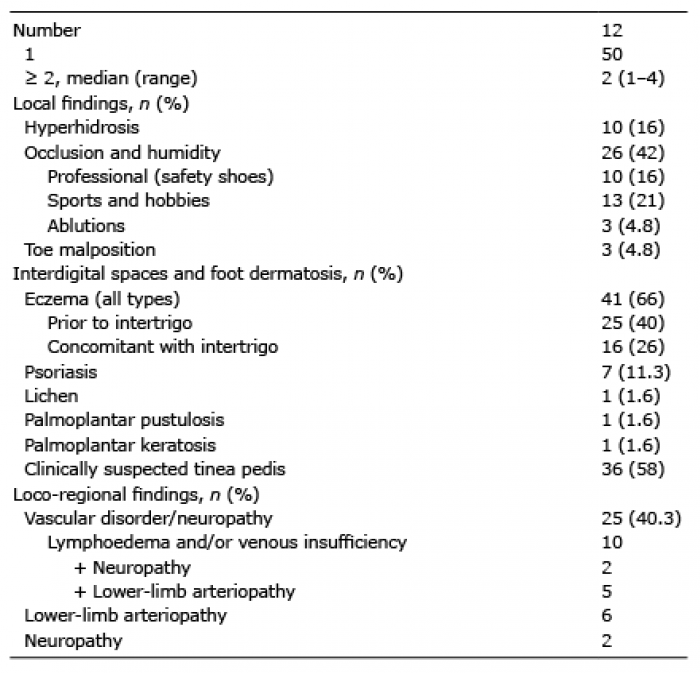 Click to show fullsize
Click to show fullsize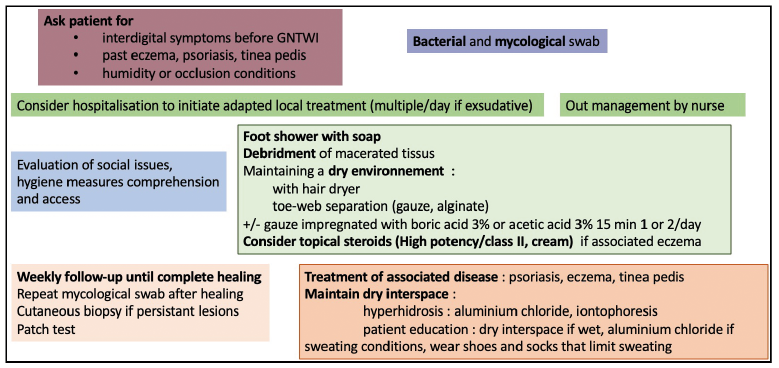 Click to show fullsize
Click to show fullsize